





To quantify the long-term impact (24 months) on the visual results and activity of neovascular lesions of COVID-19 confinement in patients with nAMD in our population.
MethodsA retrospective observational study of patients with nAMD who attended consultation or were treated during the 3 months before confinement was carried out.
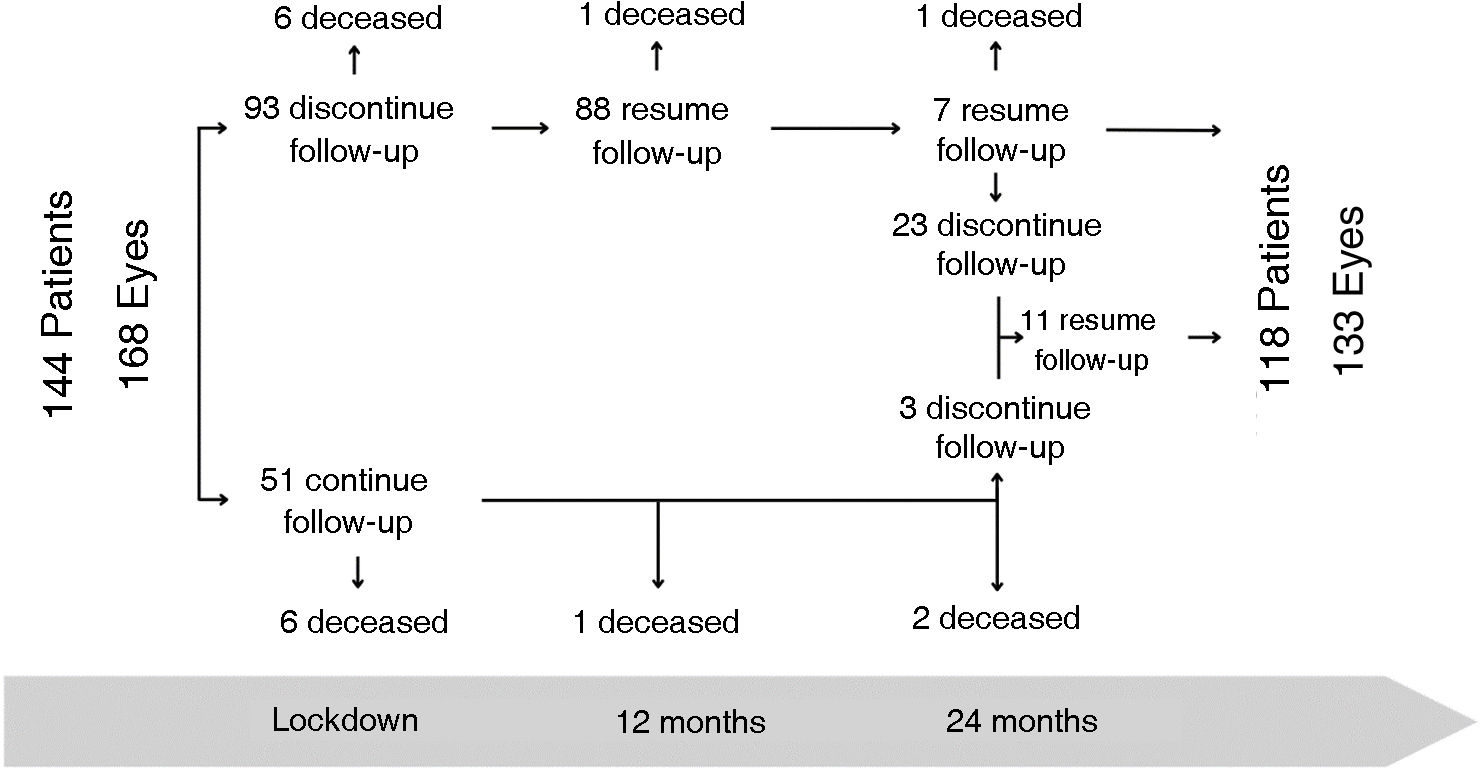
Results144 patients (168 eyes) with nAMD were included, 51 of them (35.42%) came during confinement, and at 24 months the final cohort was 118 patients (133 eyes).
