




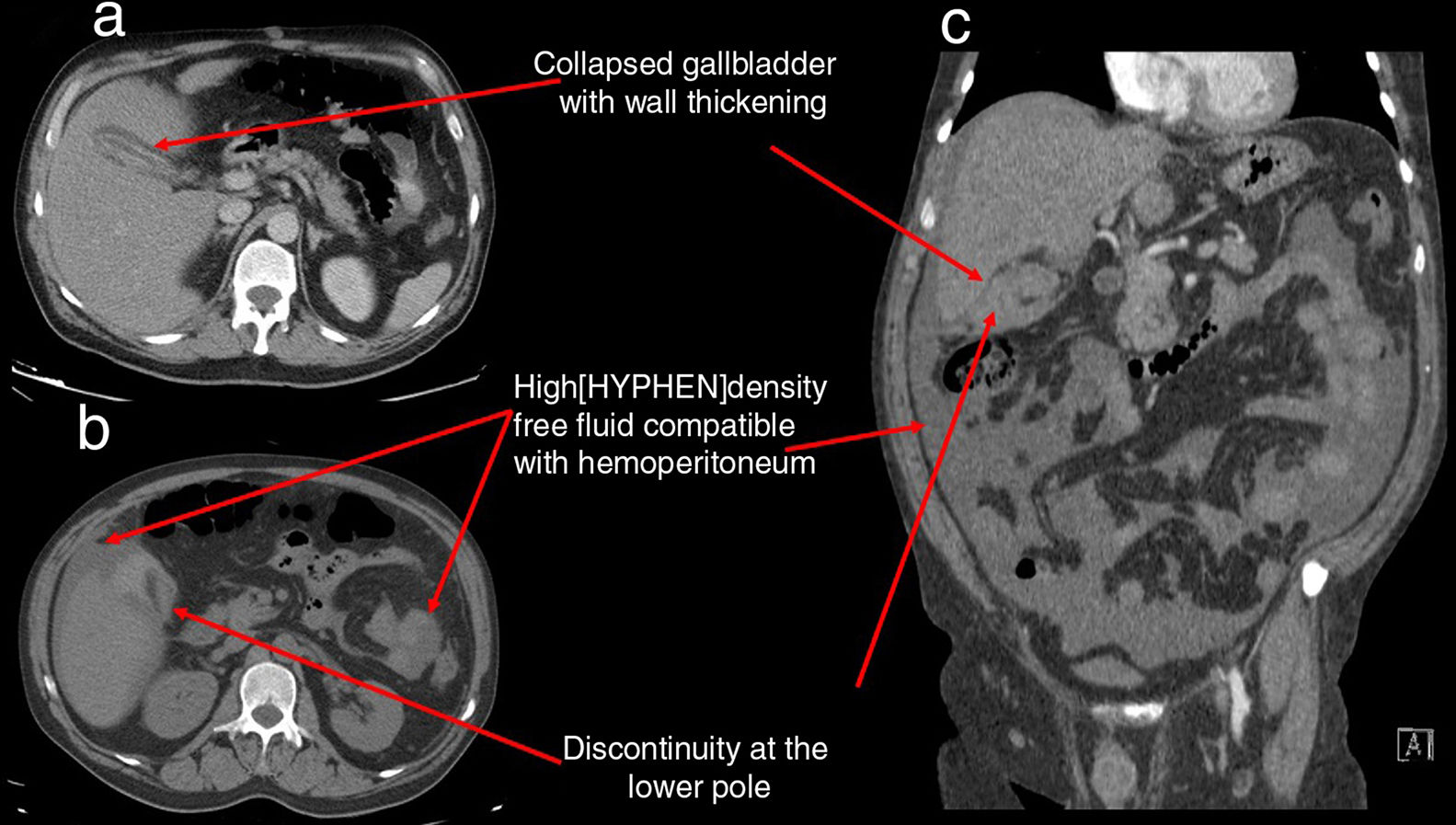
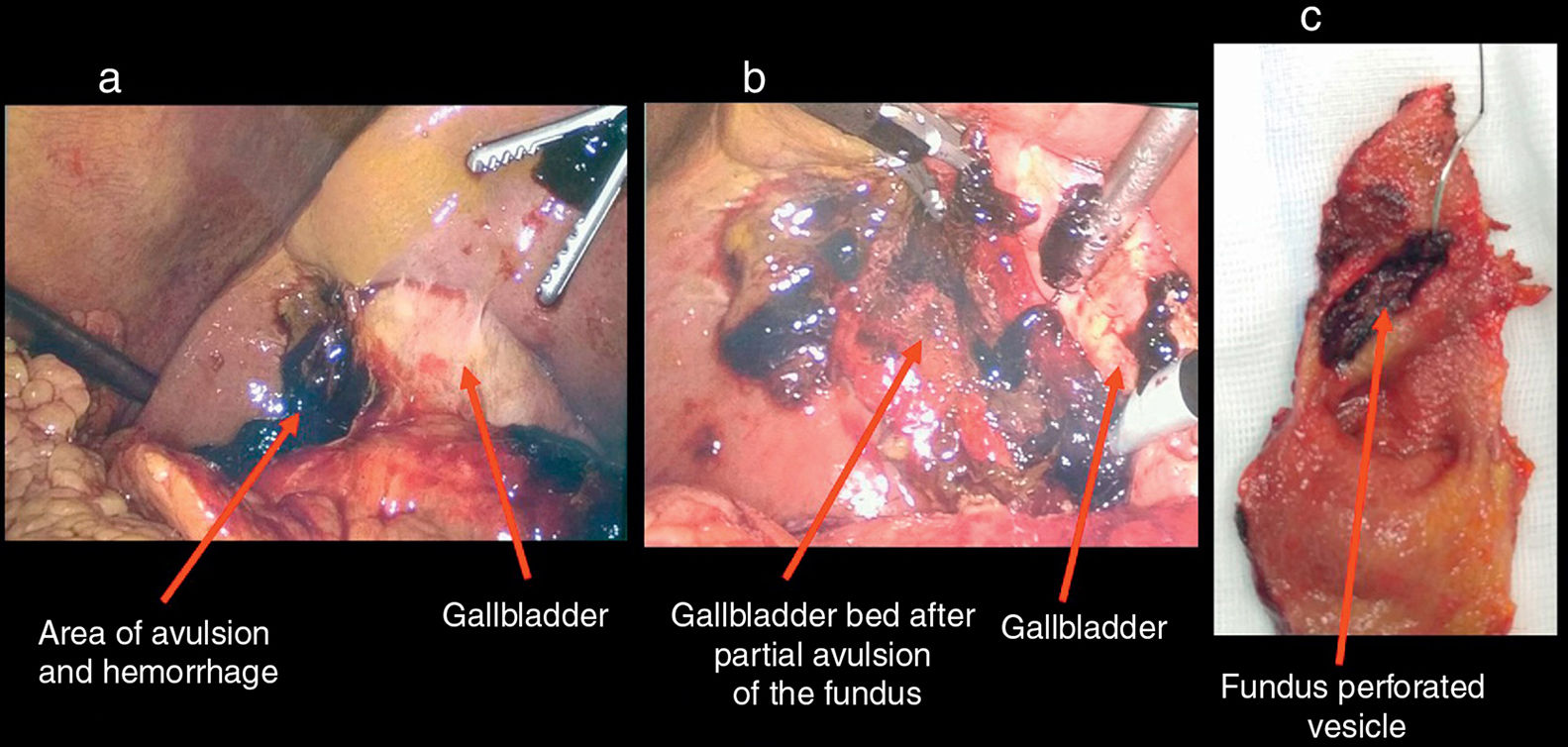
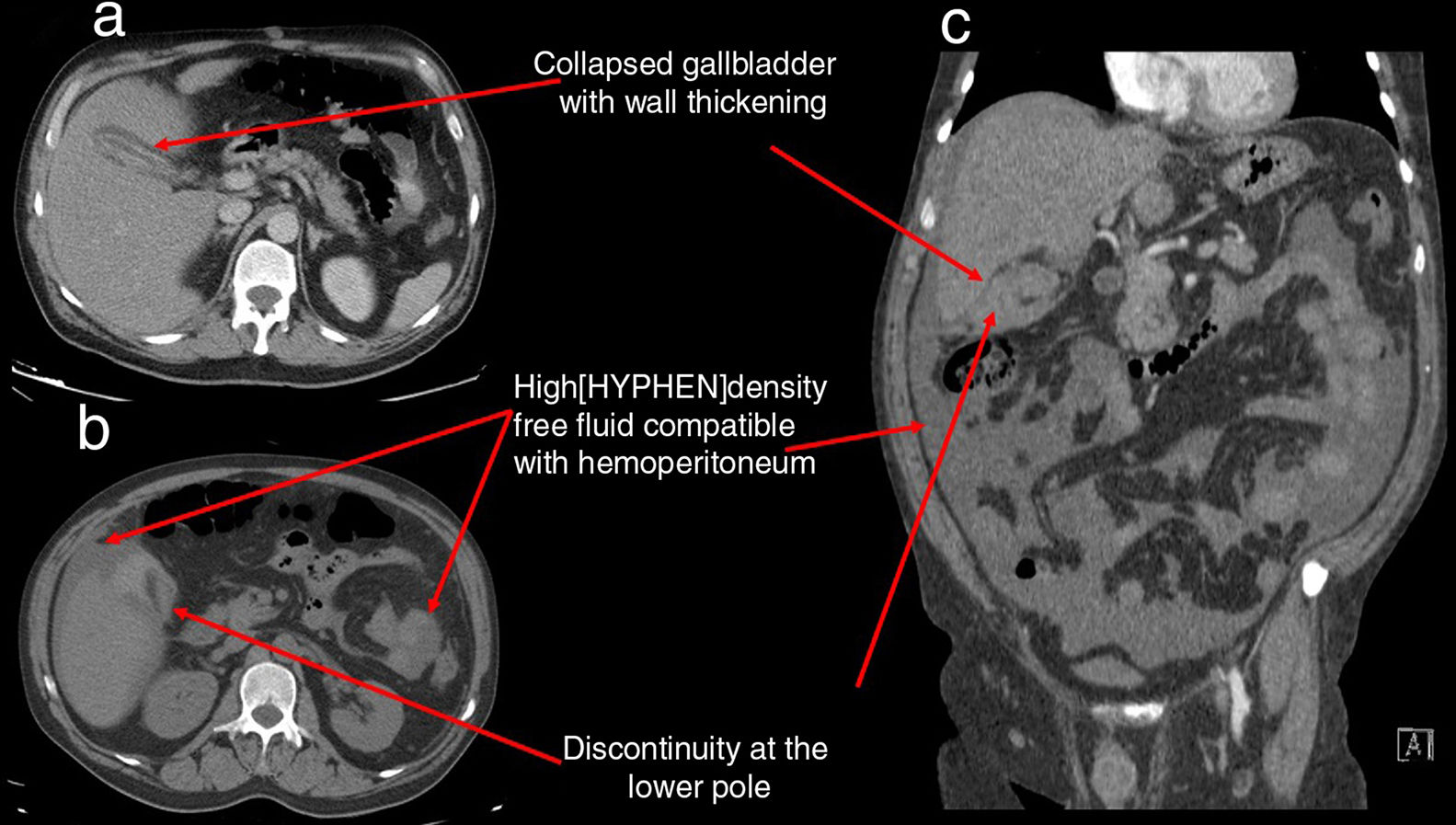
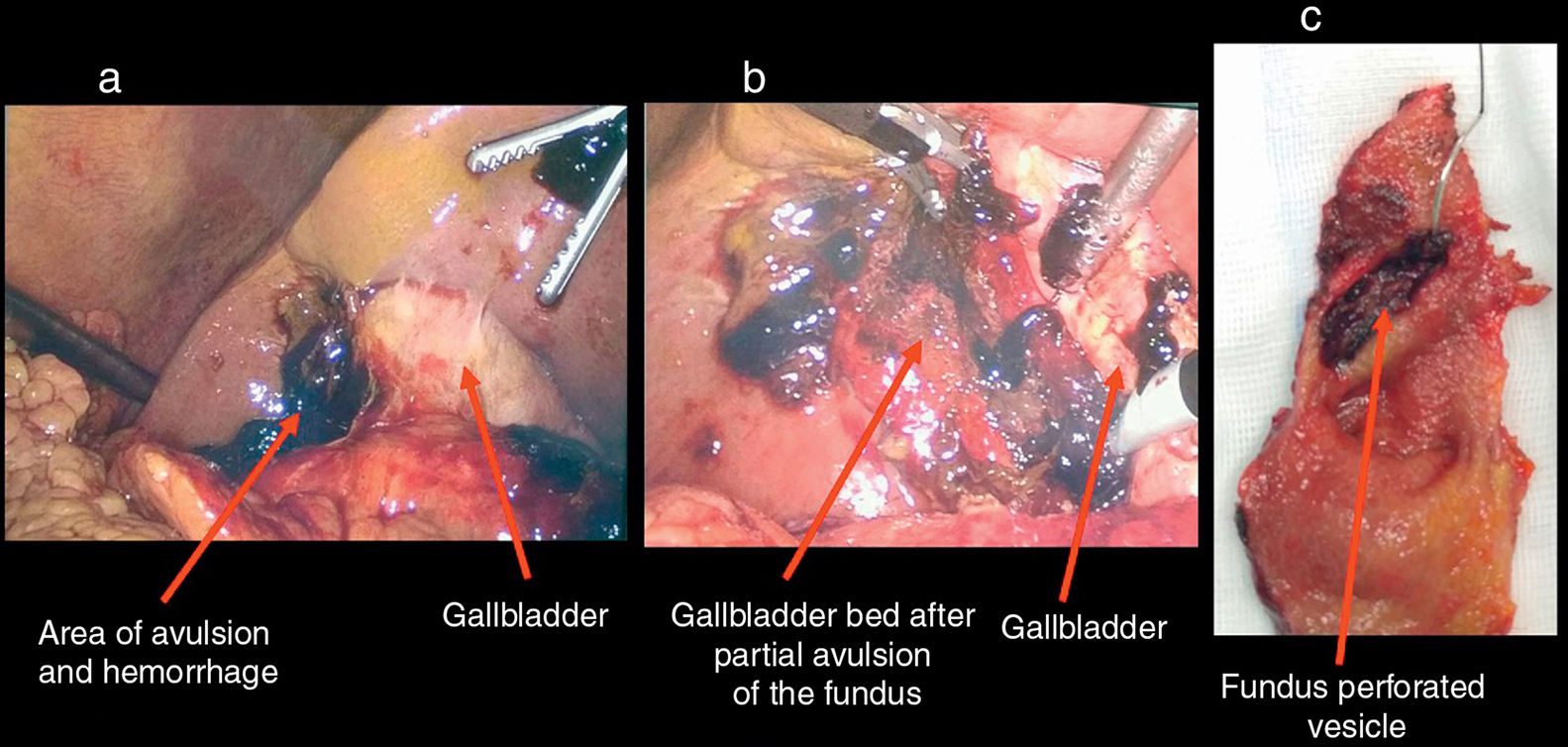
Isolated gallbladder injuries appear in only 2% of abdominal trauma cases and are associated with risk factors such as liver cirrhosis. We present the case of a 53-year-old man with a history of major depressive disorder as well as severe alcohol abuse and dependence, who presented with