


Ectopic gastric mucosa has been described in different locations of the digestive tract, but that of the rectum is the least frequent.
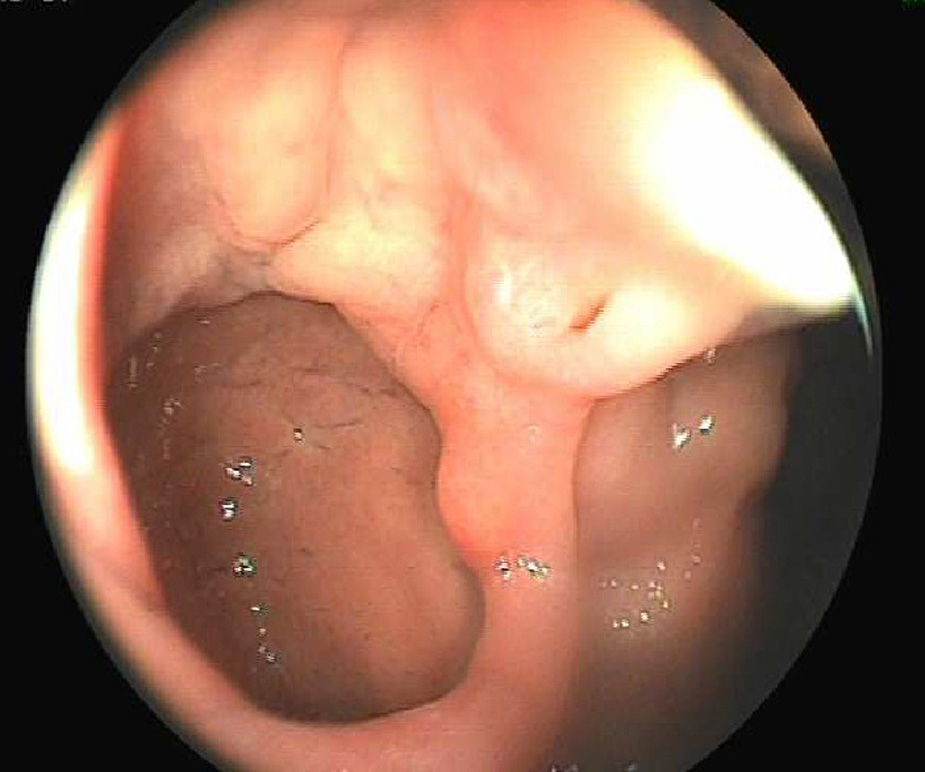
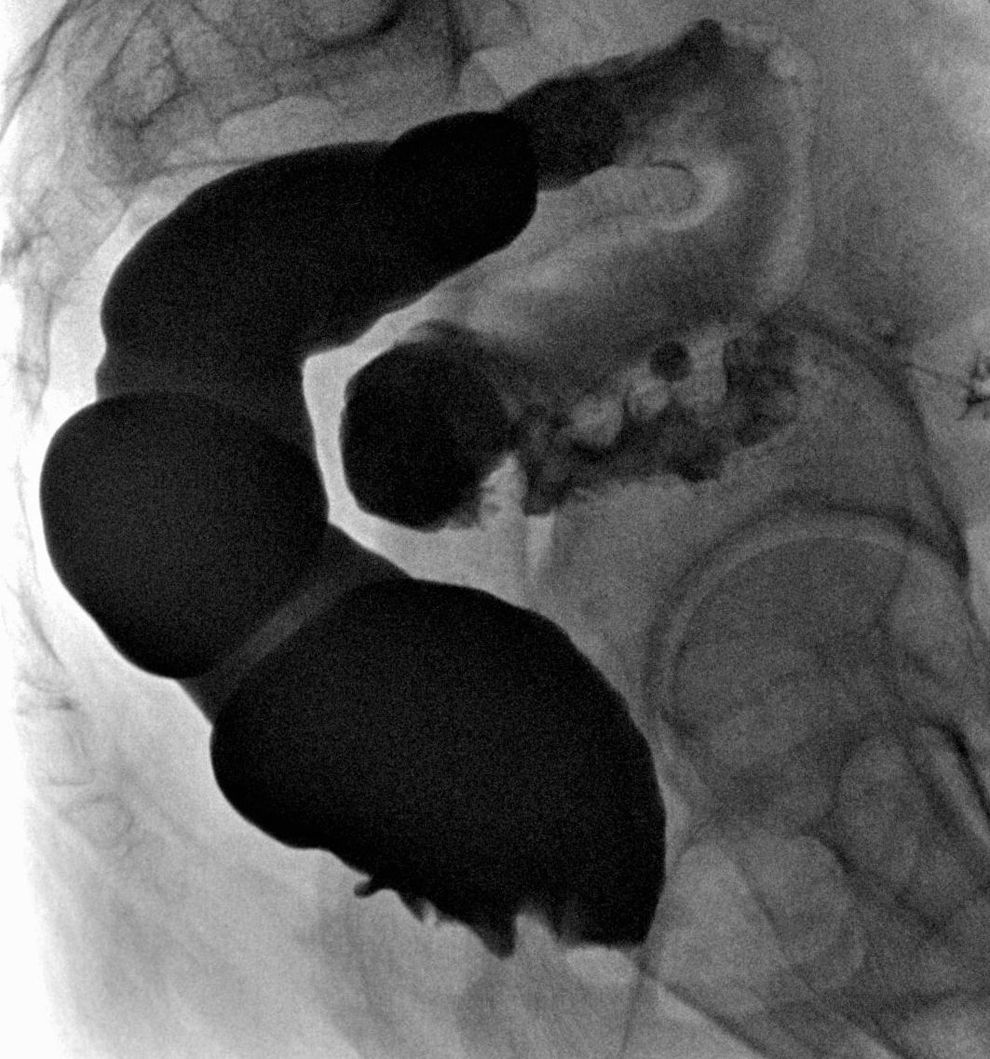
Clinical caseThe case is described of a 48 year-old woman being investigated by the gastrointestinal department due to rectal bleeding and rectal tenesmus. Colonoscopy showed a diverticular cavity 3cm, which was reported by histology as fundic-type heterotopic gastric mucosa. Barium enema and abdominopelvic CT showed a diverticular image at level of the right posterolateral wall of the rectal ampulla.
Trans-rectal diverticulectomy was performed with primary closure of the resulting mucosal defect. The surgical specimen showed areas of gastric epithelium with no signs of atypia.
ConclusionsIt is not known whether the origin of heterotopic gastric mucosa occurs during foetal development or is the result of abnormal regeneration under inflammatory conditions. It is usually clinically asymptomatic or presents as haematochezia, especially in cases where gastric acid is being produced. In these cases there must be an initial treatment with proton pump inhibitors, although the definitive treatment is always surgical or endoscopic excision of the mucosa.
La mucosa gástrica ectópica se ha descrito en distintas localizaciones del tubo digestivo, de todas ellas, el recto es la más infrecuente.
Caso clínicoMujer de 48 años estudiada por el servicio de digestivo debido a rectorragias y tenesmo rectal. La colonoscopia apreció una cavidad diverticular de 3cm, cuya anatomía patológica se informó de mucosa gástrica heterotópica de tipo fúndica. El enema opaco y el reporte de la tomografía computada abdominopélvica demostraron una imagen diverticular situada a nivel de la pared posterolateral derecha de la ampolla rectal.
Se practicó diverticulectomía por vía endoanal con cierre primario del defecto mucoso resultante. La pieza quirúrgica evidenció áreas de epitelio gástrico, sin signos de atipia.