The previous VA of 57.99 ± 23.68 letters decreased, clinically relevant and statistically significant, by an average of 6.87 (±16.84) and 7.89 (±19.58) at 12- and 24-months follow-up. This change differs significantly from the two-year vision change observed in the national database of pretreated patients.
The median number of injections and consultations is lower in our group at 12 months, compared to the pre-pandemic national database, and tends to equalize at 24 months.
We did not find differences in vision when we compared patients who attended consultations during confinement or in treatment intervals greater than 8 weeks (Tq8w).
ConclusionsThe VA of patients with nAMD decreased significantly after confinement, probably due to the lower number of antiangiogenic injections and consultations during the first year, and did not recover during the second year despite the increase in the number of injections and visits close to those reported before confinement.
El objetivo de este trabajo es cuantificar el impacto a largo plazo (24 meses) en los resultados visuales y la actividad de las lesiones del confinamiento por COVID-19 en pacientes con DMAEn en nuestra población.
MétodosEstudio observacional retrospectivo de pacientes con DMAEn que acudieron a consulta o fueron tratados durante los 3 meses previos al confinamiento.
ResultadosSe incluyeron 144 pacientes (168 ojos) con DMAEn, 51 de ellos (35,42%) acudieron durante el confinamiento, a los 24 meses la cohorte final es de 118 pacientes (133 ojos).
La AV previa de 57,99 ± 23,68 letras, disminuyó una media de 6,87 (±16,84) y 7,89 (±19,58) letras a los 12 y 24 meses de seguimiento (p < 0,001). Este cambio difiere significativamente al cambio de visión a dos años observado en la base de datos nacional de pacientes pretratados.
La mediana de inyecciones y consultas es menor en nuestro grupo a los 12 meses, comparado con la base de datos nacional prepandemia y tiende a igualarse a los 24.
No encontramos diferencias en la visión cuando comparamos los pacientes que acudieron a las consultas durante el confinamiento ni en los intervalos de tratamiento superiores a 8 semanas (c8s).
ConclusionesLa AV de los pacientes con DMAEn disminuyó significativamente tras el confinamiento, probablemente debido al menor número de inyecciones de antiangiogénicos y consultas durante el primer año, y no se recuperó durante el segundo año pese al aumento del número de inyecciones y visitas en cifras cercanas a las reportadas antes del confinamiento.
The COVID-19 pandemic had a major impact on healthcare systems, the world's population was placed in lockdown and for the first and only time, non-emergency medical treatment was universally discontinued.1
The first case of COVID-19 was diagnosed in Spain on January 31, 2020. A national containment was imposed on March 14 and continued until June 21.2 To curb viral transmission, public health measures were implemented including a decrease in clinical activity, which associated with fear of the disease and social and institutional isolation1 limited healthcare to the extent that non-urgent outpatient care in Ophthalmology services was reduced by more than 50%.3
Age-related macular degeneration (AMD) is the leading cause of blindness in developed countries4,5 and its neovascular form (nAMD) is seen in approximately 15–20% of advanced cases.6 It is effectively treated with intravitreal injections (IVT) of antiangiogenic drugs (AAG) in different patterns.7 One of the most commonly used regimens is to treat and extend,6 and in some centers such as ours, treatment can be discontinued after long periods of inactivity, with quarterly check-ups without treatment. Good compliance is essential to maximize the benefits of treatment and it has been shown that delays in the administration of injections have a negative impact on visual acuity (VA).8,9
The short- to medium-term consequences of reducing or suppressing AAG treatment during the COVID-19 pandemic have been studied in terms of both VA changes and lesion activity.10–21 It has been shown that patients with nAMD had greater VA loss than patients treated for other diseases such as retinal venous obstruction (RVO) or diabetic macular edema (DME) (loss of five ETDRS letters in nAMD versus one letter in RVO or DME).12 And also that the effect of COVID-19 was different in different countries; as there were differences in length of lockdown, dropout rates and activity in IVT units. In countries with short lockdowns, where IVT injections were maintained, the decrease in VA was less than in those where activity was completely stopped or which had long lockdowns.19,22 Dropout rates varied between countries, from 7% (Ireland) to 32% (Spain), and the most frequent reason for dropout in Spain was "medical protection" for fear of contracting COVID-19, followed by "death" and "hospital transfer" for various reasons, including changes in health insurance policies.23
After lockdown, normal follow-up and treatment activity was reinstated with variable speed, and even higher in some studies20,21 in the IVT treatment units in an attempt to recover vision loss. The authors’ center implemented a series of measures to facilitate adherence to treatment such as an increase in simultaneous treatments and the reintroduction of a loading schedule for active patients, among others.
