


The incidence of deaths and injuries associated with gunshot wounds deserves special attention, mainly because of its repercussions on hospital resources and the diagnosis and treatment protocols.
ObjectiveTo perform an analysis on the epidemiological factors associated with gunshot wounds.
Material and methodsAn analysis was made of multiple variables of all patients diagnosed with gunshot wounds during the period between 2005 and 2015.
ResultsA total of 605 cases were found, and an additional sub-group of 314 cases was obtained for a deeper analysis. The overall mortality rate was 7.9%. The main anatomical region was the abdomen, with 44%. A total of 324 laparotomies were performed, 124 incisions of the thoracic wall, and 72 vascular examinations. In the sub-group of 314 cases, a 16.9% and 42% of laparotomies and vascular examinations, respectably, were reported without evidence of injury to internal organs.
DiscussionMorbidity and mortality increases when 2 or more wounds are present with multiple organ injuries, in patients with multiple transfusions, or in those transferred to the intensive care unit.
ConclusionsThe incorporation of a physical evaluation format by all the departments involved is suggested for patients that are attended with gunshot wounds, in order to obtain more epidemiological information of these injuries for further studies.
La incidencia de heridas y muertes por herida por proyectil de arma de fuego merece una atención especial en su epidemiología, protocolos de manejo y tratamiento.
ObjetivosDeterminar las características epidemiológicas de las heridas por proyectil de arma de fuego.
Material y métodosEntre 2005 y 2015 se analizaron todos los pacientes con diagnóstico de heridas por proyectil de arma de fuego. Se estudiaron múltiples variables de su atención hospitalaria.
ResultadosSe obtuvo un total de 605 casos, los cuales se analizaron como universo total de pacientes y, además, se tomó una muestra de 314 casos, para un análisis más detallado. Se obtuvo una mortalidad total de 7.9%. Se realizaron 324 laparotomías, 124 incisiones de la pared torácica, y 72 exploraciones vasculares. Dentro del grupo de resultados específicos se obtuvo un 16.9% y 42% de laparotomías y exploraciones vasculares, respectivamente, sin evidencia de lesión.
DiscusiónLa morbimortalidad aumenta significativamente en pacientes con 2 o más heridas, múltiples transfusiones y con requerimiento de estancia en la unidad de cuidados intensivos.
ConclusionesSe propone la incorporación de un formato de evaluación física de los pacientes con heridas por proyectil de arma de fuego, por parte de los servicios involucrados en su atención, que promueva la generación de trabajos de investigación más detallados.
Gunshot wounds vary in many ways regarding their mechanism of production or ballistic properties, the site of the wounds, the anatomical regions which are affected, the severity of the wound and the possible evolution of the affected organs.
