


Osteosarcoma is one of the most common types of cancer in school age and adolescence being the most common malignant bone tumor in this age group. Osteosarcoma is frequently found in long bones of the extremities. There are very few cases described in children under five years of age. Moreover, according to our revision none in infants. The telangiectatic variant is uncommon, and there are no reports before preschool age.
Case reportA 10-month-old female infant that presented a lithic tumor of the ninth right rib, which was classified after resection as a telangiectatic osteosarcoma, is presented.
ConclusionsTelangiectatic osteosarcoma in the pediatric age is very uncommon. To date, the patient presented a good response to treatment, although the prognosis and survival of this condition are unknown.
El osteosarcoma es uno de los tipos de cáncer más común en la etapa escolar y en la adolescencia, y es el más común de los tumores óseos malignos en este grupo de edad. Frecuentemente, el osteosarcoma es hallado en los huesos largos de las extremidades. Existen muy pocos casos descritos en menores de 5 años. Hasta donde se sabe, no hay ningún caso reportado en lactantes. La variedad telangiectásica es poco común y no existen casos reportados antes de la edad pre-escolar.
Caso clínicoSe presenta el caso clínico de una paciente lactante de 10 meses de edad que presentó un tumor lítico en la novena costilla derecha, que posterior a la resección fue clasificado como osteosarcoma telangiectásico.
ConclusionesEl osteosarcoma telangiectásico en la edad pediátrica es poco común. A la fecha, la paciente ha presentado buena respuesta al tratamiento, aunque se desconoce el pronóstico y la supervivencia de este padecimiento.
Although its incidence varies with age, osteosarcoma is one of the most common types of cancer in school age and adolescence being the most common malignant bone tumor in this age group.1 The Surveillance, Epidemiology, and End Results Program (SEER) from de National Cancer Institute (NCI) in the United States reports 2.4 cases per million population per year between 5- and 9-year-old children, 7.6 cases per million population per year between 10- and 14-year-old children and 8.2 cases per million population per year between 15-and 19-year-old adolescents.
Osteosarcoma is very rare in children under five years of age, with an incidence of 0.4 cases per million population per year. Worch et al. reported 1786 patients under 20 years of age between 1973 and 2003. They only found one patient under one year of age.2 Four osteosarcoma cases in children under 18 months of age have been reported; two girls, 13- and 14-month-old, who had a femoral osteoblastic tumor, a 14-month-old boy with a tumor equal in localization and histology, and a 16-month-old boy with an osteoblastic humeral tumor.
Rivera-Luna et al. reported the case of a 3-year-old girl with a femoral telangiectatic tumor.3
Information about osteosarcoma in very young patients is scarse.1,4 The telangiectatic variety, especially in the rib cage, is less common.5–7
In this report, the case of a 10-month-old infant with osteosarcoma is described.
2Clinical caseA 10-month-old infant with anemia under treatment with oral iron supplementation arrived at the emergency service with a history of 17 days of subjective fever and hematochezia. She received ambulatory treatment with antibiotics and probiotics, and after a mild initial improvement, she developed 39°C fever, vomit, and hyporexia.
At physical examination, she was conscious and irritable with 98% capillary oximetry, heart rate of 136 beats per minute, a respiratory frequency of 32 per minute and blood pressure of 117/81mmHg (mildly above her height/age percentile average). Her weight was 7.4kg (Z-score: -1.3) and her height, 60cm (Z-score: -5).
She looked pale, with dry mucous membranes and a capillary refill of 3 s. At chest inspection, costal retractions were noticed, and at chest auscultation, hypoventilation at the right lung base and rhythmic heart sounds.
Blood analysis documented hemoglobin 7.9g/l, C-reactive protein 37mg/dl, procalcitonin 1.2 nmol/l. Liver enzymes, renal function, and serum electrolytes were within normal limits.