Short-term studies to determine the effect of lockdown in patients with nAMD tested the change in VA at three to six months pre-pandemic versus three to six months post-pandemic,22 finding a statistically significant decrease in best-corrected VA (BCVA) related to a reduction in the number of follow-up visits and IVT injections.16,19 In medium-term studies (12 months),21 they found a visual loss at one year post-pandemia greater than what they considered attributable to the natural evolution of treated nAMD.21 This approach may be useful for short time periods (six to 12 months), but is not valid for long periods, as it induces biases and changes in VA in patients with nAMD are not linear over time.24 To compare the two-year results of our cohort (COVID-19 period cohort) we will use a historical cohort of previously treated patients collected nationally as of February 2018 (two years prior to the pandemic) that tells us the natural evolution of nAMD in our setting (non-COVID-19 period cohort).24
The aim of this work is to quantify the long-term impact (24 months) on visual outcomes and lesion activity of COVID-19 lockdown in patients with nAMD in our population, and compare it with actual 2-year clinical practice data in the national population studied during the 2 years prior to the pandemic.24 In this way, we decreased comparison biases and assessed the extent to which post-pandemic efforts reversed visual loss, or whether it was irreversible.
A stratified study of subgroups was also performed to see if the effect was equal in those patients who had periods of extension between AAG IVT treatment longer than two months and in those who did come for treatment during lockdown.
MethodsWe proposed a retrospective observational study of all consecutive patients with nAMD who attended AMD consultation or had been treated with AAG for nAMD at our center in the three months prior to the start of lockdown. All patients signed an informed consent to participate in the study, which followed the guidelines of the Declaration of Helsinki. The protocol was approved by the Medical Research Ethics Committee of the Hospital Universitario Príncipe de Asturias with number OE 01/2021.
The primary objective of the present study is to measure the long-term impact on visual outcomes and lesion activity of AMD patients in our area with the safety measures we implemented during the lockdown and in the following two years, and to compare it with the results obtained in real clinical practice in Spain during the years prior to lockdown.
The number of consultations and injections, change in VA and neovascular membrane (NVM) activity were analyzed at five time points: six months before lockdown and at six, 12, 18 and 24 months after lockdown.
The SPSS 20.0 program (IBM, Armonk, United States) was used for statistical analysis. A descriptive analysis was performed, obtaining the mean, standard deviation (SD) and median of the quantitative variables and the percentage of the qualitative variables. For comparisons the t for Student test was used for unpaired samples; frequency distributions were compared using the X test2 or Fisher's exact test, as appropriate. Values of p < 0.05 were considered significant.
ResultsDemographic characteristics and patient flow during the two yearsBetween December 1, 2019 and March 13, 2020, a total of 144 patients with nAMD attended AMD consultation or received IVT treatment. The majority had unilateral involvement (83.33%) and only 24 patients had bilateral involvement (168 eyes with nAMD). The mean age was 79.06 ± 7.58 years and 54.86% were women. Of the total number of patients, 51 (35.42%) attended during lockdown. The flow of patients over the two years is illustrated in Fig. 1.

