










Recently, Delphi consensus proposed an overarching term steatotic liver disease (SLD), with various subcategories such as MASLD, MetALD and ALD. Our aim was to investigate the association between MASLD/MetALD/ALD and four intrahepatic and extrahepatic diseases (liver diseases, renal diseases, cardiovascular diseases, and cancers) in the UK Biobank cohort.
Patients and MethodsBy defining hepatic steatosis as image-derived phenotype (IDP)-PDFF >5.21%, we used data from the UK Biobank to diagnose MASLD/ MetALD/ALD. The odd ratio (OR) and the hazard ratio (HR) were calculated using the logistic regression modals and Cox regression models, respectively.
ResultsAmong 39,230 eligible individuals, 6,865 MASLD subjects, 2,379 MetALD subjects and 884 ALD subjects were diagnosed. The last follow-up time was October 13, 2023. Consistent with the logistic analyses, MASLD/MetALD/ALD were significantly associated with a higher risk of liver diseases (HR=3.04 [95%CI:2.60-3.56], HR = 2.69 [95% CI: 2.12-3.42] and HR =3.99 [95%CI:2.92-5.45], respectively). Subjects with MASLD also had an increased higher risk of renal diseases (HR = 1.40 [95%CI:1.20-1.64]) and subjects with ALD had an increased higher risk of cancers (HR = 1.36 [95%CI:1.15-1.60]).
ConclusionIt is the first study to report the association between MASLD, MetALD, ALD and common intrahepatic and extrahepatic diseases based on magnetic resonance imaging data—PDFF. We found that MASLD, MetALD and ALD were risk factors for liver diseases. Meanwhile, MASLD was also a risk factor for renal diseases and ALD was a risk factor for cancers.
Nonalcoholic fatty liver disease (NAFLD) is a worldwide public health problem. NAFLD is one of the most important causes of chronic liver disease with its prevalence increasing over the past few decades [1,2]. NAFLD and resulting nonalcoholic steatohepatitis (NASH) are causes of hepatocellular cancer (HCC) and the main indications for liver transplantation [3–6]. Growing evidence also showed that NAFLD is a multi-system disease which can increase the risk of type 2 diabetes mellitus (T2DM), cardiovascular disease (CVD), chronic kidney disease (CKD) and and some extrahepatic cancers [7–10].
In 2020, a consensus group recommended replacing NAFLD/NASH with metabolic dysfunction-associated fatty liver disease (MAFLD), which can more accurately reflected the understanding of fatty liver diseases associated with metabolic dysfunction and make it possible to assess the interaction between alcohol consumption and metabolic risk factors [11,12]. Recently, 236 panelists from 56 countries used a representative, patient-centered Delphi process to systematically discuss all issues and perspectives. Finally, they reached new nominations and definitions through consensus [13]. This consensus introduced the term steatotic liver disease (SLD) as an umbrella term encompassing various causes of steatosis and decided to use metabolic dysfunction-associated steatotic liver disease (MASLD) to replace MAFLD/NAFLD [13,14]. Another term derived from MASLD is called metabolic and alcohol-related/associated liver disease (MetALD), which used to describe those with metabolic dysfunction-associated steatotic liver disease who consume more alcohol per week (140-350 g/week and 210-420 g/week for women and men, respectively). While alcohol-related liver disease (ALD) refers to liver damage caused by excessive alcohol consumption [15]. The Delphi consensus separates MASLD, MetALD, and ALD by alcohol intake.
Previous studies have shown that MASLD is almost similar to NAFLD in many aspects [16–24]. However, to our knowledge, the association of MASLD/MetALD/ALD with intrahepatic and extrahepatic diseases based on magnetic resonance imaging data—PDFF and large-scale cohort are not yet reported. Here, we evaluated the impact of MASLD, MetALD, and ALD on the risk of intrahepatic and extrahepatic outcomes in the UK Biobank cohort, with the aim of providing valuable information for clinical healthcare. Especially, we used imaging data (Proton Density Fat Fraction, PDFF) from UK Biobank to define MASLD, which is obviously more accurate than calculated index such as fatty liver index (FLI).