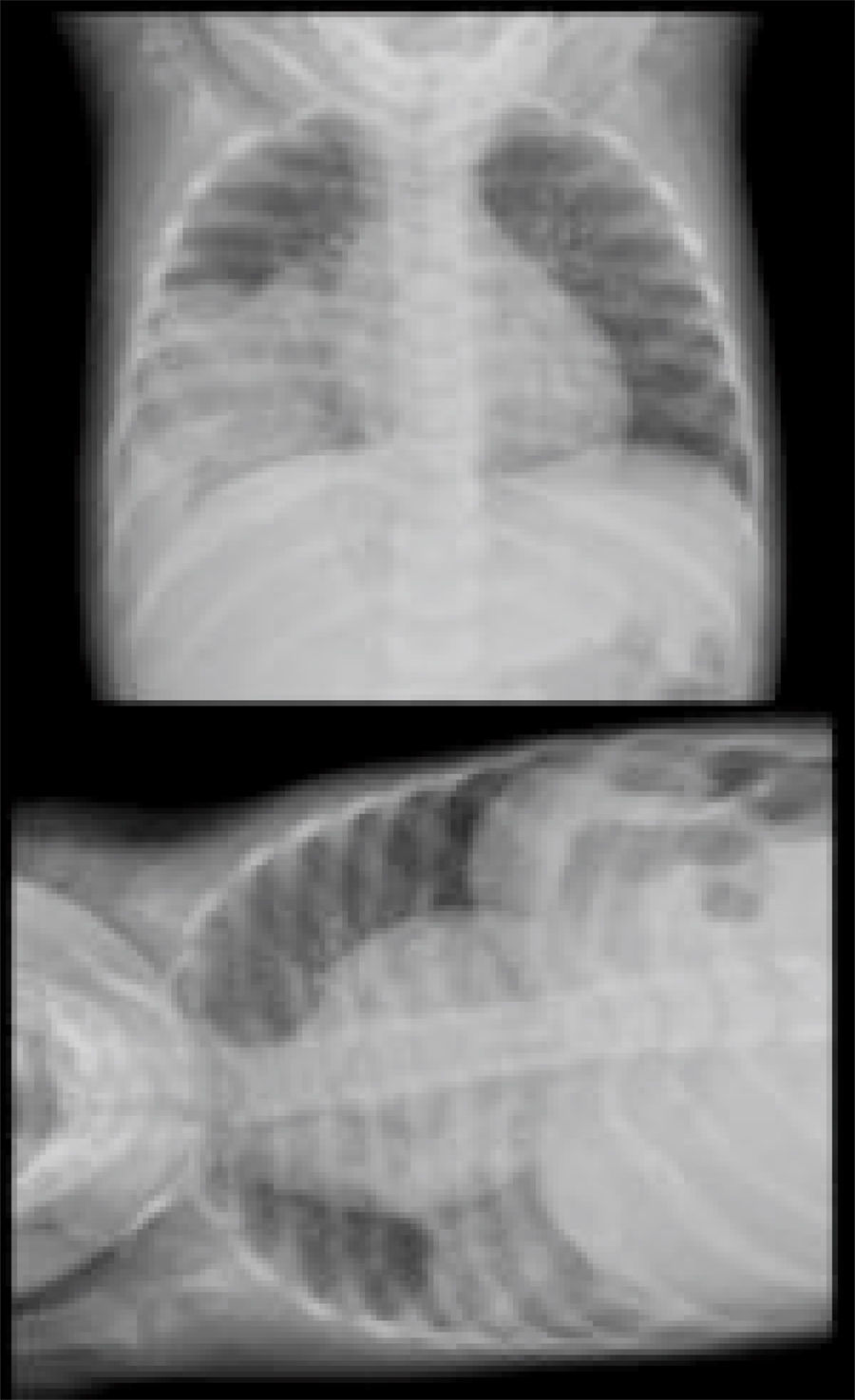
Due to dehydration signs, 0.9% of saline was administered at a 10ml/kg rate. A regular chest X-ray showed at the right lung base a radio-opaque image and loss of the right rib-diaphragm angle without changes in its horizontal projection (Figure 1). Echography analysis showed a solid image, heterogeneous in its composition, with undefined borders and a hyperechogenic and anechoic 7cm center discretely vascularized.

