




Granulomatous appendicitis is a rare cause of acute abdomen. Its aetiology can be infectious, non-infectious or idiopathic, and its presentation is similar to symptoms of acute abdomen due to appendicitis.
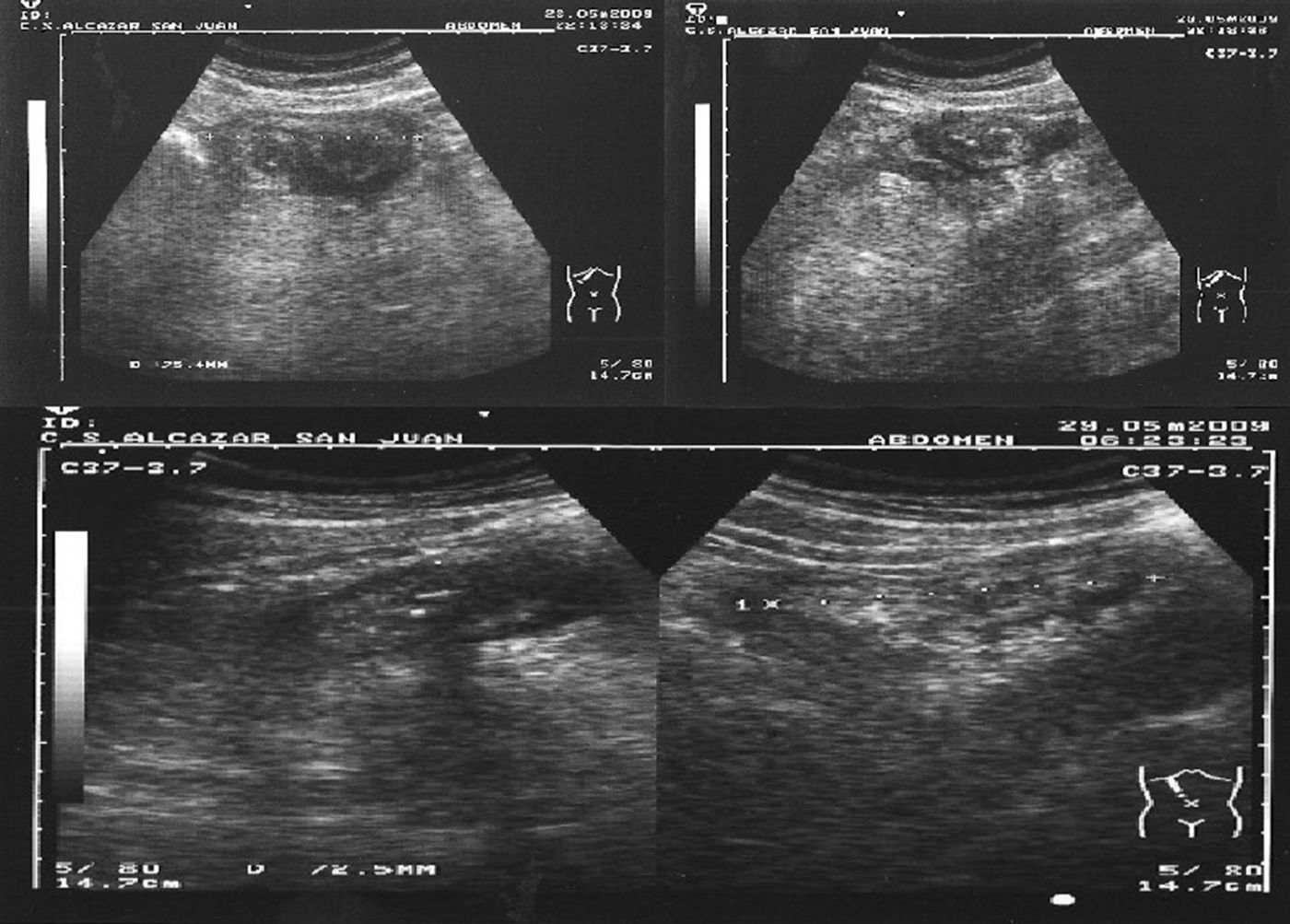
We present the case of a 32-year-old male with no prior history of interest who reported pain in the right hemiabdomen. He had had diarrhoea the week before, which lasted 48h. He had experienced no other symptoms or fever. During the physical examination, the patient presented pain upon deep palpation of the right flank, with no guarding or peritonitis. Lab workup demonstrated leucocytosis with neutrophilia and elevated acute-phase reactants. Abdominal ultrasound showed evidence of a subhepatic “pseudokidney” image, compatible with inflammation of the cecal appendix (Fig. 1).