Regardless of how slight a wound appears to be, patient evaluation must be exhaustive and must always take into account the possibility that vital structures have been affected. It is therefore fundamental to detect wounds that may be catastrophic if they are detected at a late stage, given that some wounds take some time before causing clinical symptoms. These include intestinal perforations, certain wounds to blood vessels, lead poisoning and tissue necrosis caused in the periphery of the projectile path cavity.1
Gunshot wounds are now a worldwide public health problem. In the past 15 years wounds caused by weapons of this type have undergone a major increase.2 Many factors have influenced this growth, including family disintegration, unemployment, joining criminal groups when young, experiences with drugs and the uncontrolled diffusion of violent acts in the mass media, as well as the fact that weapons are easier to acquire.3
Every year in the United States 30,000–50,000 people die due to gunshot wounds, and they are the first cause of death in the first 2 decades of life; moreover, it is estimated that for each death there are at least 3 incapacitating wounds. This means there are approximately 150,000 gunshot wounds per year.4 Violence using firearms has a major economic impact, as it is the third most expensive lesion and the fourth cause of hospitalisation.5
In the period from 2000 to 2007 400,000 deaths occurred due to external causes.6 Of these, 79,784 were homicides, amounting to 19% of the total. When the external causes of mortality in the general population are analysed individually, homicides are the second cause of death after traffic accidents, while in some age groups such as the one from 25 to 44 years old they are the first cause.7
In the year 2000 Mexico had a higher than 2 digit rate of homicides per 100,000 inhabitants (10.15). This figure has gradually gone down to a rate of 8.38 in 2007, one of the lowest rates in decades.8
Violence is now seen to be a public health problem and a serious social epidemic. It is expressed not only in the number of deaths or mortality rates, but also in the amount, intensity and variety of ways in which it occurs. It also causes deterioration in quality of health and the health conditions of the population.9
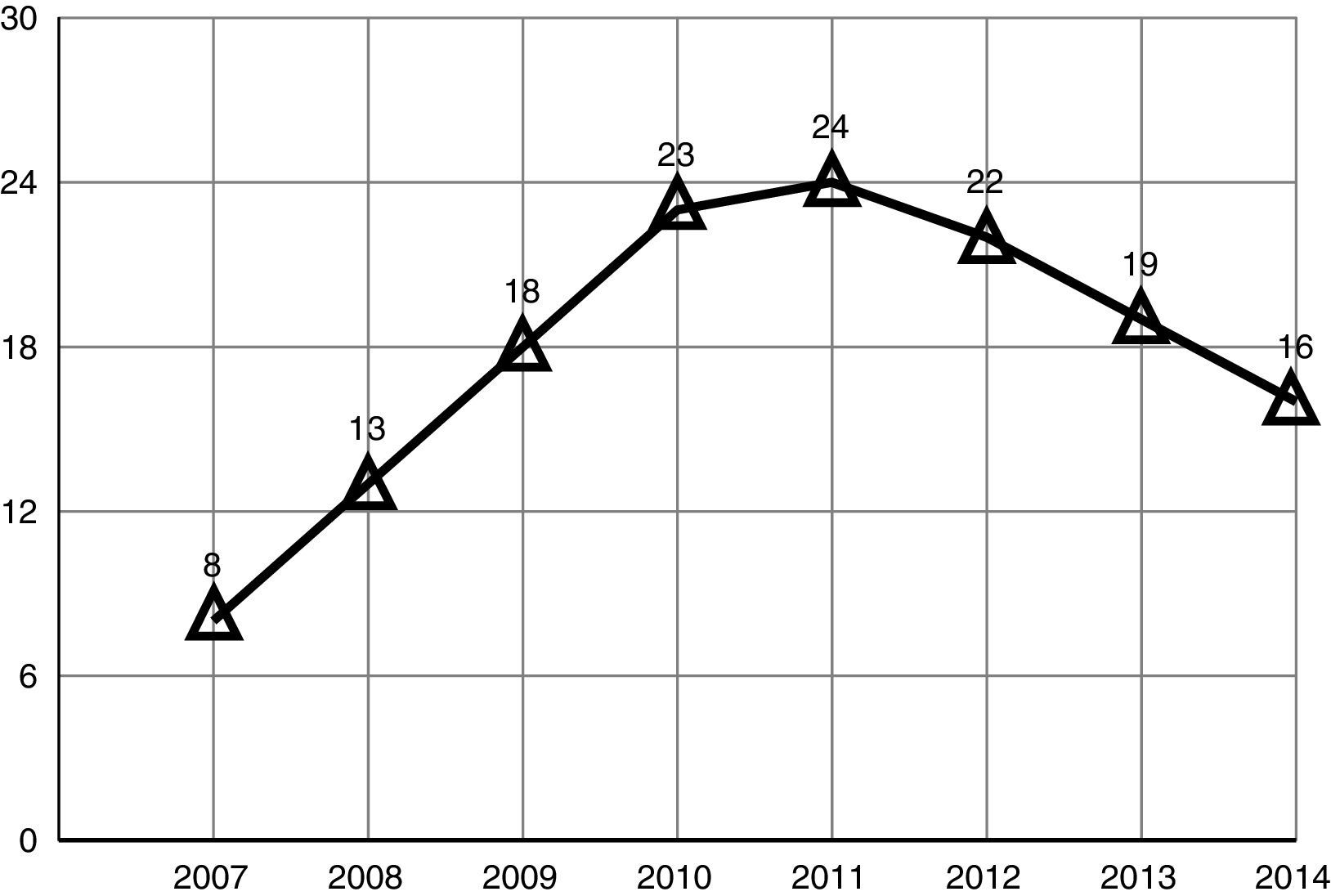
Statistics show that in 2014 20,010 homicides were recorded in Mexico (11,514 of which were caused by firearm projectiles), i.e., a proportion of 16 per 100,000 inhabitants at national level.10
Homicides cause about 1.5% of total deaths in our country. According to the vital statistics of the National Statistical and Geographical Institute (INEG), there were no major variations in the number of homicides recorded from 2000 to 2007. However, in 2008 a significant increase was recorded, with 14,006 homicides (13 per 100,000 inhabitants). This tendency carried on increasing and reached its highest peak in 2011, with 27,213 homicides (24 per 100,000 inhabitants). Subsequently there was a slight reduction down to the figure of 20,010 homicides recorded in 2014 (16 per 100,000 inhabitants), which represents a fall of 27% in comparison with 201211 (Fig. 1).
.")