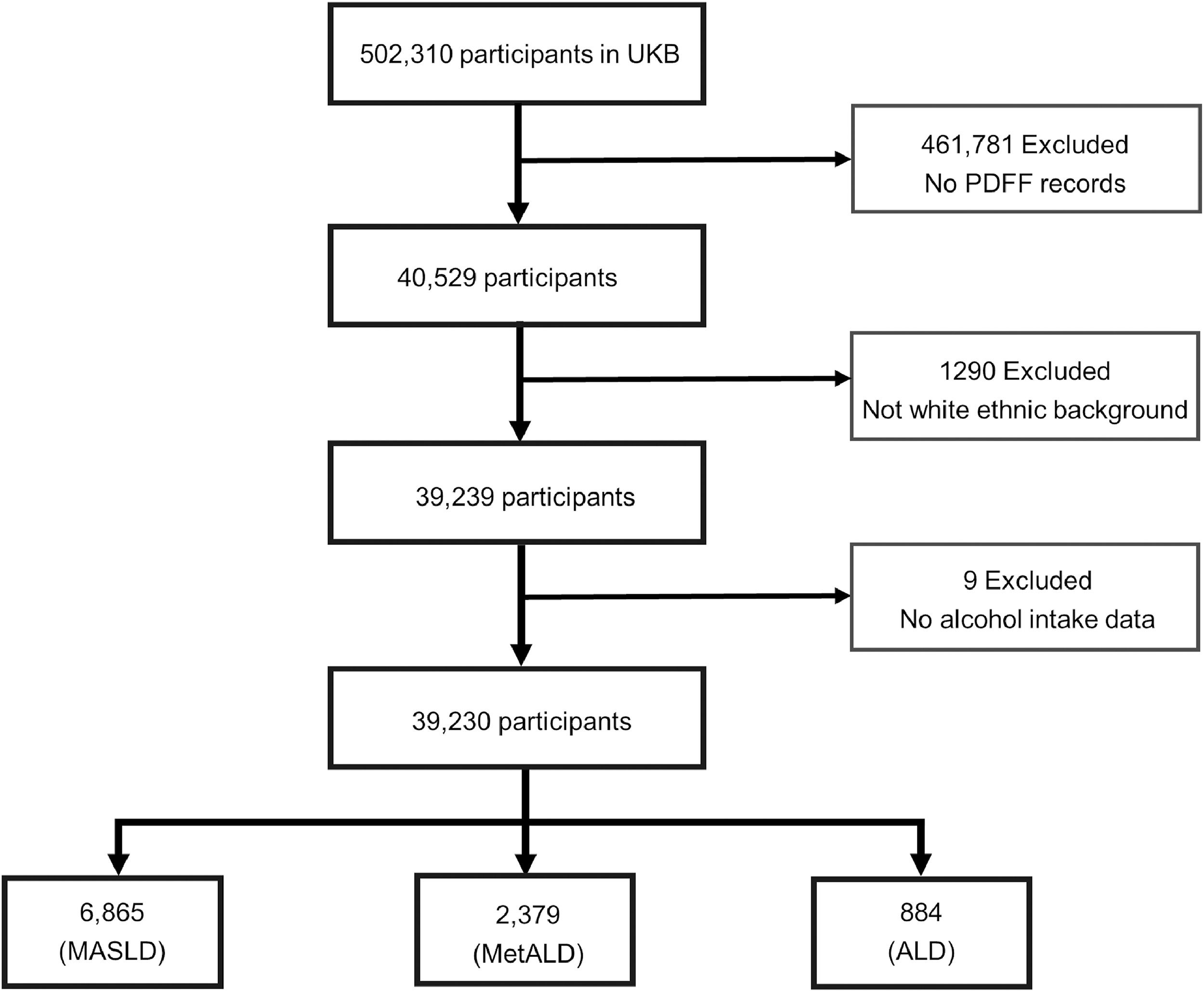
2Materials and Methods2.1Study populationThe UK Biobank is a large-scale, population-based prospective study that recruited 502,000 adults aged 40-69 years from the UK general population between 2006 and 2010, with deep phenotyping and genomic data [25]. We excluded participants of non-white ethnic and individuals who lacked data for PDFF records and alcohol intake (Fig. 1). Finally, 39,230 individuals with image-derived phenotype (IDP) from the UK Biobank were included. Of which, 6,865 were diagnosed as MASLD, 2,379 were diagnosed as MetALD and 884 were diagnosed as ALD (Table 1).

