


Spontaneous sub-capsular or peri-renal haemorrhage (Wunderlich syndrome) is a rare condition that involves a diagnostic challenge. In many cases, bleeding leads to haemodynamic instability that may be life threatening. Therefore, it is important to have a high clinical suspicion for timely action.
ObjectiveThis paper highlights the experience of the Urology Department of the Centro Médico Nacional de Occidente del Instituto Mexicano del Seguro Social.
Material and methodsRetrospective study of consecutive non-randomized sampling. The Emergency Service Registry was reviewed for all admissions from 1 January 2010 to 31 December 2013 to identify patients with non-traumatic spontaneous retroperitoneal haemorrhage. Patient charts were reviewed to determine sex, age, vital signs, laboratory and imaging results, associated diseases, management, and outcomes.
ResultsA total of 11 patients met the inclusion criteria for the study. All patients were received in the Emergency Department referred from secondary care hospitals. None of them were referred with a diagnosis of spontaneous retroperitoneal haemorrhage. The diagnosis was made in 100% of patients with abdominal CT scan. All patients received urgent surgical management on the day of admission due to haemodynamic instability. Ten patients underwent nephrectomy. Histopathological findings included, among others, angiomyolipoma, renal carcinoma, and metastatic hepatocellular injury.
ConclusionsSpontaneous retroperitoneal haemorrhage is a lethal condition if not detected on time. The abdominal CT scan is the most accurate diagnostic method for detection. Surgical management is necessary in patients with haemodynamic instability.
La hemorragia subcapsular o perirrenal espontánea (síndrome de Wunderlich) puede condicionar inestabilidad hemodinámica con riesgo para la vida. Es una enfermedad rara que implica un reto diagnóstico; por lo que debe sospecharse su diagnóstico para actuar a tiempo.
ObjetivoPresentar la experiencia adquirida del servicio de Urología de la Unidad Médica de Alta Especialidad del Hospital de Especialidades del Centro Médico Nacional de Occidente del Instituto Mexicano del Seguro Social.
Material y métodosEstudio retrospectivo con muestreo consecutivo no aleatorizado. Se revisaron los ingresos en el servicio de Urgencias de enero de 2010 a diciembre de 2013 para identificar los casos con diagnóstico de hemorragia retroperitoneal espontánea no traumática. De los expedientes se recabaron los siguientes datos: edad, sexo, signos vitales, resultados de laboratorio, métodos de diagnóstico por imagen, enfermedades asociadas, tratamiento y pronóstico.
ResultadosUn total de 11 pacientes cumplieron los criterios de inclusión. Todos los pacientes fueron recibidos en el servicio de Urgencias, y referidos de hospitales de segundo nivel. El diagnóstico se realizó en el 100% de los pacientes con tomografía computada abdominal. Todos los pacientes recibieron tratamiento quirúrgico urgente el día de la admisión debido a la inestabilidad hemodinámica; a 10 se les realizó nefrectomía; los hallazgos histopatológicos incluyeron angiomiolipomas, carcinoma renal y lesión metastásica de hepatocarcinoma, entre otras.
ConclusionesLa hemorragia retroperitoneal espontánea es una entidad patológica letal si no se detecta a tiempo. La tomografía computada es el método diagnóstico más preciso para su detección. El tratamiento quirúrgico es indispensable en pacientes con inestabilidad hemodinámica.
Spontaneous sub-capsular or perirenal haemorrhage is a relatively rare pathologic entity and hard to diagnose.1 In 1856, Wunderlich described for the first time the clinical features of spontaneous renal haemorrhage characterised by the low blood flow effect in the sub-capsular or perinephric cavity.2 The definitive treatment is indicated when the retroperitoneal haemorrhage conditions haemodynamic instability and the need for haemotransfusion in the patient. After the acute episode is resolved, other therapies are recommended for the purposes of preventing recurrent bleeding and the specific treatment.1,3 Most commonly reported aetiologies are: renal cell carcinoma and angiomyolipoma; less common causes include: autoimmune, vascular, infectious diseases, use of anticoagulants, adrenal carcinoma, adrenal myelolipoma and chronic renal failure.3–7
Retroperitoneal haemorrhage may be fatal for the patient if not diagnosed in time. There should be a high suspicion index, since there are other diseases which may have the same symptomatology.
Objective: review the experience of the Urology service as regards patients treated with diagnosis of spontaneous retroperitoneal haemorrhage admitted into the casualty department at Hospital de Especialidades Centro Médico Nacional de Occidente del Instituto Mexicano del Seguro Social, for the purposes of showing statistical data, prognosis, morbidity and mortality, as well as the applied treatment.
