


The impact of animal death on surgeons during training in laparoscopic techniques is unknown.
MethodsEmotions and cognitive load were assessed depending on animal survival.
ResultsThose exposed to animal death (n=14) had higher levels of sadness (1.3) and anxiety (2.4), and lower levels of happiness (6.1) on a one-to-ten scale, compared to the 56 that were non-exposed (1.0/2.0/7.5). Mean cognitive load was 68.21±12.865 in the exposed and 64.74±14.632 in the non-exposed (p>0.05).
ConclusionsEmotions and cognitive load among surgeons training in laparoscopic techniques were similar, regardless animal survival after the surgical procedure.
Se desconoce el impacto de la muerte animal en los cirujanos durante el entrenamiento en técnicas laparoscópicas.
MétodosSe evaluaron emociones y carga cognitiva dependiendo de la exposición a la muerte del animal.
ResultadosLos 14 expuestos tuvieron niveles de tristeza (1,3) y ansiedad (2,4) más altos, y de felicidad más bajos (6,1), que los 56 no expuestos (1,0/2,0/7,5). La carga cognitiva fue 68,21±12,865 en los expuestos y 64,74±14,632 en los no expuestos. (p>0,05).
ConclusionesEmociones y carga cognitiva de cirujanos durante el entrenamiento en técnicas laparoscópicas fueron similares independientemente de la supervivencia del animal.
Participants emotions during simulation-based training (SBT) tend to be negative and cognitive load high when the simulated patient dies. It is not known if these effects are comparable to animal death in the simulation lab.1 We are aware only of one case report referring to death in surgical simulation that describes the learner was upset and frustrated, and reluctant to reflect on the case.2 The objective was to assess the emotional and mental workload impact that the unexpected death of an animal in the simulation laboratory has on participants.
Material and methodsThis was an observational cohort study with animal death (or not) as primary variable.
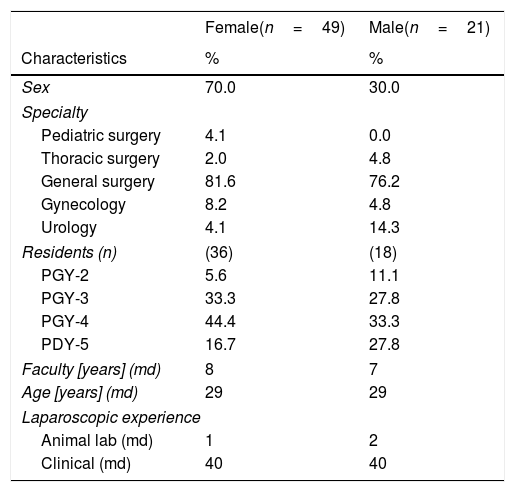
The study population consisted of 70 faculty and surgical residents from different surgical specialties in Spain participating as principal surgeons in minimally invasive surgical training programs for 14 months (Table 1).
Characteristics of the studied population (n=number, PGY=postgraduate year, md=median).
| Female(n=49) | Male(n=21) | |
|---|---|---|
| Characteristics | % | % |
| Sex | 70.0 | 30.0 |
| Specialty | ||
| Pediatric surgery | 4.1 | 0.0 |
| Thoracic surgery | 2.0 | 4.8 |
| General surgery | 81.6 | 76.2 |
| Gynecology | 8.2 | 4.8 |
| Urology | 4.1 | 14.3 |
| Residents (n) | (36) | (18) |
| PGY-2 | 5.6 | 11.1 |
| PGY-3 | 33.3 | 27.8 |
| PGY-4 | 44.4 | 33.3 |
| PDY-5 | 16.7 | 27.8 |
| Faculty [years] (md) | 8 | 7 |
| Age [years] (md) | 29 | 29 |
| Laparoscopic experience | ||
| Animal lab (md) | 1 | 2 |
| Clinical (md) | 40 | 40 |
Surgical procedures were performed in 59 swine under general anesthesia conducted by a veterinarian, including laparoscopic Nissen fundoplication (n=30), laparoscopic gastro-intestinal anastomosis (n=17), laparoscopic radical prostatectomy (n=5), laparoscopic hysterectomy (n=6), and laparoscopic colectomy and gastrectomy (n=12). Two were performed in the same swine on 9 occasions, and 3 on 1 occasion.