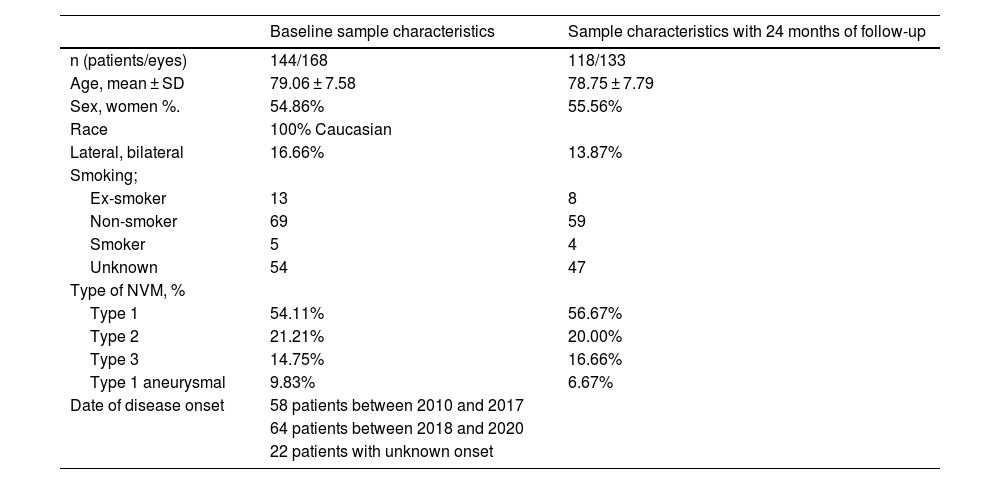
The final cohort comprised 118 patients (81.94%) and 133 eyes, with a mean age of 78.75 ± 7.79 years, of which 55.56% were women. The demographic characteristics at baseline and at 24 months follow-up are shown in Table 1.
Demographic characteristics of the sample at baseline and at 24 months of follow-up.
| Baseline sample characteristics | Sample characteristics with 24 months of follow-up | |
|---|---|---|
| n (patients/eyes) | 144/168 | 118/133 |
| Age, mean ± SD | 79.06 ± 7.58 | 78.75 ± 7.79 |
| Sex, women %. | 54.86% | 55.56% |
| Race | 100% Caucasian | |
| Lateral, bilateral | 16.66% | 13.87% |
| Smoking; | ||
| Ex-smoker | 13 | 8 |
| Non-smoker | 69 | 59 |
| Smoker | 5 | 4 |
| Unknown | 54 | 47 |
| Type of NVM, % | ||
| Type 1 | 54.11% | 56.67% |
| Type 2 | 21.21% | 20.00% |
| Type 3 | 14.75% | 16.66% |
| Type 1 aneurysmal | 9.83% | 6.67% |
| Date of disease onset | 58 patients between 2010 and 2017 | |
| 64 patients between 2018 and 2020 | ||
| 22 patients with unknown onset | ||
SD: standard deviation; NVM: neovascular membrane.
Table 2 shows the changes in VA, number of consultations and injections during follow-up. At 12 months we found a VA loss of 6.87 (±16.84) letters that was maintained during the second year, although the loss between the first and second year was lower. At 12-month follow-up 30 patients (20.83%) had lost ≥15 letters of VA and seven (4.86%) had gained ≥15 letters. At 24 months, 32 patients (22.22%) had lost ≥15 letters and eight (5.55%) had gained ≥15 letters.
Changes in VA, expressed as the logarithm of ETDRS letters, number of visits and IVT injections.