Material and methodsRetrospective study with consecutive non-randomised sampling. The database was reviewed (IMSS VISTA) for the purpose of detecting patients with diagnosis of spontaneous retroperitoneal haemorrhage admitted into the emergency department from 1 January 2010 to 31 December 2013. Medical notes and pathology reports were used to select 11 patients who met the inclusion criteria. Full demographic data were taken, such as: gender, age, progression time of symptoms, characteristics of the symptoms, comorbidity, pathological, non-pathological personal history and immediate clinical condition. There were 2 inclusion criteria: a) spontaneous retroperitoneal haemorrhage diagnosed through clinical assessment and abdominal computed tomography; b) a histopathological report which confirmed the renal haemorrhage diagnosis.
Exclusion criteria: cases secondary to trauma, use of anticoagulant therapy; however, in our series, no patient presented this condition.
For the analysis of the database, a simple descriptive statistic was used, namely raw numbers, proportions and central trend measurements.
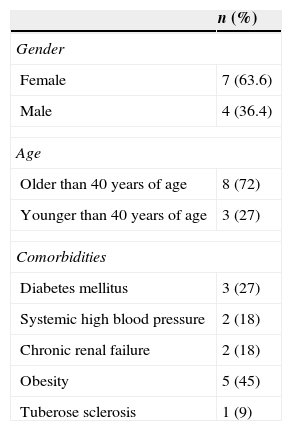
Results11 patients with a diagnosis of spontaneous retroperitoneal haemorrhage were included in the study, 4 men and 7 women (36.4% and 63.6% respectively), with an average age of 42.9 years (SD 17.70, 25–75). 100% of patients were admitted through the casualty department.
All patients presented pain in the affected flank, general discomfort and nausea. Only one of the patients had a fever. None were referred to this Department with diagnosis of spontaneous retroperitoneal haemorrhage. The referral diagnosis in 5 patients was reno-ureteral colic and none had imaging studies. In 4 patients, there was a diagnosis of renal abscess based on tomographic findings. The rest were sent with diagnosis of pyelonephritis and acute abdominal pain.
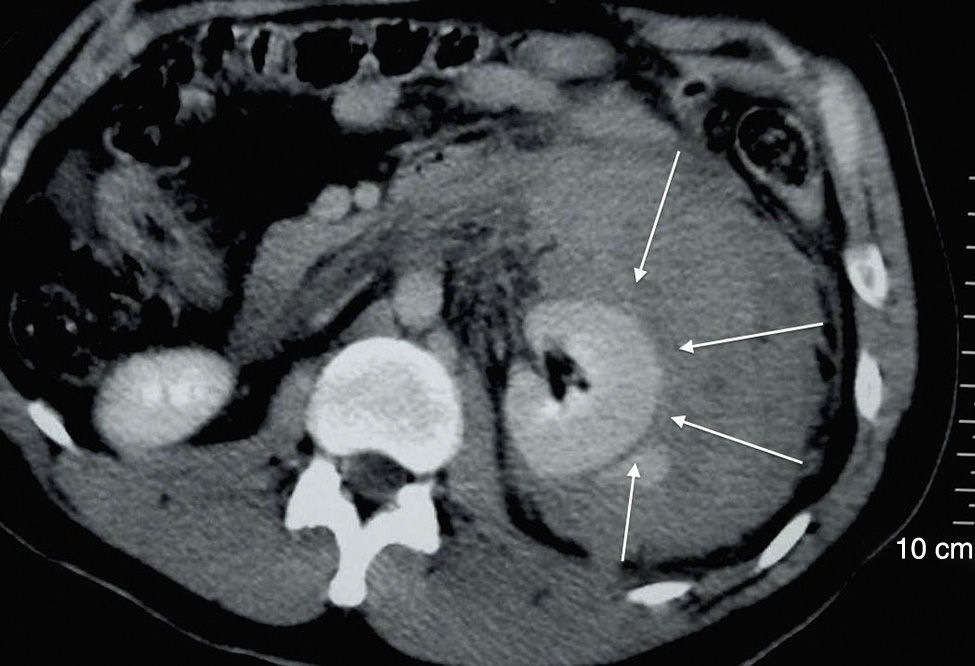
Upon admission into the casualty department and after clinical assessment, a simple abdominopelvic computed tomography was indicated to complete the study protocol. In all patients the retroperitoneal haemorrhage diagnosis was after the tomography (Fig. 1).
.")