Characteristics of eligible participants.
MASLD, metabolic dysfunction-associated steatotic liver disease; MetALD, metabolic and alcohol-related/associated liver disease; ALD, alcohol-related liver disease; BMI, body mass index; MET, metabolic equivalent task; HDL, high-density lipoprotein; PDFF, proton density fat fraction.
We defined MASLD as the presence of hepatic steatosis in conjunction with at least one cardiometabolic risk factor (CMRF) and low alcohol intake (less than 140 g/week for females and less than 210 g/week for males). MetALD was defined as hepatic steatosis, at least one cardiometabolic factor and moderate alcohol intake (140 to 350 g/week for females and 210 to 420 g/week for males), ALD was defined as hepatic steatosis, at least one cardiometabolic factor and excessive alcohol intake (more than 350 g/week for females and more than 420 g/week for males) [25–27].
We used an IDP—Proton Density Fat Fraction (PDFF) >5.21% to define the hepatic steatosis [28,29]. The cardiometabolic risk factors (CMRF) including: (1) body mass index ≥25 kg/m2 (23 for Asians) or waist circumference >94 cm (males) or 80 cm (females) or ethnicity adjusted; (2) fasting serum glucose ≥5.6 mmol/L (100 mg/dL) or 2-hour post-load glucose levels ≥7.8 mmol/L (≥140 mg/dL) or hemoglobin A1c ≥5.7% (39 mmol/L) or type 2 diabetes or treatment for type 2 diabetes; (3) blood pressure ≥130/85 mmHg or specific antihypertensive drug treatment; (4) plasma triglyceride level ≥1.70 mmol/L (150 mg/dL) or lipid-lowering treatment; (5) plasma high-density lipoprotein-cholesterol ≤1.0 mmol/L (40 mg/dL males) and ≤1.3 mmol/L (50 mg/dL females) or lipid-lowering treatment [13,26].
Alcohol intake was calculated based on ABV (the alcohol by volume) of various alcohol types. The alcohol content was 15.625g, 22.72g, 15.625g, 11.5625g, and 12g per standard drink, respectively for red wine, beer, champagne plus white wine, fortified wine, and spirits [30].
2.3Outcomes dataWe evaluated the associations of MASLD, MetALD, ALD with four intrahepatic and extrahepatic diseases outcomes (liver diseases, renal diseases, cardiovascular diseases, and cancers). The diseases outcomes were defined by the International Classification of Diseases-Tenth Revision codes (ICD-10) (Table S1). Specifically, in UK Biobank, the ICD-10 codes for liver diseases were B18.x, C22.x, K70.x–K77.x, and Z94.4. For renal diseases, the codes were I12.0, I13.1, N03.2–N03.3, N03.5–N03.7, N05.2–N05.7, N18.x–N19.x, N25.0, Z49.x, Z94.0, and Z99.2. For cardiovascular diseases, the codes were I09.9, I11.0, I13.0, I13.2, I21.x–I22.x, I25.2, I25.5, I42.0, I42.5–I42.9, I43.x, and I50.x. For cancers, the codes were C00.x–C97.x. A more detailed description of the coding algorithms that define diseases outcomes in the UK Biobank's ICD-10 administrative data can be found in Table S3.
2.4Statistical analysesContinuous and categorical variables were described with mean ± SD and count (%), respectively. Logistic regression analyses were used to assess the association of MASLD/MetALD/ALD with the morbidity of four intrahepatic and extrahepatic diseases (liver diseases, renal diseases, cardiovascular diseases, and cancers). Cox proportional hazards regression analyses were used to assess the association of MASLD/MetALD/ALD with time to diagnosis of four intrahepatic and extrahepatic diseases (liver diseases, renal diseases, cardiovascular diseases, and cancers). We constructed two types of logistic regression models and Cox proportional hazards regression models, respectively. One type of model was univariate model without adjusting covariates. Another was multivariate model with adjusting sex and age at recruitment. Statistical analyses were performed using SAS 9.4 and R statistical software version 4.3.0.