ConclusionesSe ignora si el origen de la mucosa gástrica heterotópica se produce durante el desarrollo fetal o es el resultado de una regeneración anómala, bajo condiciones inflamatorias. Clínicamente suele ser asintomática o presentarse como hematoquecia, especialmente en los casos en que es productora de ácido gástrico; en estos casos, debe hacerse un tratamiento inicial con inhibidores de bomba de protones, aunque el tratamiento definitivo es siempre la escisión quirúrgica o endoscópica de la mucosa.
Although the presence of heterotopic gastric mucosa has been described from the tongue to the anus, it is rarely located in the rectum. Since it was first described in 1939 by Ewell and Jackson1 barely fifty cases have been published on ectopic gastric mucosa in the rectum.
Clinical caseWe present the case of a 48 year-old, examined in our hospital's digestive unit for rectal bleeding and tenesmus. She had a history of smoking and arterial hypertension. She had no history of colitis or rectal trauma.
The results of complementary tests showed haemoglobin levels of: 10.7g/dl and normal carcinoebryonic antigen (CEA), colonoscopy showed a diverticular cavity of 3cm (Fig. 1) whose pathologic anatomy reported heterotopic gastric mucosa, fundic in type. There was no evidence of colonisation by Helicobacter pylori. Opaque enema and abdominopelvic computed tomography showed a diverticular image 3cm in depth, situated at the level of the right posterolateral wall, in the most caudal section of the rectal ampulla (Fig. 2). Gammagraphy did not detect any other foci of uptake in the area.


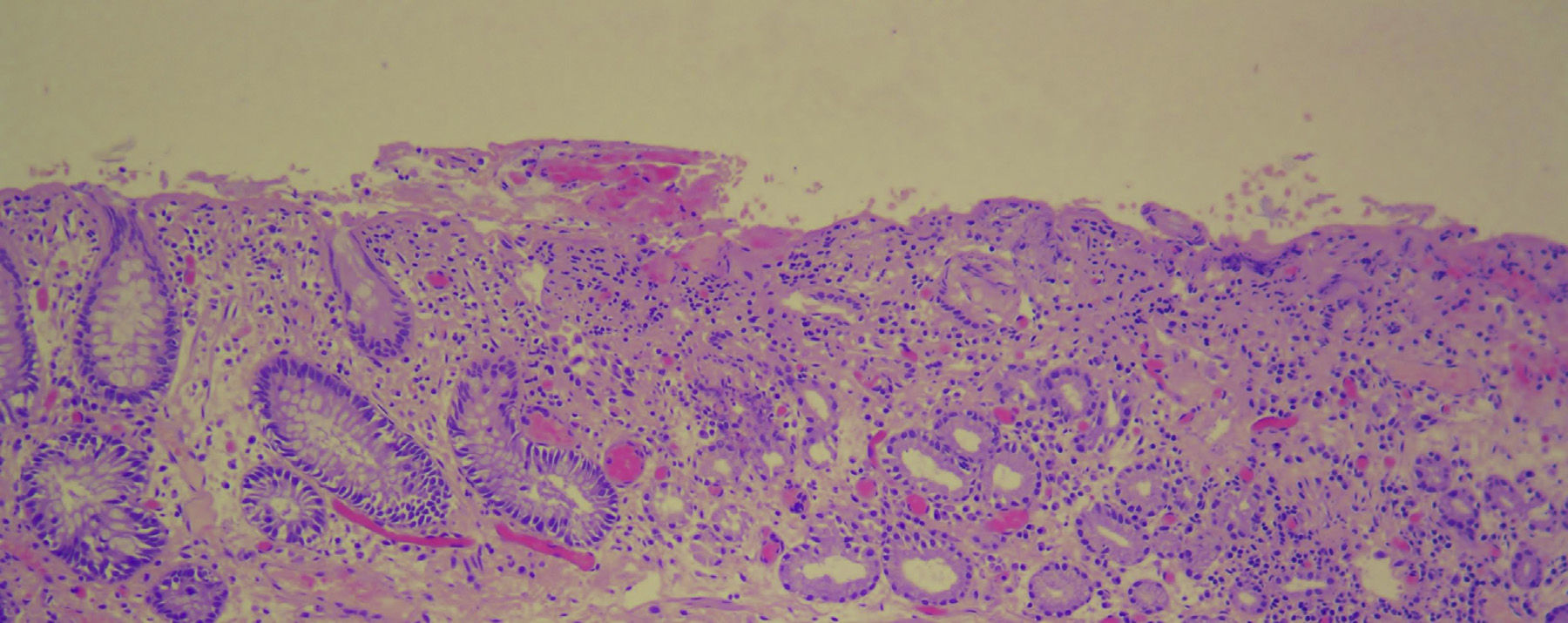
In this context the patient was evaluated by the digestive unit in general surgery and it was decided to operate. The procedure was undertaken via the endoanal route, and a diverticulectomy was performed with primary closure of the resulting mucosal defect. The surgical sample showed areas of gastric epithelium with mucosecretory, parietal and principal cells with no signs of atypia. Transition with the rectal mucosa was abrupt without dysplastic or inflammatory changes (Fig. 3).