It is clear that differences exist between different Federal districts in our country, and that these should be considered. According to INEG data, among the areas with the highest levels of homicides particularly outstanding cases include Chihuahua (76 per 100,000 inhabitants), Baja California (33 per 100,000 inhabitants) and Sinaloa (30 per 100,000 inhabitants). All of these underwent a sudden increase during 2008, mainly located in the municipalities of Ciudad Juárez (108 per 100,000 inhabitants), Tijuana (47 per 100,000 inhabitants) and Culiacán (42 per 100,000 inhabitants), respectively.12
The state of Nuevo León has remained among the first 12 regions over the years. According to the latest INEG data, in 2014 the areas with the highest homicide levels were Guerrero (48 per 100,000 inhabitants), Chihuahua (46 per 100,000 inhabitants), Sinaloa (38 per 100,000 inhabitants), Tamaulipas (25 per 100,000 inhabitants) and Sonora (23 per 100,000 inhabitants).13
Homicide mainly affects men. Murders of men account for from 87% to 90% of all homicides, and of these, the age group that is affected the most is that from 15 to 34 years old.14,15
The increase in violence in our country is associated to a certain degree with the increase in unemployment rates, with levels of poverty and with the fall in per capita GDP.16 Additionally, we should not ignore the increasing number of firearms possessed by the Mexican population, the majority of which are brought into the country illegally over the border with the United States. It has even been said that about 80% of the weapons confiscated by the Mexican authorities from 2006 to 2010 had been illegally brought into the country from the United States.17
The percentage of homicides caused by gunshot has increased notably over recent years, so that now almost 2 of every 3 homicides in the country are committed using firearms. This illustrates not only the levels of violence which exist, but also the availability in the market and accessibility of weapons of this type, which are obviously more lethal.18
It is vitally important that doctors and health institutions are expert in external, internal and terminal ballistics associated with clinical symptoms. This knowledge offers us important data which allows us to understand the different types of wounds presented by a patient with gunshot injuries. The magnitude of the wounds caused by a firearm depends on the energy transmitted by the projectile to the target, and this depends not only on velocity but also on the calibre or diameter of the projectile, its shape, stability in flight and its weight.
Firearm projectiles cause damage by tissue disruption, leading to haemorrhages and infections. The amount of kinetic energy transferred from a projectile to the surrounding tissues, internal organs and structures which are damaged directly, as well as the final location of the projectile, all determine the severity of gunshot wounds.
ObjectivesOverall objectiveTo describe the epidemiology of gunshot wounds in “Dr. José Eleuterio González” University Hospital, of Nuevo León Universidad Autónoma, so that it can be properly analysed, as well as to gain greater knowledge of the socioeconomic variables involved in their management and treatment.
Secondary objectivesTo generate statistical information that will be useful for other disciplines connected with public health and security, to attain greater comprehension of this complex social problem. To generate information that is reliable and objective, so that the most affected anatomical sites can be identified together with the type of wound and surgical treatment applied. This will make it possible to develop training courses for interns that centre on the most frequent types of wounds in our area.
Material and methodsRetrospective, observational, descriptive and transversal analysis was undertaken for the design of this study. A population of patients admitted to the General Surgery Department of “Dr. José Eleuterio González” University Hospital of Nuevo León Universidad Autónoma, during a period from January 2005 to December 2015 and diagnosed as having suffered gunshot wound.
Description of study designThe study was carried out with the authorisation of the Hospital Research Committee. The variables to be analysed were taken from a database supplied by the Archive and Statistical Department of the said hospital. After this the files from the period from January 2011 to December 2015 were reviewed, as no clinical files were available from previous years due to the clearance policy. The information was collected in a database for subsequent statistical analysis.
Variables analysedYear, month, sex, age, marital status, occupation, Mexican state, municipality and suburb of residence, days of hospitalisation, duration of stay in the Intensive Care Unit, anatomical site of wound, number of wounds, type of wound, surgical approach and treatment, blood transfusions and patient follow-up and mortality.
Inclusion criteriaPatients admitted to and treated by the General Surgery Department of “Dr. José Eleuterio González” University Hospital of Nuevo León Universidad Autónoma, and diagnosed as having suffered gunshot wound during a period from January 2005 to December 2015.
Exclusion criteriaPatients with incomplete data.
As this is a retrospective study neither the approval nor the informed consent of patients were obtained. Statistical data are used without including any personal data of the subjects.
Evaluation methodsData were analysed using the Numbers® v3.6.1 (Apple Inc.) computer programme. Statistical analysis was performed using the IBM SPSS Statistics v20.0 programme (SPSS, Inc., Armonk, NY, U.S.A.), of a descriptive type according to conventional methods, and the results are expressed as tables and figures, enabling conclusions to be drawn.
ResultsA total of 1423 cases of patients admitted to “Dr. José Eleuterio González” University Hospital with a diagnosis of gunshot wound from January 2005 to December 2015 were reviewed. Of these 605 were admitted and treated by the General Surgery Department, and these were considered to be the total universe of patients (n=605). The majority of the other patients were treated by the Traumatology or Neurosurgery Departments, and they were excluded from the study.