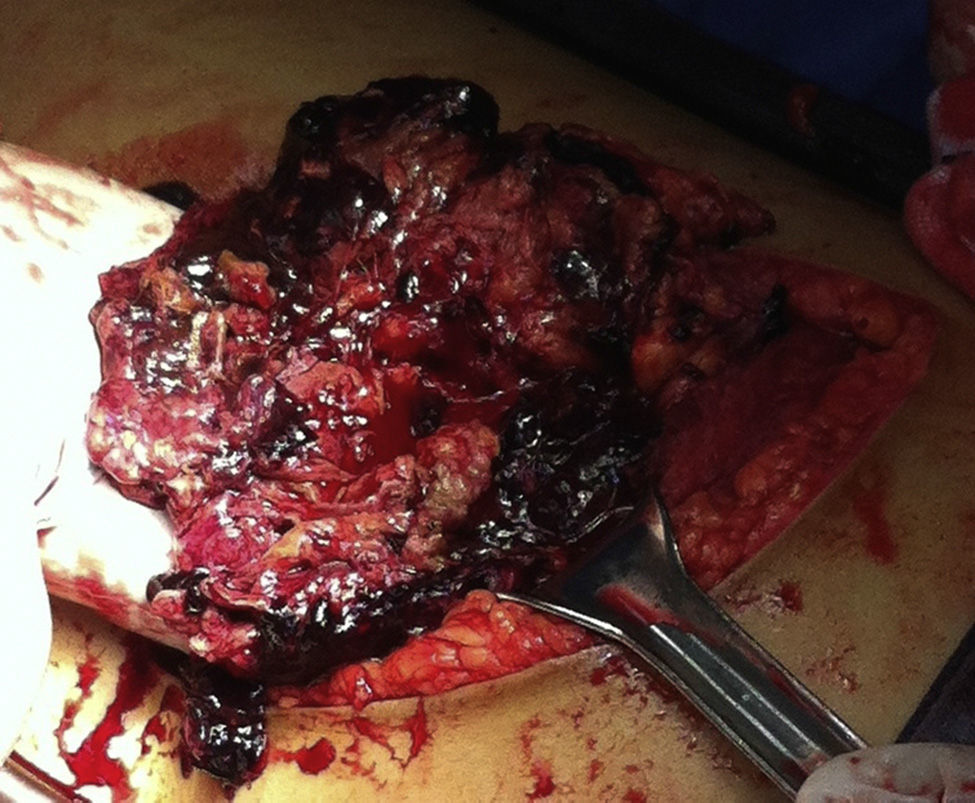
Given the haemodynamic instability, emergency surgical exploration was necessary in all cases. In 7 patients, the affected side was the left side (Fig. 2). No intraoperative complications were reported, although all patients required blood transfusion.

As previously mentioned, most patients were women (63.6%). Personal comorbidity histories were: 3, diabetes mellitus (27%); 2, systemic blood hypertension (18%); 2, chronic renal failure (18%); 5, obesity (45%); and one patient with tuberose sclerosis (9%) (Table 1).
Demographic characteristics of the group of patients with Wunderlich syndrome.
| n (%) | |
|---|---|
| Gender | |
| Female | 7 (63.6) |
| Male | 4 (36.4) |
| Age | |
| Older than 40 years of age | 8 (72) |