| Mean ± SD | Six months prior | Lockdown | Pa | Six months | pb | Six to 12 months | pc | 12−18 months | pd | 18−24 months | pe |
|---|---|---|---|---|---|---|---|---|---|---|---|
| VA | 57.99 ± 23.68 | – | – | 53.03 ± 27.14 | 0.001 | 53.06 ± 26.28 | < 0.0001 | 53.16 ± 26.28 | 0.002 | 50.49 ± 26.60 | 0 |
| Average change in VA | −6.87 (± 16.84) | −7.89 (±19.58) | |||||||||
| Number of Consultations | 2.72 ± 0.87 | 0.27 ± 0.53 | 0.001 | 1.91 ± 0.88 | 0.02 | 2.76 ± 1.01 | 0.898 | 2.34 ± 0.77 | < 0.0001 | 2.17 ± 0.75 | < 0.001 |
| Anti-VEGF IVT | 2.35 ± 3.02 | 0.33 ± 0.56 | 0.001 | 1.42 ± 1.47 | 0.001 | 2.85 ± 1.51 | 0.585 | 3.59 ± 1.68 | 0.232 | 3.02 ± 1.57 | 0.363 |
VA: visual acuity; anti-VEGF - anti vascular endothelial growth factor (anti-vascular endothelial growth factor).
P significance level for multiple comparisons (p < 0.025).
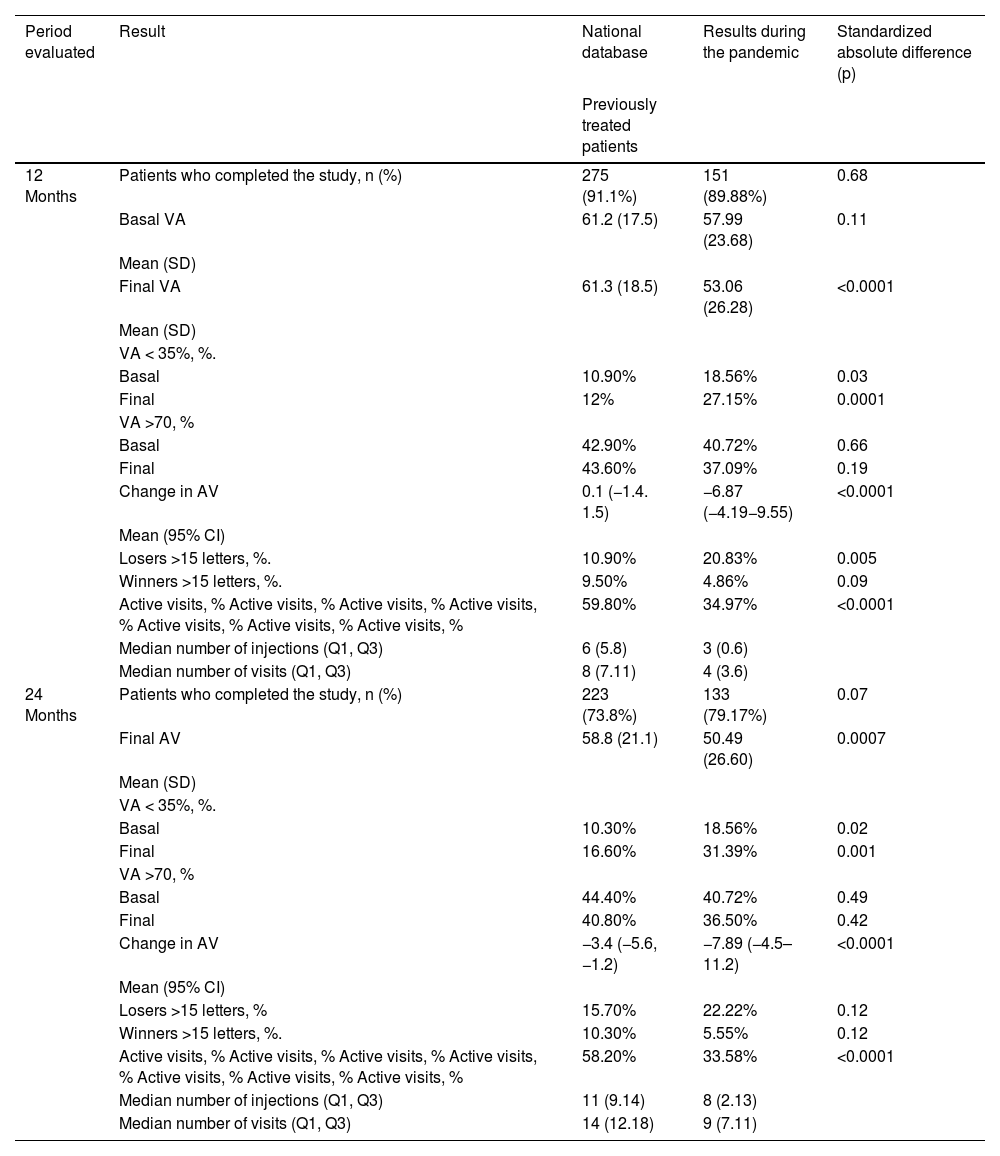
Statistically significant differences were observed in final VA and changes in VA at 12 and 24 months of follow-up, comparing the results of the national database with our results.