The decision was taken to divide the results into 2 groups, general and specific. The group of general results included all of the cases (n=605) with data obtained from the database supplied by the Hospital Archive and Statistics Department. It was no possible to revise the clinical files of cases from January 2005 to December 2010 due to the clearance policy, according to which only the last 5 year history of each patient is kept on file. This group included the variables of year, month, sex, age, marital status, occupation, state of the Mexican republic, municipality and suburb of residence, days of hospitalisation, duration of stay the Intensive Care Unit, anatomical location of the wound, surgical approach and mortality.
The group of specific results only included the sample of cases from January 2011 to December 2015 (n=359) and, of these, only those for which it was possible to revise their clinical file (n=314), so that more detailed information was obtained about each case. This group also included the variables of number of wounds, number of lesions, type of lesion, surgical treatment applied, blood transfusions, number of days in the Intensive Care Unit and patient follow-up.
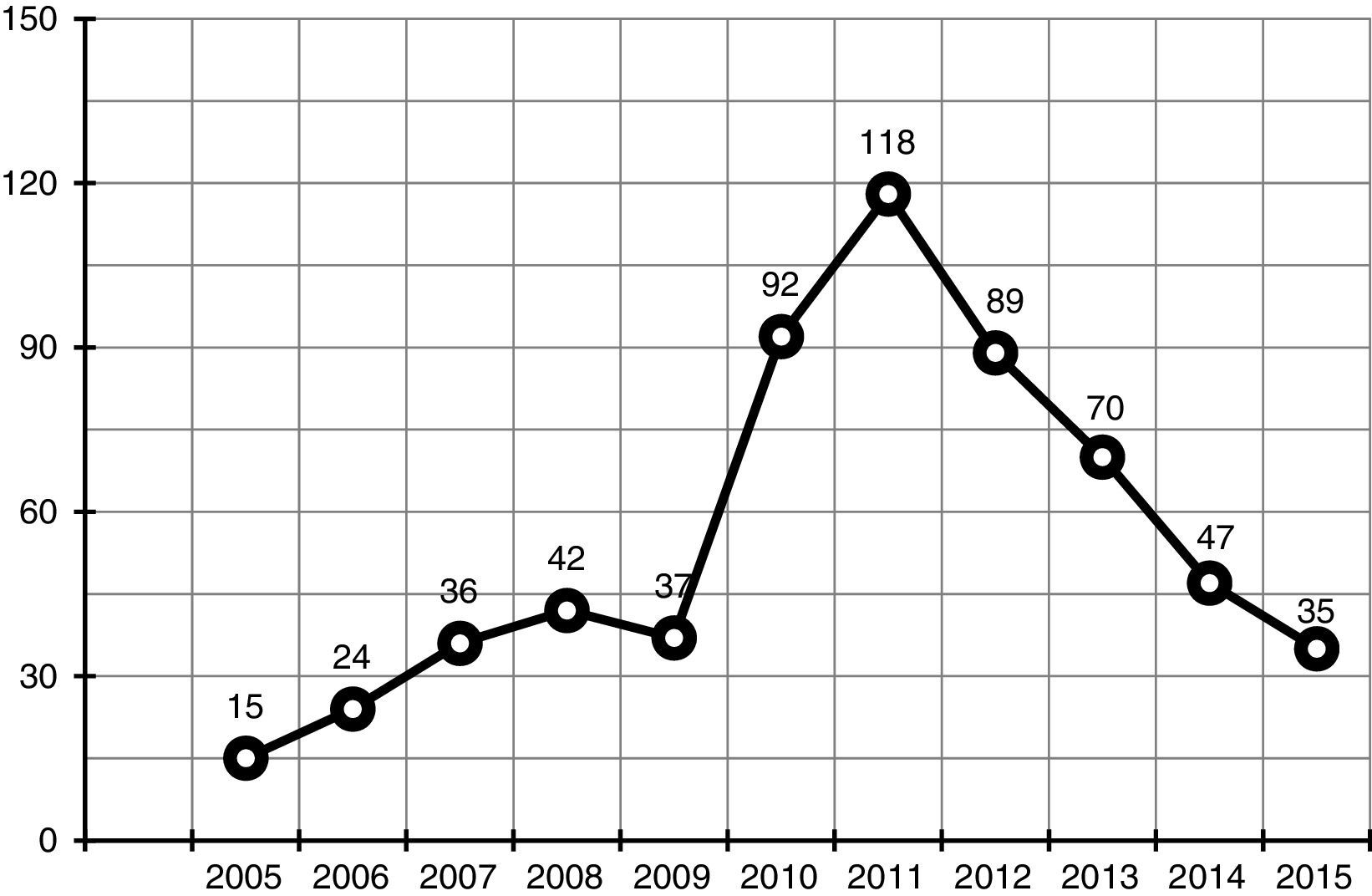
Group I. General resultsA total of 605 cases were reviewed, of which the year with the most cases was 2011 with 118 (19.5%) of reported cases, followed by 2010 and 2012 with 92 (15.2%) and 89 (14.7%) cases, respectively (Fig. 2). The distribution according to year showed a notable increase in 2010, 2011 and 2012 which together accounted for 49.4% of cases, with 299 patients. Regarding the months when cases occurred, the highest number of cases were in June, with 72 (11.8%) cases, followed by February with 62 (10.2%).