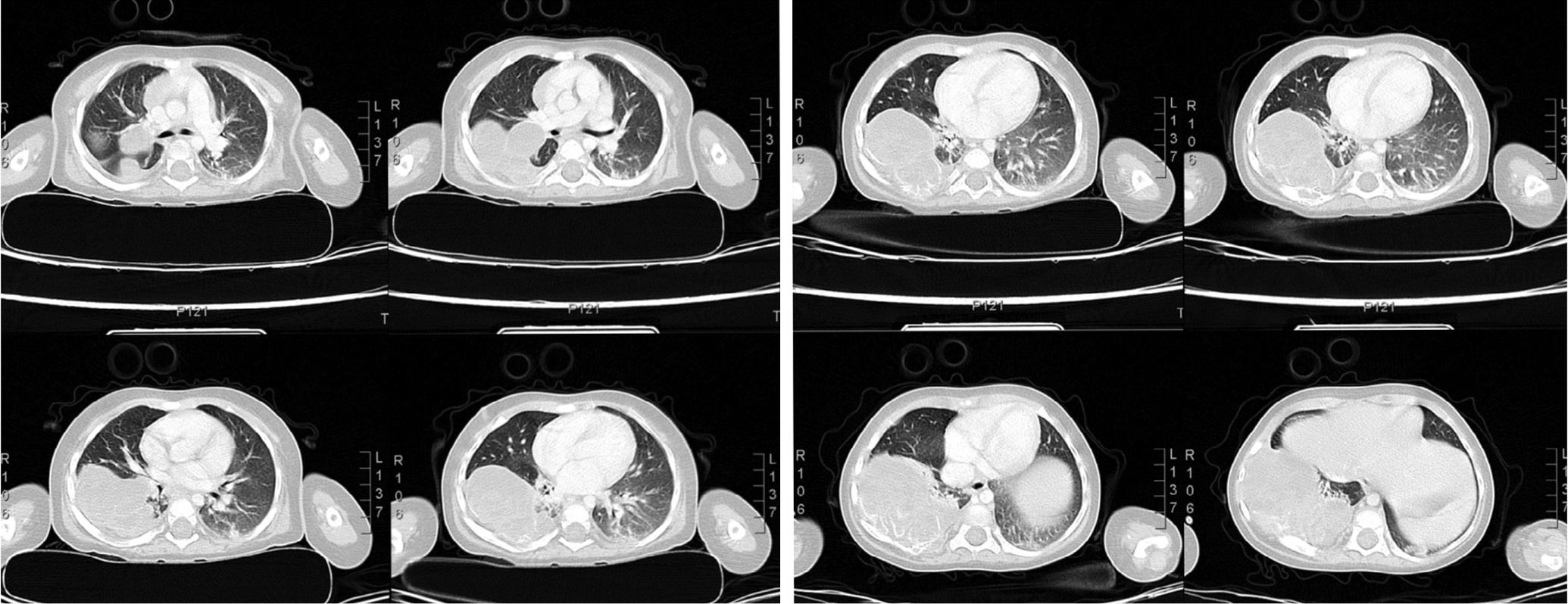
The patient presented tachypnea and oxygen was administered with a low flux device. Antibiotic treatment was started with third generation cephalosporins. A regular chest CT scan showed a hypodense mass located in the inferior right lobe, which produced diaphragm depression and protruded to the posterior abdominal cavity with septums, some of which were calcified in its superior and posterior portions.
The mass dimensions were 85 x 53.5mm with densities between 5 and 35 HU, emerging from the ninth rib in its posterior arch. In the posterior segments of the left inferior thorax, confluent infiltrative lesions, which formed a small area of pulmonary consolidation, were observed.
After the administration of intravenous contrast, no significant changes in the attenuation of the tumor or mediastinal and perihilar adenopathies were observed (Figure 2).

Given these results, we asked for the involvement of the hemato-oncology and surgery services and complementary tests to rule-out tumor lysis. Elevated values of ferritin of 549 ng/ml were found (normal reference values for 7 to 12 months of age are 36-100 ng/ml) and carcinoembryonic antigen of 5.19 ng/ml (normal reference value < 3 ng/ml).