| Younger than 40 years of age | 3 (27) |
| Comorbidities | |
| Diabetes mellitus | 3 (27) |
| Systemic high blood pressure | 2 (18) |
| Chronic renal failure | 2 (18) |
| Obesity | 5 (45) |
| Tuberose sclerosis | 1 (9) |
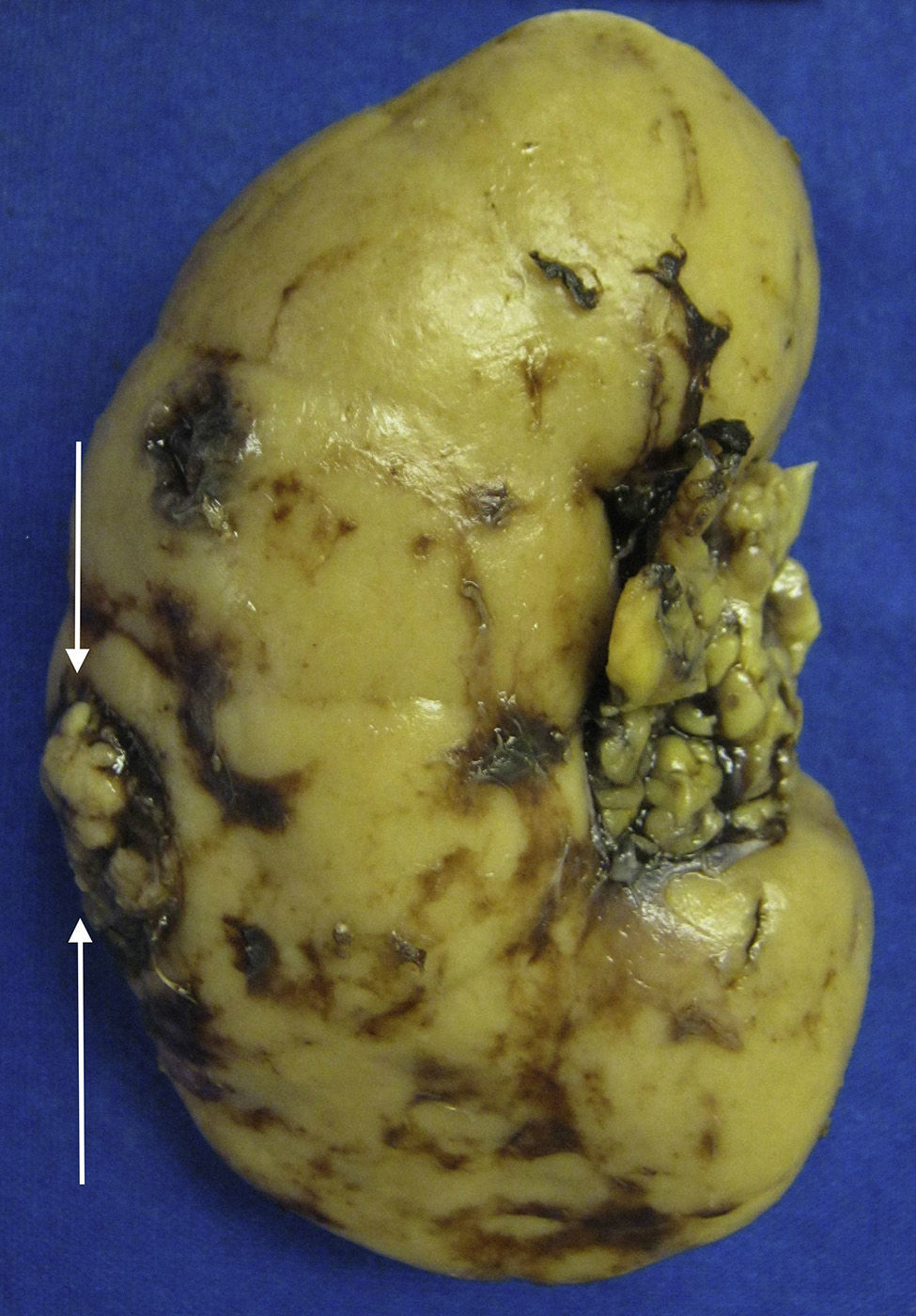
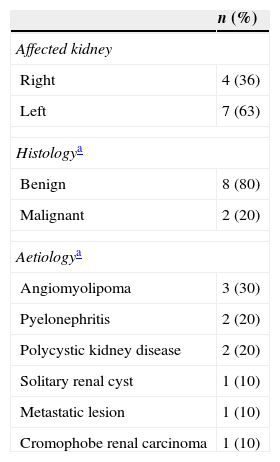
Only 10 nephrectomies were performed in patients treated. No nephrectomy was needed for one of the patients, since the bleeding site was controlled through suture of the renal cortex, which was affected by acute infection. The Pathology department (Table 2) reported: 3 angiomyolipomas (30%), 2 pyelonephritis, 2 with multiple renal cysts, one solitary renal cyst; 2 reported malignity (one, cromophobe renal carcinoma and another with metastatic hepatocellular carcinoma) (Fig. 3).