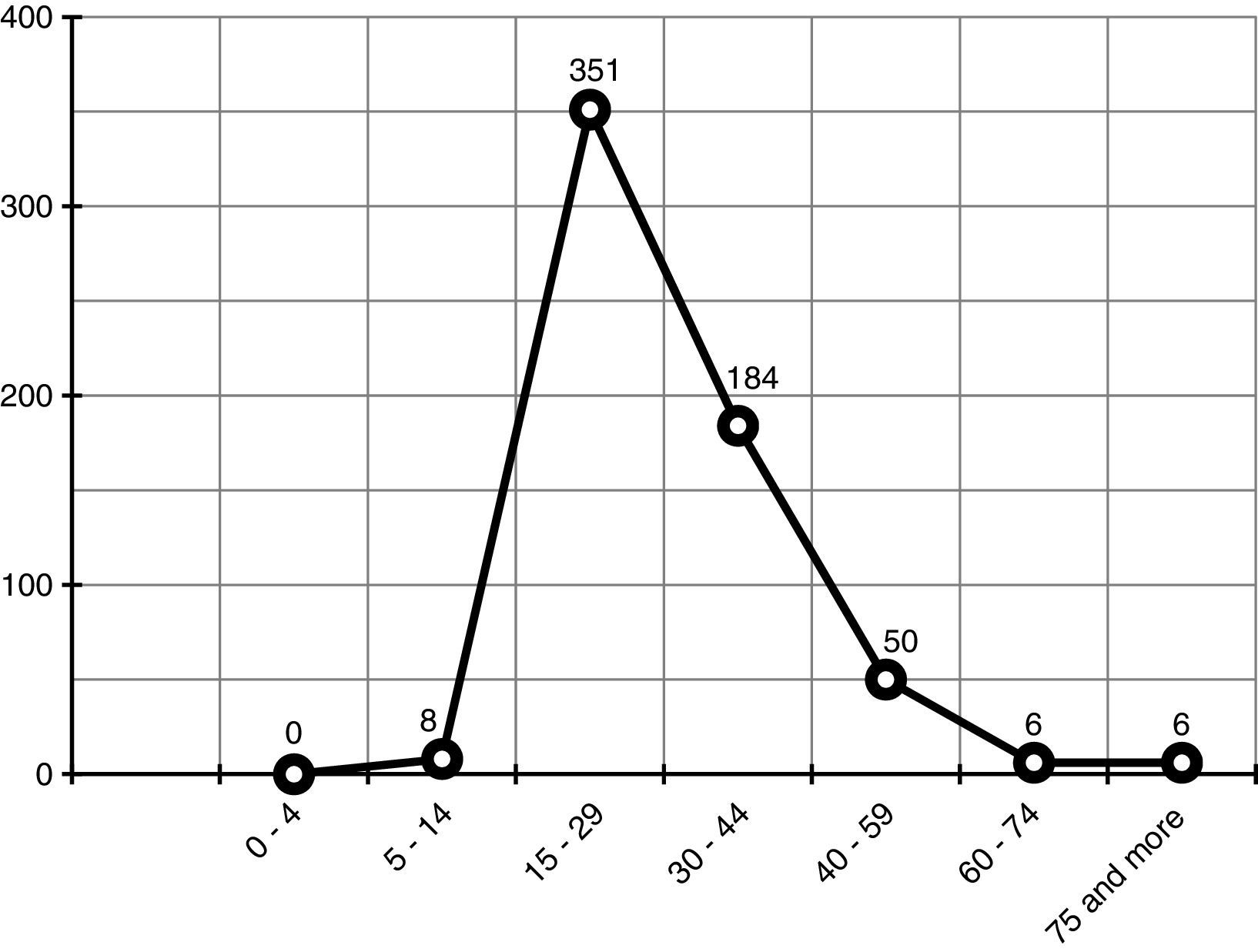
Demographic variables were analysed with the following results: men predominated, with 554 (91.6%) cases; the average age was 29.4 years old, with a SD of 11.8. This corresponds to 58% of the cases, which are distributed in the age group from 15 to 29 years old (Fig. 3). In terms of marital status, a total of 298 (49.2%) patients were single, 161 (26.6%) were married and 98 (16.2%) were living with their partner.

Regarding occupation, the groups with the largest numbers of cases were builders/workers, with 110 (18.2%), employees with 95 (15.7%) and unemployed with 74 (12.2%) patients.
All of the patients were from the state of Nuevo León, within which the municipalities with the highest rates of incidence were Monterrey (309 cases, 51%), a percentage that could be expected given the location of the hospital, followed by the municipalities of Guadalupe (58, 9.6%), Apodaca (49, 8.1%), San Nicolás (32, 5.3%), Escobedo (28, 4.6%), Santa Catarina (26, 4.3%) and Juárez (19, 3.1%).