The median number of injections and consultations is lower in our group compared to the national database, which is higher at 12 months and tends to equalize at 24.
Changes in lesion activity during follow-upBefore lockdown, 43.71% of the NVM were active; the percentage decreased to 34.97%; 34.78%; and 33.58% at 12, 18, and 24 months, respectively. If we stratify the groups in those who continued follow-up during lockdown (51 patients) we observe that at 12 months of follow-up there was NVM activity in 50% of the cases and it decreased to 46.3% at 24 months. Meanwhile, in the group of patients who discontinued follow-up, there was only 36.14% active NVM at one year, while at 24 months, it decreased to 24.10%.
Subgroup analysisPatients with extension patterns greater than, less than or equal to eight weeks and patients who maintained consultations or injections during lockdown.
DiscussionDuring the 24-month follow-up there is a statistically significant and clinically relevant decrease (almost 10 ETDRS letters) in mean VA among AMD patients who experienced the COVID-19 pandemic period versus those who did not, even though median AAG injections reached values close to pre-pandemic and the percentage of active lesions decreases significantly. There are several studies of the impact of the COVID-19 pandemic on ophthalmic practice.10,25
The mean VA decline during the first year in our sample (-6.87 letters) is higher than that reported by other studies, 4.7 letters18 and 4.1.19 This may be because the populations of those studies were selected excluding patients with low VA (VA of counting fingers in the former and VA < 40 ETDRS letters in the latter) so the mean VA before lockdown was higher in both samples than in ours (67.2 and 60.5 versus 57.99).20 To our knowledge, there are no 24-month follow-up studies.
The percentages of gainers/losers of ≥15 letters at 24 months in the non-COVID period were 10.3%/15.7%,24 whereas in the COVID period they were significantly different, 5.55%/22.22%. The high percentage of patients losing at least 15 letters of VA during the COVID period may be related to the decrease in the number of AAG visits and injections during lockdown. Neither the loss of VA nor the increase in the percentage of patients losing more than 15 letters normalized during the second year despite the fact that the number of injections and visits was similar to that of the non-COVID period. In this regard, studies conducted before the pandemic showed that patients lost to follow-up for a mean period of 346 ± 122 days experienced an irreversible loss of VA, which was not recovered after additional AAG treatment despite anatomical improvement of the lesions.26
AMD patients are elderly with comorbidities and were particularly affected by limited access to medical care.17,22 Despite efforts to reduce COVID-19 infections, a significant decrease in the administration of IVT therapies was observed in highly endemic areas.18
In the prepandemic period, the median number of injections/visits at 12 months was 6/8 and at 24 months 11/14.24 In our study there is a median of 3/4 at 12 months and 8/9 at 2-year follow-up. We considered the decrease attributable to treatment abandonment and follow-up during lockdown. It is also noteworthy that in the second year of follow-up the number of injections is closer to those of prepandemic studies (Table 3).24
Comparison with patients in the national database at one and two years of follow-up.