2.5Ethical statementsUK Biobank has approval from the North West Multi-centre Research Ethics Committee (MREC) as a Research Tissue Bank (RTB) approval, which means we do not require separate ethical clearance.
3Results3.1Characteristics of study participantsAmong 39,230 eligible individuals, 6,865 MASLD subjects, 2,379 MetALD subjects and 884 ALD subjects were diagnosed. The mean (SD) age of all individuals was 55.12 (7.51) years. Slightly difference of mean age were found among MASLD (55.58 years), MetALD (54.90 years), ALD (54.35 years), and other (55.05 years) individuals. The proportion of male in MASLD, MetALD, and ALD subjects were 56.46%, 65.20% and 79.19%, respectively. Subjects with MetALD and ALD were more likely to be smokers. Three indicators for liver function (ALT, AST, GGT) increased successively in MASLD, MetALD and ALD individuals, and were all higher than other individuals. Proportion of subjects were diagnosed with liver diseases, renal diseases, cardiovascular diseases and cancers were shown in Fig. 2 (Fig. 2, Table S2).
 Proportion of MASLD subjects with four intrahepatic and extrahepatic diseases. (b) Proportion of MetALD subjects with four intrahepatic and extrahepatic diseases. (c) Proportion of ALD subjects with four intrahepatic and extrahepatic diseases. (d) Proportion of other subjects with four intrahepatic and extrahepatic diseases.")
Proportion of subjects with four intrahepatic and extrahepatic diseases. MASLD, metabolic dysfunction-associated steatotic liver disease; MetALD, metabolic and alcohol-related/associated liver disease; ALD, alcohol-related liver disease. (a) Proportion of MASLD subjects with four intrahepatic and extrahepatic diseases. (b) Proportion of MetALD subjects with four intrahepatic and extrahepatic diseases. (c) Proportion of ALD subjects with four intrahepatic and extrahepatic diseases. (d) Proportion of other subjects with four intrahepatic and extrahepatic diseases.
By using logistic regression analyses, we found that all three hepatic steatosis status (MASLD, MetALD and ALD) were significantly associated with the risk of liver diseases (OR = 2.97 [95% CI:2.55-3.46], OR = 1.65 [95% CI:1.47-1.86] and OR = 1.55 [95% CI:1.39-1.72], respectively). However, only subjects with MASLD was significantly associated with a higher risk of renal diseases (OR = 1.42 [95% CI:1.21-1.66]) and only subjects with ALD was significantly associated with a higher risk of cancers (OR = 1.07 [95% CI: 1.01-1.14]). Besides, all three hepatic steatosis status were associated with a higher risk of CVD in the unadjusted model (OR = 1.31 [95% CI: 1.16-1.48] for MASLD, OR =1.17 [95% CI:1.07-1.29] for MetALD and OR = 1.15 [95% CI:1.04-1.27] for ALD, respectively) but only MASLD achieved a p value less than 0.05 in the adjusted model (OR = 1.15 [95% CI: 1.01-1.30]) (Table 2).
Odds ratios (ORs) with 95% confidence intervals(CI) from logistic regression analyses for four intrahepatic and extrahepatic diseases.
The adjusted covariates were: age and sex. MASLD, metabolic dysfunction-associated steatotic liver disease; MetALD, metabolic and alcohol-related/associated liver disease; ALD, alcohol-related liver disease.