A total mortality of 7.9% was reported; the median number of days of hospital was 7, with an interquartile range of 7–13. Additionally, 84 (13.9%) of the cases required a period of time in the Intensive Care Unit.
The anatomical locations which were involved the most often were the abdomen, with a total of 266 (44%) cases, followed by the thorax with 118 (19.5%) cases. It has to be born in mind that this study only took into account patients admitted to the General Surgery Department, so that anatomical locations such as the limbs, which are normally some of the locations most commonly affected,1,2 are hardly reported in this study.
597 surgical procedures were performed, with 324 (54.4%) laparotomies, 124 (20.8%) incisions in the thoracic wall and pleural wall, and 72 (12%) vascular explorations, among others.
Group II. Specific resultsThis group includes the sample of cases in which it was possible to review their clinical file (n=314), adding the following variables: number of wounds, number of lesions, type of lesion, surgical treatment, blood transfusions, days in the Intensive Care Unit and patient follow-up.
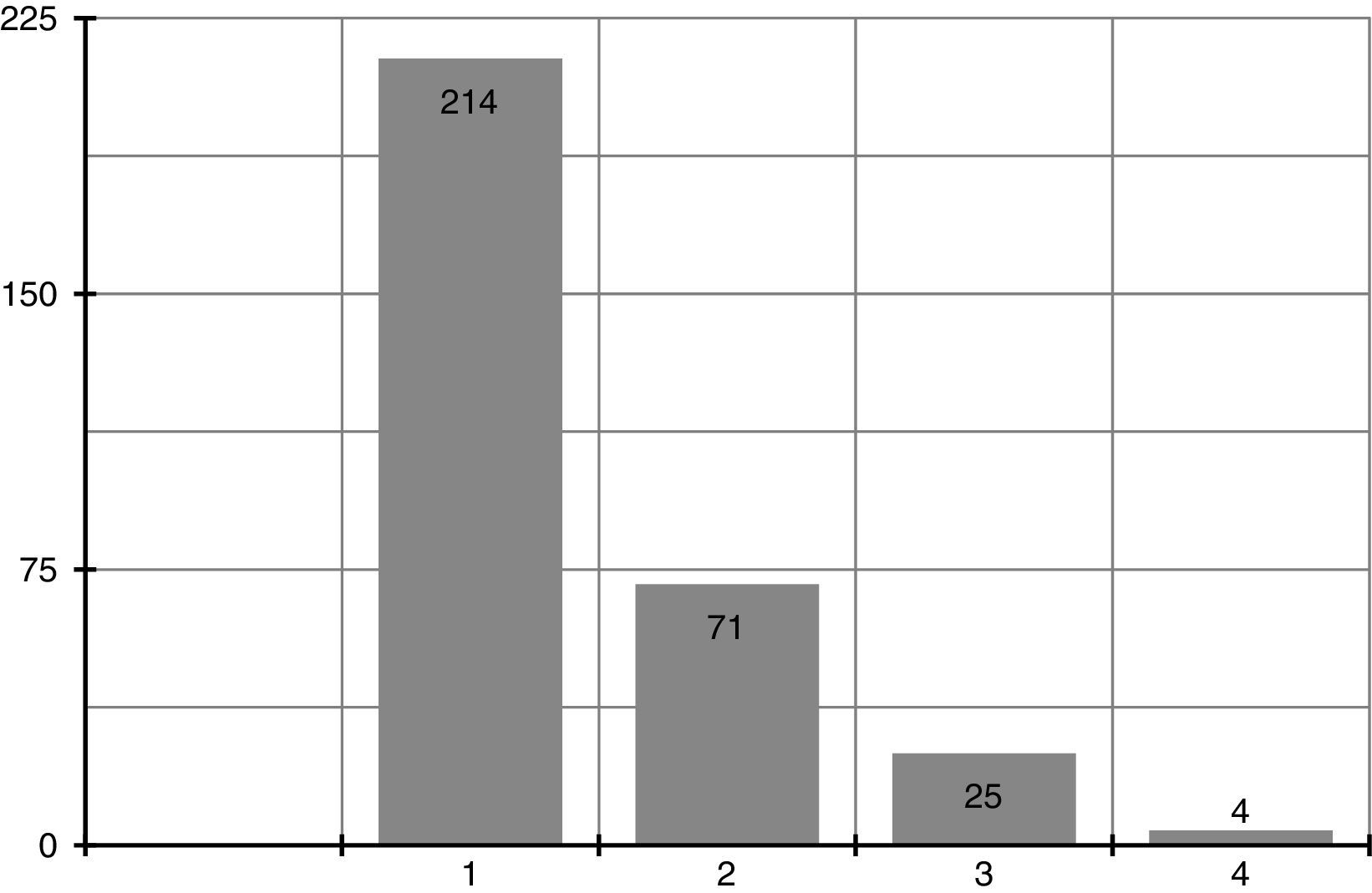
The number of wounds or impacts varies from 1 to 4, with a median of 1 (Fig. 4). Moreover, in 170 (54.1%) cases there was a single lesion, while in 144 (45.9%) cases 2 or more organs were affected. It was decided to exclude wounds that only affected the skin or soft tissues and ones which were simply sutured from this distribution, as they are not fully described in the clinical files of the patients.