Based on the oxygen requirements and an increase in ventilator distress, a red blood cell transfusion was ordered at a 15ml/kg rate.
Due to previous findings, tumor markers were measured with these results: neuronal specific enolase, 47.47μg/l (normal reference value of 0-16) and beta-2 microglobulin, 1mg/l (normal reference value 0.8-3.0mg/l).
The surgery service evaluated the patient and decided to perform a biopsy with the pre-surgical diagnosis of osteosarcoma. The patient underwent a thoracotomy in which the ninth and tenth right ribs were extracted as well as a lobed tumor from the ninth rib with free clots in the cavity.
An atelectasis was observed due to compression of the middle and inferior right pulmonary lobes, and a chest tube connected to a water seal was placed, and the surgical wound was repaired in anatomical planes.
The patient was transferred to the intensive pediatric care unit for post-surgical management, and the tumor was taken to the Pathology Department for its analysis.
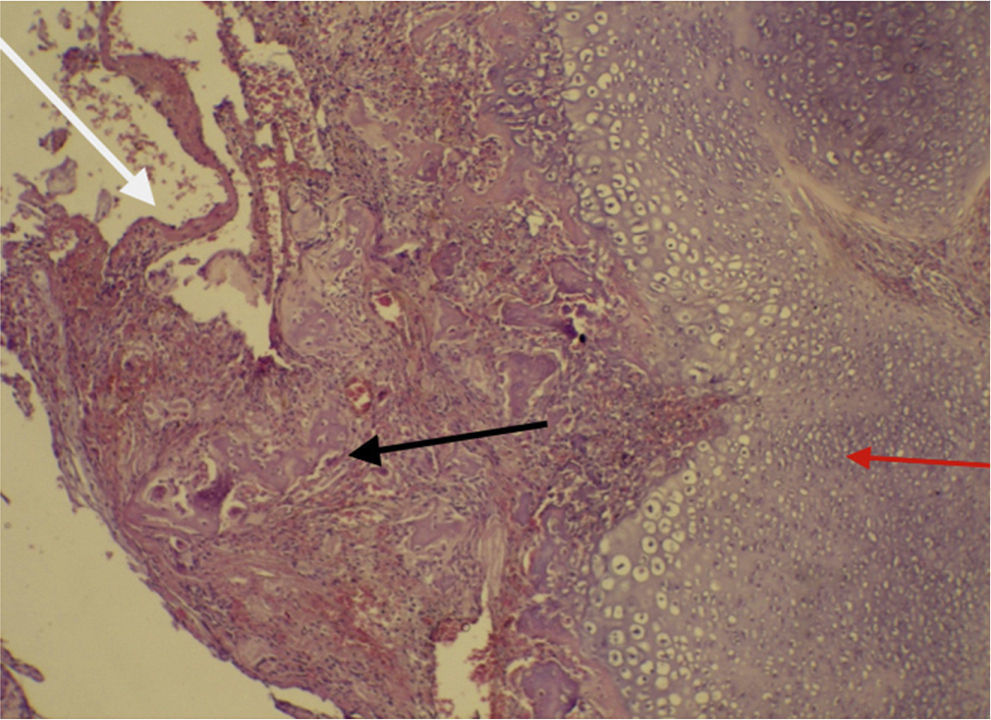
The histopathological and immunohistochemistry report identified the tumor as a costal telangiectatic osteosarcoma with pleural involvement (Figure 3). Bone gammagraphy analysis ruled out metastasis.
.")
The patient was transferred to a local oncologic hospital to receive treatment. Two cycles of chemotherapy with vincristine, cyclophosphamide, doxorubicin, dexrazoxane and mesna were planned. Seven days after the first cycle, the patient presented febrile neutropenia, filgrastim, antibiotic treatment with antimycotic, aminoglycosides and a fourth generation cephalosporin were started. She also presented anemia, for which a red blood cell transfusion was administered. The patient also had mucositis, which was treated with opioids.