| Period evaluated | Result | National database | Results during the pandemic | Standardized absolute difference (p) |
|---|---|---|---|---|
| Previously treated patients | ||||
| 12 Months | Patients who completed the study, n (%) | 275 (91.1%) | 151 (89.88%) | 0.68 |
| Basal VA | 61.2 (17.5) | 57.99 (23.68) | 0.11 | |
| Mean (SD) | ||||
| Final VA | 61.3 (18.5) | 53.06 (26.28) | <0.0001 | |
| Mean (SD) | ||||
| VA < 35%, %. | ||||
| Basal | 10.90% | 18.56% | 0.03 | |
| Final | 12% | 27.15% | 0.0001 | |
| VA >70, % | ||||
| Basal | 42.90% | 40.72% | 0.66 | |
| Final | 43.60% | 37.09% | 0.19 | |
| Change in AV | 0.1 (−1.4. 1.5) | −6.87 (−4.19−9.55) | <0.0001 | |
| Mean (95% CI) | ||||
| Losers >15 letters, %. | 10.90% | 20.83% | 0.005 | |
| Winners >15 letters, %. | 9.50% | 4.86% | 0.09 | |
| Active visits, % Active visits, % Active visits, % Active visits, % Active visits, % Active visits, % Active visits, % | 59.80% | 34.97% | <0.0001 | |
| Median number of injections (Q1, Q3) | 6 (5.8) | 3 (0.6) | ||
| Median number of visits (Q1, Q3) | 8 (7.11) | 4 (3.6) | ||
| 24 Months | Patients who completed the study, n (%) | 223 (73.8%) | 133 (79.17%) | 0.07 |
| Final AV | 58.8 (21.1) | 50.49 (26.60) | 0.0007 | |
| Mean (SD) | ||||
| VA < 35%, %. | ||||
| Basal | 10.30% | 18.56% | 0.02 | |
| Final | 16.60% | 31.39% | 0.001 | |
| VA >70, % | ||||
| Basal | 44.40% | 40.72% | 0.49 | |
| Final | 40.80% | 36.50% | 0.42 | |
| Change in AV | −3.4 (−5.6, −1.2) | −7.89 (−4.5–11.2) | <0.0001 | |
| Mean (95% CI) | ||||
| Losers >15 letters, % | 15.70% | 22.22% | 0.12 | |
| Winners >15 letters, %. | 10.30% | 5.55% | 0.12 | |
| Active visits, % Active visits, % Active visits, % Active visits, % Active visits, % Active visits, % Active visits, % | 58.20% | 33.58% | <0.0001 | |
| Median number of injections (Q1, Q3) | 11 (9.14) | 8 (2.13) | ||
| Median number of visits (Q1, Q3) | 14 (12.18) | 9 (7.11) |
VA: visual acuity; SD: standard deviation.
As in previous studies,10,14,21,25 we did not observe recovery of VA loss, despite the increase in the number of AAG injections observed after lockdown, which in some studies even exceeds the figures reported before lockdown. As in the study by Rego-Lorca et al. in which they report that, during the year prior to lockdown, the mean number of AAG injections was 5.4 ± 1.8 and during the first post-pandemic year, it increased to 6 ± 2.7.21 In our work, the mean number of injections is 4.62 ± 2.70 the first year, lower than that reported by them since we included the months of lockdown, however, they exceed the mean of Rego-Lorca et al.21 (6.11 ± 5.10) at 24 months. The median number of consultations in our series did not increase to the same extent as injections because the number of consultations with simultaneous administration of AAG increased as a measure to improve adherence to treatment and facilitate care.
A study with a short follow-up period described a 3.1% increase in active NVM on OCT images six months after the start of lockdown.22 While Yeter et al.11 and Rego-Lorca et al.21 identified anatomical improvement, without associated functional improvement, at 3.5 and 12 months after lockdown, in agreement with other studies with similar findings.10,14,21,25,27 We found a decrease in activity in all the periods studied, with respect to pre-pandemic activity. We agree that the decrease in the percentage of activity is not related to improvement in VA. Thus, we observed a higher percentage of inactive NVM in the group that suspended follow-up during lockdown, probably associated with a lower need for injections prior to the pandemic, which may have been the reason for absenteeism from consultations during the pandemic.