A total of 532 lesions were reported, and a total of 518 procedures were performed. In 57.7% the lesion was in the abdominal cavity, where in order of frequency intestinal, gastric, hepatic and splenic lesions occurred. 29.8% of lesions were in the thoracic cavity, where the lungs and diaphragms were the most frequent sites of lesions. 8.5% of the lesions reported were vascular, among which those of the lower limbs stand out.
A total of 518 surgical procedures were performed, among which primary repairs to hollow viscera stand out, together with intestinal resections and anastomosis, intestinal shunts, thoracic catheterisation, splenectomies, hepatorrhaphies and vascular explorations with primary repairs and vascular grafts.
The most common associated lesions were fractures of the limbs, pelvis or spinal column, in 29 (5.5%) cases, with a certain degree of spinal injury.
In more detailed analysis of the lesions and procedures two points can be underlined: (1) (120) 92.3% of thoracic lesions were resolved by endopleural catheterisation, while only 10 (7.7%) required thoracotomy. Only 13 (10%) of complications arose here, among which retained haemothorax and empyema stand out. (2) of the lesions to the colon and rectum, primary repair or resection and anastomosis were only performed in 5 (6.1%) of cases, with 86.6% of intestinal shunts. The literature currently states that primary repair or resection and anastomosis can be used in the majority of lesions, regardless of how severe they are.
68 (21.7%) of cases required admission to the Intensive Care Unit, for a median duration of 7 days and an interquartile range of from 4.25 to 12.75 days. 171 (54.5%) of cases required blood transfusions, with a median number of 3 and an interquartile range of 2–5, up to a total of 728 units transfused in these 171 cases. If patients who received 5 units or more of blood are considered to be “polytransfused” then this applies to 58 (34%) of these cases.
In patient follow-up the most relevant actions were the closure of a colostomy or ileostomy, which were performed in 27 and 8 patients, respectively. In 3 cases of colostomy closure there was leakage from the anastomosis followed by death of the patient, and in 2 cases of closure of an ileostomy there was leakage from the anastomosis that was treated by a new intestinal shunt. It must be born in mind that our institution is a teaching hospital, so that the majority of these procedures were performed by interns in training, so that complications such as those described above may be expected. Additionally, other complications were reported such as retained haemothorax, dehiscence of the surgical wound, pancreatic fistula, infection of the surgical wound and thrombosis of a vascular graft, among others.
Another important datum refers to the 66 cases in which a surgical procedure was performed without lesions being found. 242 laparotomies were performed from January 2011 to December 2015, of which 41 (16.9%) found no lesion, as well as 22 (42%) vascular explorations that also found no sign of lesions.
When the mortality was examined in greater detail (n=48), the files of 31 cases were reviewed; the file had been cleared in the other cases. 60% of these cases occurred from 2010 to 2012, which were the most violent years. 45 (93.8%) of all these cases involved men. The majority of them were in the age range from 15 to 44 years old, with a median age of 30.5 years old (SD 13.2). 80% of these cases had 2 or more wounds, and the majority of them had multiple lesions. The anatomical sites affected the most often were the thorax and abdomen. There was a median of 9 days of hospitalisation and an interquartile range of from 4 to 16. Additionally, 39 patients required a stay in the Intensive Care Unit, with a median stay of 8 days and an interquartile range of from 4.25 to 15. 29 cases required blood transfusions, and 69% of patients required multiple transfusions. A total of 204 units of blood were transfused (a median of 6 with records of from 4 to 9), representing 28% of the total units transfused from 2011 to 2015. Of the lesions found, those affecting the duodenum stand out (2.3%), which had a high rate of mortality (66.6% of patients with duodenal lesions died).
DiscussionThe homicide rate in Mexico has ceased to decline. There was a significant upturn in its incidence from 2008 to 2010, although it has once again fallen in recent years.19
The number of gunshot wound cases admitted and treated in “Dr. José Eleuterio González” University Hospital from January 2005 to December 2015, corresponds to the incidence and rates of homicide by firearm at a national level, and it follows the same tendency over the years. There are many reasons for this increase, although there can be no doubt that the most important one has been the fight against organised crime.