The last follow-up time for this study was October 13, 2023. By using Cox regression analyses, we found that all three hepatic steatosis status (MASLD, MetALD and ALD) were significantly associated with a higher risk of liver diseases (HR=3.04 [95%CI:2.60-3.56], HR = 2.69 [95% CI: 2.12-3.42] and HR =3.99 [95%CI:2.92-5.45], respectively). However, only subjects with MASLD had an increased higher risk of renal diseases (HR = 1.40 [95%CI:1.20-1.64]) and only subjects with ALD had an increased higher risk of cancers (HR = 1.36 [95%CI:1.15-1.60]). Consistent with the logistic analyses, all three hepatic steatosis status had an increased excess risk of CVD in the unadjusted model (HR = 1.23 [95%CI:1.08-1.40], HR = 1.33 [95%CI:1.10-1.62] and HR =1.47 [95%CI:1.09-1.97], respectively) but none achieved a p vlaue less than 0.05 in the adjusted model (Table 3, Fig. 3).
Hazard Ratios (HRs) with 95% confidence intervals(CI) from Cox regression analyses for four intrahepatic and extrahepatic diseases.
The adjusted covariates were: age and sex. MASLD, metabolic dysfunction-associated steatotic liver disease; MetALD, metabolic and alcohol-related/associated liver disease; ALD, alcohol-related liver disease.

The association of MASLD, MetALD, and ALD with four intrahepatic and extrahepatic diseases in the UK Biobank cohort. The hazard ratios were obtained from Cox regression model with the other subjects as reference group. The Cox regression model was adjusted for sex and age. MASLD, metabolic dysfunction-associated steatotic liver disease; MetALD, metabolic and alcohol-related/associated liver disease; ALD, alcohol-related liver disease.
In this study, we explored the association of MASLD/MetALD/ALD with four intrahepatic and extrahepatic diseases. As expected, we found that all three hepatic steatosis status (MASLD/MetALD/ALD) were significantly associated with a higher risk of liver diseases. However, either in the logistic regression analyses or in the Cox regression analyses, only MASLD was significantly associated with a higher risk of renal diseases and only ALD was significantly associated with a higher risk of cancers. To our knowledge, this is the first study to investigated the association between MASLD, MetALD, ALD and common intrahepatic and extrahepatic diseases based on imaging data—PDFF.
For liver diseases outcomes, subjects with ALD exhibited the highest risk, followed by MASLD and then MetALD. We speculate that this could be attributed to the fact that ALD subjects have the highest alcohol intake. Studies have shown that ALD is one of the most common causes of liver-related morbidity [31], which is consistent with our findings. Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) are commonly utilized liver biomakers in measuring liver dysfunction [32]. The baseline levels of AST and ALT in MASLD, MetALD, and ALD subjects increased sequentially and all were higher than other subjects. But ALT levels may increase when using certain medications or during strenuous exercise. AST occurs in two isoenzymes, and it is difficult to distinguish whether it occurs in hepatocytes in standard AST assays. Caution should be exercised when using these two biomarkers [32]. Inamine et al. reported that MAFLD was independent factor for significant/advanced liver fibrosis in patients with morbid obesity, which were in line with our findings [33]. Studies have shown that obesity was not only associated with simple steatosis, but also with advanced liver disease [34]. In terms of diagnostic criteria, MASLD, MetALD and ALD all have hepatic steatosis and at least one cardiometabolic factor. Metabolic abnormalities/disorders may be responsible for the increased risk of liver diseases.
For renal diseases outcomes, we identified MASLD as a risk factor. A recent study has found that MASLD was associated with an increased risk of chronic kidney disease (CKD), which was consistent with our findings [35]. But their study defined hepatic steatosis based on ultrasound. Our definition was based on a magnetic resonance imaging data—PDFF, which had better sensitivity compared with ultrasound [35]. As reported, a complex combination of metabolic and hemodynamic changes, lipid nephrotoxicity, and genetic predisposition may drive the development of CKD in patients with NAFLD [36]. A meta-analysis showed that luseogliflozin, a sodium-glucose cotransporter 2 inhibitor, improved various cardiometabolic risk factors and may improve MASLD in diabetic patients [37]. Therefore, it is worth exploring whether SGLT2 inhibitor play a positive role on liver diseases and renal diseases.