One month later, the patient received the second chemotherapy cycle without eventualities. After the second chemotherapy cycle, an echocardiogram was performed, which showed normal structure and function. To the date of this publication, the patient is stable and has shown a good response to treatment.
3DiscussionOsteosarcomas are tumors that can appear in any bone structure. They are the third most frequent cancer in school age and adolescence after lymphomas and cerebral tumors.8 The most common sites for these tumors are the femur (42%), from which 75% locate in the distal portions; the tibia (19%), from which 80% locate in the proximal portions, and the humerus (10%), with 90% of the tumors located near its proximal end. They can also be found in the skull o the jaw (8%) and pelvis (8%).9
According to the Cooperative Osteosarcoma Study Group (COOS) of the United States, which gathered patients during 28 years (2076 patients with high-grade osteosarcoma), only 28 patients under 5 years of age were identified with this diagnosis, which represents only 1% of all osteosarcoma patients (1 case per 100 000 population per year). None of the 28 patients presented the tumor in the ribs; on the contrary, the presentation was in the femur, tibia or humerus in all cases. There were three cases of lung metastasis4 in the telangiectatic group; in the group of patients under five years of age, no case had a tumor located in the ribs.2,5
Osteosarcomas in the ribs are a rare even in adulthood; they have a bad prognosis and a 5-year survival rate of 11.7%.10 From all pediatric malignant tumors in the rib cage, Ewing's sarcoma was reported in 193 patients from 1973 to 2011 according to data from the SEER, from which only 17 cases were patients under five years of age. The survival rate at five years in this group was 60%.11
Since 2014, from eight patients in whom a malignant bone tumor was suspected, only a 5 years 9-month-old male was diagnosed with a femoral undifferentiated osteosarcoma at Hospital Roberto Gilbert (HRG). To this date, there has not been another diagnosis of telangiectatic osteosarcoma at HRG.
The most common symptom of osteosarcoma is joint pain (growth pains), mainly during activity. In the telangiectatic type as in this case, pathologic fractures are common. Fever is a rare symptom in these patients. Lung metastasis rarely give any respiratory symptoms.2,4,5
In this patient, respiratory symptoms were very noticeable during physical examination because the tumor had extended from the rib to the right lung. Due to the histologic type of the osteosarcoma and its location, there were no pathologic fractures, which were indeed observed in four of six patients with telangiectatic osteosarcoma reported by the COOS.4 In the literature, another case of telangiectatic osteosarcoma located in the rib cage in the age group of this patient has not been found.
Five-year-survival in the COOS cohort study was 51%. Tumor resection with broad margins and a good chemotherapy response in the primary tumor were factors that improved survival.4,8 In the present case, tumor resection was accomplished, and affected ribs were removed.
The patient has had a good response to chemotherapy to this date. Survival rates or prognostic factors for telangiectatic rib osteosarcoma in this age group have not been found. It should be considered that in the SEER's data analysis, it was mentioned that in patients under five years of age, prognosis and survival are unknown. Since it is a rare age of presentation, there are only institutional reports, where the bad prognosis has been reported in patients under five years of age with telangiectatic osteosarcoma.2
A good prognostic factor that has been documented in limb osteosarcoma studies is the presence of normal or slightly elevated lactate dehydrogenase levels12 and alkaline phosphatase.13 The patient, in this case, presented normal serum values in both tests.
As a conclusion, it is restated that telangiectatic osteosarcoma in pediatric age is uncommon. There are only a few cases reported in patients under five years of age. To the extent of our knowledge, not a single case in infants has been reported. This disease has been linked with inheritance.2 However, any relevant familial history was not found.
The intention of this work is to add to the literature and medical statistics one more case of telangiectatic osteosarcoma in a female infant patient.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestThe authors declare no conflict of interest of any nature.
Please cite this article as: Cepeda MdlÁ, Sosa AJ, Mora G. Osteosarcoma telangiectásico en un lactante. Bol Med Hosp Infant Mex. 2017;74:60–64.