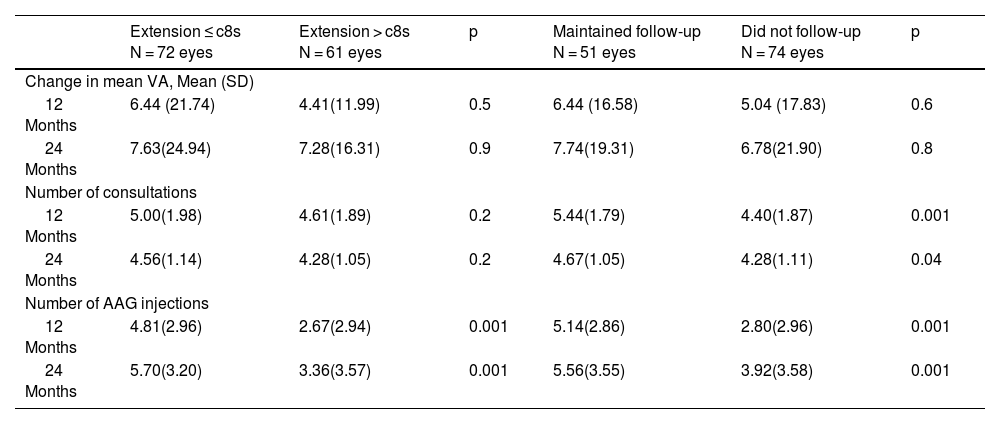
We did not observe significant differences in VA at 24 months of follow-up between patients with intervals between injections equal to or less than eight weeks, with respect to those with longer intervals (Table 4).
Changes in VA, number of consultations and IVT injections among patients with AAG IVT treatment extension periods equal to, less than or greater than 8 weeks and among patients who maintained follow-up during lockdown compared to those who did not.
| Extension ≤ c8s N = 72 eyes | Extension > c8s N = 61 eyes | p | Maintained follow-up N = 51 eyes | Did not follow-up N = 74 eyes | p | |
|---|---|---|---|---|---|---|
| Change in mean VA, Mean (SD) | ||||||
| 12 Months | 6.44 (21.74) | 4.41(11.99) | 0.5 | 6.44 (16.58) | 5.04 (17.83) | 0.6 |
| 24 Months | 7.63(24.94) | 7.28(16.31) | 0.9 | 7.74(19.31) | 6.78(21.90) | 0.8 |
| Number of consultations | ||||||
| 12 Months | 5.00(1.98) | 4.61(1.89) | 0.2 | 5.44(1.79) | 4.40(1.87) | 0.001 |
| 24 Months | 4.56(1.14) | 4.28(1.05) | 0.2 | 4.67(1.05) | 4.28(1.11) | 0.04 |
| Number of AAG injections | ||||||
| 12 Months | 4.81(2.96) | 2.67(2.94) | 0.001 | 5.14(2.86) | 2.80(2.96) | 0.001 |
| 24 Months | 5.70(3.20) | 3.36(3.57) | 0.001 | 5.56(3.55) | 3.92(3.58) | 0.001 |
VA: visual acuity; c8s: every eight weeks.
The present study provides estimates of the discontinuation of IVT therapy and the effect on visual outcomes caused by the COVID-19 pandemic over a 24-month period following lockdown and compares it to a national study of the same duration conducted before the pandemic. Other studies with shorter time periods of post-pandemic follow-up hypothesized that, with longer follow-up and similar visit and injection intervals as pre-pandemic, VA would return to earlier values.18,19 We found that eyes with nAMD lost VA in relation to the lower number of injections and visits during lockdown, and that this loss is maintained over time, despite the recovery of the number of visits and injections in the months following lockdown. Considering these results, it seems appropriate to prioritize IVT AAG therapy in patients with nAMD in similar settings.17,18,22
Ethical considerationsAll patients signed an informed consent form to participate in the study, which followed the norms of the Declaration of Helsinki. The protocol was approved by the Medical Research Ethics Committee of the Príncipe de Asturias University Hospital with number OE 01/2021.
FundingThis work has not received private or public funding for its conception, execution and development.
Conflict of interestThe authors declare that they have no conflicts of interest related to this work.