abdominal pain for 6 days after an accidental fall against a sidewalk while intoxicated. Physical examination demonstrated: blood pressure 152/90 and heart rate 120bpm; palpated abdominal distension, hepatomegaly, guarding and peritoneal irritation. Lab work-up showed: 7.5g/dL of hemoglobin, 528×103/μl platelets, C-reactive protein 6.9mg/dL and prothrombin activity 90%. Liver profile reported: total bilirubin 2.3mg/dL, GPT 91U/L, GOT 38U/L and GGT 416U/L. Tomography showed a collapsed gallbladder with dense peri- and intravesical material and discontinuity in the most caudal region, associated with a moderate amount of intraperitoneal free fluid of intermediate density compatible with hemoperitoneum (Fig. 1). Surgical exploration of the abdomen was conducted laparoscopically, revealing perforation and partial avulsion of the gallbladder fundus, associated with moderate chole-hemoperitoneum (Fig. 2). Laparoscopic cholecystectomy and lavage of the abdominal cavity were carried out, and the patient was discharged without incident 24h later. The pathology study reported non-specific chronic cholecystitis with foci of acute activity and transmural perforation.
Please cite this article as: Ibañez N, González A, Ramirez P, Parrilla P. Hemoperitoneo tras estallido vesicular diferido como consecuencia de traumatismo abdominal. Cir Esp. 2018;96:514.