Histopathology findings in nephrectomy pieces of patients with Wunderlich syndrome.a

In 2002, Zhang et al.1 reported 165 cases obtained from a review of 47 articles from the USA (16), Europe (15) and Asia (16). The study was carried out in a 14-year period (1985–1999). The number of reported cases in each section varied from one to 18. A higher percentage of men than women was observed (55 vs. 45). The radiological evaluation included 135 cases with computed tomography, 100 with ultrasound, 5 with magnetic resonance and 81 with angiography. Several patients had multiple studies made. Their results showed that the abdominopelvic computed tomography evidenced the retroperitoneal haematoma in 100% of patients. The ultrasound was useful for the diagnosis in 56 (56%) and magnetic resonance in 5 (100%). The angiography showed active bleeding in only 11 cases. In the review of these 47 articles, Zhang et al.1 estimated the aetiology in 154 cases (93.33%); the rest were reported as aetiology idiopathic (6.66%). As regards benign and malignant neoplasms as the main causes of retroperitoneal haemorrhage, 101 patients were counted, 48 of whom (29.09%) were angiomyolipomas and 43 (26.06%) renal cells carcinoma. The rest of neoplasms (6.06%) included: metastatic disease (4), sarcoma (one), oncocytoma (one), adenoma (2) and myelolipomas (2). The following most common aetiology was vascular disease in 28 cases (17%). Severe pyelonephritis was the aetiology in 4 patients (2.4%). 21 (12.7%) cases were classified as miscellaneous associated to causes such as: cyst rupture, nephrosclerosis and pre-eclampsia. The study reported 113 nephrectomies, that is to say, 68.48% of cases. The simple evacuation of the perirenal haematoma was reported in 17 cases (10.3%). Regarding our review, the total number of cases was 11 patients. This equals 6.66% of the total sample analysed by Zhang et al.1 But it is worth noting that patient limits in the 47 articles were from one to 18, and therefore our study is within the average of reported cases. There is a difference regarding gender, since there were more women than men in our review (63.63% vs. 36.36%). All patients in our study were diagnosed precisely with computed tomography, achieving a 100% precision with this imaging method. The nephrectomies percentage in our study is higher in proportion to that recorded by Zhang et al.1 (90.9% vs. 68.48%). This difference is because in 10 of the 11 cases the kidney was found with relevant damage and uncontrollable bleeding secondary to the lesion in the parenchyma. 90.9% of our definitive diagnosis was through histopathology. One of the cases did not require nephrectomy for the causes referred above.
Hernández et al.3 reported the management of retroperitoneal haemorrhage with laparoscopic approach in 4 patients, and it is concluded that laparoscopic exploration offers an alternative to open surgery, although the procedure can be complicated secondary to the fibrosis. The laparoscopic approach was not considered a viable option for any of the patients in our study due to the degree of retroperitoneal haemorrhage presented and the risk of sudden decompression, in addition to the fact that laparoscopic vascular control is harder in patients who are haemodynamically unstable and the procedure, in general, is technically more complex.
The general consensus with other studies reveals that simple abdominopelvic computed tomography has 100% sensitivity for the diagnosis and that ultrasound is an option only if tomography is not available, since scientific evidence reports a sensitivity of up to 76.4% for the detection of retroperitoneal haemorrhage.8 Magnetic resonance can offer the same sensitivity as computed tomography for the diagnosis, although with no additional advantage, since its cost is higher, availability may be lower and the time of the study is longer.
On the other hand, the meta-analysis described by Zhang et al.1 reported almost the same proportion of nephrectomies as our study. In fact, the proportion in relation to renal cells carcinoma, angiomyolipomas and other causes for retroperitoneal haemorrhage was very similar.
It is also important to mention that our series presented a case of metastatic hepatocellular carcinoma as aetiology for retroperitoneal haemorrhage, a condition that has been reported only once in the medical bibliography.9 We are probably presenting the second case, of a 33-year-old man with primary hepatocellular carcinoma who began with pain in flank 6h before attending the casualty department. The tomography showed left retroperitoneal haemorrhage (Fig. 2). The surgery was necessary given the medical condition. A simple left nephrectomy was carried out as treatment and the pathology department reported metastatic hepatocellular carcinoma in the left kidney (Fig. 3).
ConclusionSpontaneous retroperitoneal haemorrhage is a rare condition and hard to identify, given its similarity in the clinical symptoms with other pathologic entities. Delay in diagnosis may be lethal for the patient. The suspicion index should be high in patients admitted to the casualty department with sudden flank pain with a few hours of progression, anaemia and haemodynamic instability. The abdominopelvic computed tomography has proven to be the best imaging method to detect it. Prompt acknowledgement is a fundamental factor in establishing specific management. Surgery, as the gold standard, shows absolute efficacy as definitive treatment and offers a favourable prognosis.
Conflict of interestThe authors declare that there are no conflicts of interest.
Please cite this article as: Sierra-Díaz E, Belmonte-Hernández MV, Villanueva-Pérez MA, García-Gutiérrez M. Hemorragia retroperitoneal espontánea no traumática: efecto del diagnóstico preciso y oportuno. Cir Cir. 2015;83:206–10.