 and colonic-type mucosa with Lieberkuhn crypts (to the right of the image).")
The patient is currently asymptomatic and undergoes periodic monitoring in consultations.
DiscussionEctopic gastric mucosa has been described in different areas of the digestive tract (tongue, oesophagus, duodenum, pancreas, bile duct, intestine), mediastinum2 and even the scrotum3 and spinal cord.4 Within heterotopia of the digestive tract, the anus-rectum is one of the least common sites, with barely 48 cases described in the references.
Its aetiology is not well known, and there are various theories which attempt to explain it. Some authors claim that it occurs between the fourth and seventh week of foetal development. According to Morrison,5 due to an erroneous differentiation of the pluripotent stem cells of the endodermis, whereas Wolff6 considers that it generates due to a failure in the descent of the proximal intestine. Another possibility is that it is the result of an anomalous regeneration under inflammatory conditions, such as gastric metaplasia in Barrett's oesophagus.7
It predominates in males with an incidence peak in the second decade of life, and in some cases is a chance endoscopic finding, during a study of anaemia or irritable bowel. More than half of symptomatic cases present: painless haematochezia, less frequently anal pain, abdominal pain, melena stools, perineal fistula or even rectovesical fistula.8
The findings usually present in the posterolateral rectal wall at more than 5cm from the anal margin (62%)9 in the form of: polyps, diverticuli or ulcers.10 These endoscopic findings can be confirmed with more than 90% sensitivity by uptake of Tc99m.
Histologically, 90% present isolated gastric mucosa, however, 2 cases have been described where the gastric mucosa was associated with pancreatic tissue and in 3 cases with salivary glands. Heterotopic gastric mucosa has been classified according to its area of provenance, finding: 50% fundic mucosa, 13% gastric body and 3% pylorus; half of the remainder presented association of mucosa from various gastric regions and the in the other half the area of provenance could not be defined.10
Heterotopic gastric mucosa can produce gastric acid, in which case it is important that it is initially treated with proton bomb inhibitors or H2 antihistamines to prevent the development of rectal bleeding. In cases associated with H. pylori an eradication treatment should be prescribed as the first therapeutic option. In any case, when the acute episode of ulcer or gastritis has been resolved, surgical excision or endoscopy of the mucosa is indicated as the definitive treatment.
ConclusionThis report describes a case of heterotopic gastric mucosa on a rectal diverticulum. It is a rare surgical disease and there is a much debate as to its origin. Clinically it can start as haematochezia or it can be asymptomatic. From a histological perspective there are different patterns; the most usual being isolated gastric mucosa which is fundic in type. In all cases the definitive treatment is endoscopic or surgical excision, as with our case.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Colsa-Gutiérrez P, Kharazmi-Taghavi M, Sosa-Medina RD, Berrío-Obregón JI, Ingelmo-Setién A. Mucosa gástrica heterotópica en el recto: reporte de un caso. Cirugía y Cirujanos. 2016;84:158–161.