For cardiovascular diseases outcomes, the definition of MASLD includes at least one risk factor for CVD, which implies that patients with MASLD are at an increased risk of cardiovascular disease (CVD) [38]. Basing on the fatty liver index (FLI), studies have found that MASLD increased the risk of CVD [39,40]. MAFLD could predict the progression of atherosclerotic cardiovascular risk [41,42]. In our analyses, we found that only MASLD was associated with a higher risk of CVD in the adjust logistic regression. It is important to note that our study strictly adhered to the Delphi consensus, using imaging data—PDFF to define hepatic steatosis, which made our study more reliable. Ruttmann E et al. found that gamma-glutamyl transferase (GGT) is a risk factor for cardiovascular disease (CVD) [43]. High GGT was significantly associated with overall CVD mortality and showing a clear dose-response relationship. In our study, the GGT index of subjects with MASLD, MetALD, and ALD increased sequentially and were all higher than other subjects.
For cancers outcomes, we found that ALD is a risk factor for cancers and remained significant after adjusting for age and sex. Considering that smoking is involved in the development of cancers, we included smoking status as a covariate along with age and sex, and the association remained significant (OR = 1.26 [95%CI:1.05-1.51], HR = 1.33 [95%CI:1.12-1.57]) . At the same time, we did not find a risk association between MASLD/MetALD and cancer. A review suggested that drinking alcohol can increase the risk of several types of cancer, such as cancers of the upper aerodigestive tract, liver, colorectum, and breast [44]. As the diagnostic criteria mentioned earlier, ALD subjects exhibit the highest alcohol intake. Therefore, excessive alcohol intake may be a contributing factor to the increased cancers risk in ALD subjects. Previous studies have focused on the associations between NAFLD/MAFLD and various conditions, including pancreatic cancer, gastric cancer, esophageal cancer,and reflux esophagitis [45–48]. Most of them concentrated on specific cancer outcomes, whereas ours focused on pan-cancer analysis.
Our study has two advantages. First of all, the UK Biobank is a very large, prospective cohort and the imaging data from UK biobank made our study possible and reliable. Secondly, this study used imaging data—PDFF for the diagnosis of hepatic steatosis, which strictly adhered to the new definition of the Delphi consensus. At the same time, there are some limitations we need to consider. Firstly, only white ethnic was included in our study, which limits the generalization of our results to other ethnicities. Secondly, we selected the PDFF threshold provided by the Wilman HR study to diagnose hepatic steatosis, however, additional research is required to predict PDFF with higher accuracy [28].
5ConclusionsOur findings demonstrated that all three hepatic steatosis status (MASLD, MetALD and ALD) are risk factors for liver diseases. In addition, MASLD is also a risk factor for renal diseases and ALD is a risk factor for cancers.
Authors contributionsYX: writing—original draft preparation, writing—review and editing, visualization. WH: conceptualization, methodology, formal analysis, visualization. JH: methodology, formal analysis. SX: data curation. DJ: resources, supervision. RN: resources, project administration, funding acquisition. ZY: resources, supervision. JZ: data curation, writing—original draft preparation, project administration. HC: conceptualization, data curation, writing—review and editing, project administration, funding acquisition.
FundingThis work was supported by the National Key R&D Program of China (2023YFC2307004) to Haitao Chen, Shenzhen-Hong Kong-Macau Science and Technology Program (Category C; SGDX20220530111403024) to Haitao Chen and Rong Na, the National Natural Science Foundation of China (NSFC, 82272312) to Haitao Chen, the 100 Top Talent Programs of Sun Yat-sen University (58000-12230029) to Haitao Chen. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplementary Fig1. The Kaplan-Meier curve for all outcomes in patients with MASLD/MetALD/ALD. The y axis is cumulative incidence.
Supplementary Fig2. The Kaplan-Meier curve for all outcomes in patients with MASLD/MetALD/ALD. The y axis is survival probability.
The authors thank the National Key R&D Program of China (2023YFC2307004), Shenzhen-Hong Kong-Macau Science and Technology Program (Category C; SGDX20220530111403024), the National Natural Science Foundation of China (NSFC, 82272312), and the 100 Top Talent Programs of Sun Yat-sen University (58000-12230029)




{kind=link}
{kind=link}