Understanding the reasons for different levels of violence and most especially the increase in the levels of homicide by firearm is certainly complex. It requires analysis of the social, economic, political and cultural context that leads to this situation. There are high levels of impunity, insecurity, drug trafficking, social exclusion and unemployment, and it is also hard to access higher education. To achieve a marked and sustained reduction in homicide rates it would therefore be necessary to urgently implement public policies to strengthen our system of justice to reduce levels of impunity and corruption. It is necessary to implement a range of actions to combat the growing strength of drug cartels and to prevent crime. Moreover, strategies to reduce the consumption of drugs and alcohol have to be applied, to correct the social and economic deficiencies which exist in different parts of the country.
It is clear that the perception and feeling of insecurity has increased. We have experienced this in the state of Nuevo León, and in particular in the city of Monterrey from 2010 to 2012. It was during these years that our hospital went from receiving patients with multiple trauma or stab wounds to receiving increasing numbers of patients with gunshot wounds, giving rise to a new challenge for their management and treatment. Due to these tendencies, the interns in our institution have acquired skills and expertise that make them stand out over those in other state institutions, and the Surgery Department of our hospital should maintain this level.
“Dr. José Eleuterio González” University Hospital is now a centre in Nuevo León for the concentration of patients with gunshot wounds. This study made it possible to obtain data, together with the analysis of the frequency and distribution of these cases and draw inferences from them. These patients are a major public health problem in our population, and the large amount of economic, human and material resources needed to treat them has to be taken into account.20
Studies in the United States calculate an average cost of 17,000 dollars for each patient treated for gunshot wound.21 The cost of treating gunshot wound patients is both a social problem and a challenge for our healthcare systems. It is vitally important to analyse the cost per patient to create trustworthy data and thereby be able to dispose of the evidence that is necessary create social programmes to reduce the levels of violence in our environment and thereby lower the costs of the same for our institutions.
The demographic variables analysed, chiefly sex and age, correspond to the tendency at a national level for homicides by firearm. A study in Ciudad Juárez (Chihuahua) General Hospital22 reports a general mortality of 9% and an average duration of hospitalisation of 11 days. These statistics are very similar to ours, which report a mortality rate of 7.9%. If we divide mortality according to anatomical areas, it stands at 5% for neck lesions, 8.6% for the abdomen and 12.3% for lesions affecting the thorax and abdomen. In our institution the average duration of hospitalisation was 12.1 days, a statistic that is very similar to those reported in the literature.23
It is clear from the data obtained by statistical analysis that morbimortality increases notably in patients with 2 or more wounds, those with 2 or more anatomical areas affected, those with multiple lesions to target organs, those who received multiple transfusions and those admitted to the Intensive Care Unit during hospitalisation. It is also important to point out that 16.9% of laparotomies and 42% of vascular explorations found no evidence of lesion. This raises the possibility of changing the initial approach in patients, being more conservative and using imaging studies that help to reduce the percentage of unnecessary surgical operations, on condition that the patient is haemodynamically stable.
It is evident that new computer systems have helped to improve the organisation and use of clinical files to obtain data and thereby gain reliable statistical records of gunshot wound lesion characteristics. These in turn will stimulate research projects in this field.
It also has to be said that the information not recorded while treating these patients includes data as important as the calibre of the projectile and proper classification of wounds. The lack of uniformity in how they are described means that studies such as this one require a great effort in data gathering. It is suggested that a physical evaluation format for gunshot wound patients be developed by those departments who see them, to make it possible to follow them up during hospitalisation and encourage the generation of more detailed multidisciplinary research projects.
Another very important point is the training of doctors and interns in the management and treatment of these patients. The information in this study may be used to develop programmes for general surgery interns in our hospital, centring on the types of lesions and anatomical sites which are involved the most often, as well as the most common surgical procedures, as reported in this work.
The limitations of this study are that it is retrospective, that it only includes patients admitted for general surgery and that it focuses on lesions to the abdomen and thorax.
ConclusionThe incidence of hospital admissions due to gunshot wounds has increased drastically over recent years. This is mainly due to organised crime, which has major social repercussions as well as leading to a serious challenge for healthcare institutions which treat these patients in “Dr. José Eleuterio González” University Hospital of Nuevo León Universidad Autónoma, one of the main centres in the north of the country.
It is fundamental to prepare studies that analyse the epidemiology of these lesions to gain a clearer idea of their socioeconomic implications for healthcare systems. It is also necessary to understand their pattern of presentation, the most frequent anatomical sites and the treatment, prognosis and morbimortality of gunshot wounds.
Study of the variables associated with these lesions will also allow us to gain greater comprehension and facilitate effective interventions for them.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Cavazos JC, Palacios-Zertuche J, Reyna-Sepúlveda F, Álvarez-Villalobos N, Alatorre-López L, Muñoz-Maldonado G. Epidemiología de las lesiones por proyectil de arma de fuego en el Hospital Universitario “Dr. José Eleuterio González” de la Universidad Autónoma de Nuevo León. Cir Cir. 2017;85:41–48.