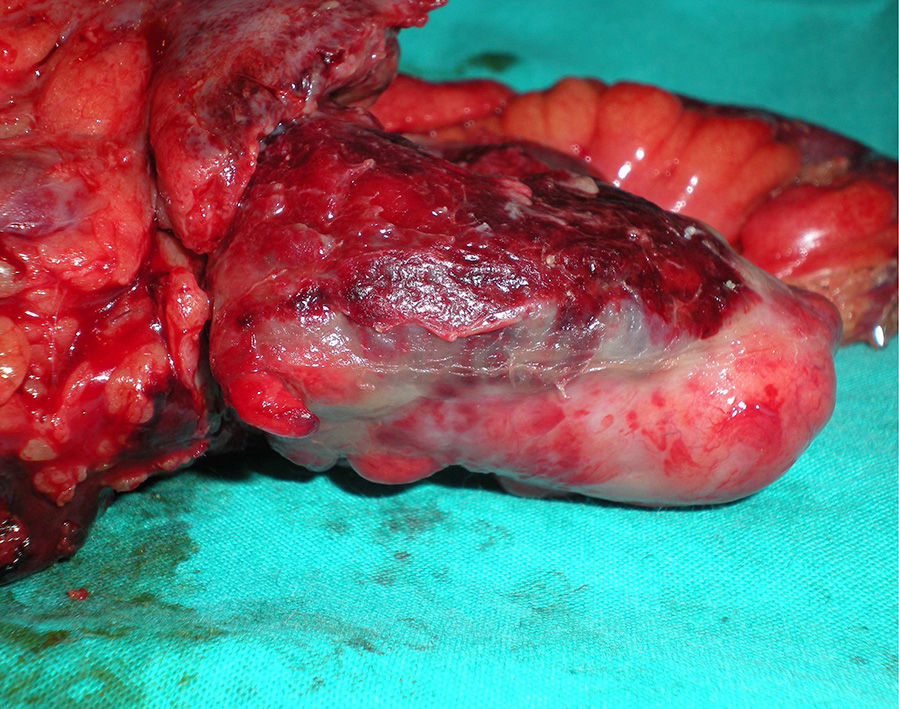
With a suspected diagnosis of acute appendicitis, the patient underwent emergency surgery, which revealed an ileocecal mass; the cecal appendix could not be identified, and there were no signs of peritonitis. Given these findings, ileocecal resection was performed (Fig. 2).

Microscopic study of the surgical specimen demonstrated a transmural inflammatory infiltrate with lymphoid follicles, confluent epithelioid granulomas and suppurative centres, indicative of granulomatous inflammation. These histology findings can be found in Yersinia infection as well as intestinal tuberculosis. After PAS and Ziehl–Neelsen staining of the specimen, which were negative, we arrived at the diagnosis of granulomatous acute appendicitis due to Yersinia.
Afterwards, the progress of the patient's condition was favourable, and he was discharged on the 8th day post-op. During the outpatient follow-up, and after receiving the pathology report, the patient underwent ambulatory Mantoux testing and chest radiograph, which excluded the presence of tuberculosis. Moreover, he never developed symptoms to suggest the presence of Crohn's disease.
Granulomatous inflammation of the appendix is a rare entity with a frequency of less than 2% of appendectomies.1–3 Its aetiology includes non-infectious and infectious causes, which are responsible for 38 and 62% of cases, respectively.3 Among the non-infectious causes, there are cases of diverticulitis, Crohn's disease, foreign-body reactions, tumours and sarcoidosis. Infectious causes are the result of Yersinia, Mycobacterium tuberculosis and other microorganisms.4,5
Approximately 5 and 10% of patients with granulomatous appendicitis will develop Crohn's disease in their lifetimes.1,6,7
Yersinia infection represents up to 25% of granulomatous appendicitis.7 There are 2 species of this enterobacteriaceae: Yersinia enterocolitica and Yersinia pseudotuberculosis. From a clinical standpoint, they are conditions whose presentation does not differ from acute appendicitis, although they are usually more insidious.4,5 Lab studies provide little data and specific serology should be done at the onset of symptoms as it turns negative shortly after appendectomy.4
Imaging studies do not provide specific data. Abdominal ultrasound can indicate the diagnosis of acute appendicitis.8 Furthermore, in select cases, computed tomography studies can show a thickened appendix as well as increased density of the surrounding soft tissue, which are findings that can lead to the diagnoses of granulomatous appendicitis, neoplasms or lymphoma of the appendix.9
The definitive diagnosis of this entity should be based on histology. The granulomatous inflammation is characterised by the presence of activated macrophages, known as epithelioid histiocytes, in addition to the presence of multinucleated giant cells, crypt abscesses, neural hyperplasia and lymphangiectasia.4,10 Crohn's disease involves the presence of non-necrotising epithelioid granulomas, aggregation of activated T lymphocytes and mucosal ulcers.4 However, as in the case we present, Yersinia infection causes granulomas with central necrosis and suppuration with formation of microabscesses, very similar to those found in intestinal tuberculosis.3,10 This latter condition also gives rise to confluent caseating granulomas, and this diagnosis should be ruled out with specific techniques.
Other types of granulomatous appendicitis are unusual. Mucinous neoplasms, foreign bodies in the appendix and actinomycosis can be accompanied by a granulomatous reaction, but specific histologic findings will determine the diagnosis in all cases.4
Surgical treatment of granulomatous appendicitis is curative. Notwithstanding, it is recommended to follow up these patients because of the possibility of developing Crohn's disease.2,4,7
Conflict of InterestThe authors have no conflict of interests.
Please cite this article as: Alhambra Rodríguez de Guzmán C, Morales Marín VJ, Salvelio Picazo Yeste J, Moreno Sanz C. Apendicitis granulomatosa: una causa infrecuente de abdomen agudo. Cir Esp. 2015;93:e119–e121.