Emotional state was assessed using the Scale for Mood Assessment3 and cognitive load using NASA Task Load Index.4
Median and interquartile range were employed for numerical variables and Wilson Score for quantitative variables, while the Mann–Whitney U Test was utilized to compare medians.
The study protocol was approved by the Ethics and Research Committee of Cantabria, Spain (code: 2014.217), and informed consent was obtained from all participants.
ResultsFourteen out of 70 participants (20.0%) experienced death. Eleven deaths happened during anti-reflux surgery. Causes of death included pneumothorax (n=10), hemorrhage (n=1), and dysrhythmias (n=3).
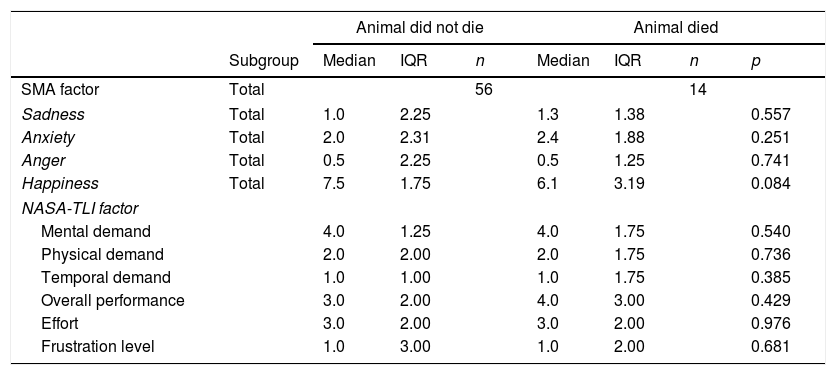
Exposed participants had a higher level of sadness and anxiety, and a lower level of happiness in comparison with the non-exposed ones. Noticeably, happiness levels were high, and anxiety, anger-hostility, and sadness-depression were low in both cohorts. Total cognitive load was slightly higher in the exposed cohort. These differences were not significant (Table 2).
Scale for Mood Assessment (SMA) and NASA Task Load Index scores after finishing the training (NASA-TLI).
| Animal did not die | Animal died | |||||||
|---|---|---|---|---|---|---|---|---|
| Subgroup | Median | IQR | n | Median | IQR | n | p | |
| SMA factor | Total | 56 | 14 | |||||
| Sadness | Total | 1.0 | 2.25 | 1.3 | 1.38 | 0.557 | ||
| Anxiety | Total | 2.0 | 2.31 | 2.4 | 1.88 | 0.251 | ||
| Anger | Total | 0.5 | 2.25 | 0.5 | 1.25 | 0.741 | ||
| Happiness | Total | 7.5 | 1.75 | 6.1 | 3.19 | 0.084 | ||
| NASA-TLI factor | ||||||||
| Mental demand | 4.0 | 1.25 | 4.0 | 1.75 | 0.540 | |||
| Physical demand | 2.0 | 2.00 | 2.0 | 1.75 | 0.736 | |||
| Temporal demand | 1.0 | 1.00 | 1.0 | 1.75 | 0.385 | |||
| Overall performance | 3.0 | 2.00 | 4.0 | 3.00 | 0.429 | |||
| Effort | 3.0 | 2.00 | 3.0 | 2.00 | 0.976 | |||
| Frustration level | 1.0 | 3.00 | 1.0 | 2.00 | 0.681 | |||
IQR: interquartile range. n: number. p-values≤0.05 were considered statistically significant.
Our results showed that animal death during SBT did not seem to make significant differences in cognitive workload and emotional state among surgeons training in complex surgical procedures in the simulation lab. The emotional state of surgeons was positive overall, which correlates with the good acceptance of simulation-based training in healthcare. Eleven out of the 14 deaths occurred during laparoscopic fundoplication indicating its complexity.
These results may have been related to the fact that cause of death could not always be directly attributed to the learner, as several times different procedures were performed on the same swine. Moreover, sometimes animals were in poor physical condition that was not previously detected. And it was a non-survival procedure in any case. The training was for formative assessment and did not involve a high stakes outcome such as grading.
Cognitive load theory proposes that working memory is a key element to manage the complexities of learning surgical skills, as it is responsible for actively processing and manipulating information in the moment. The addition of information that is irrelevant to learning objectives, as the stress of experiencing death, place extraneous cognitive load on trainees that may hinder learning.5
One limitation of this study was the small sample size. Characteristics of the cohorts were somewhat different due to the fact that participants were grouped after the surgical procedures. Ethical and cultural differences might have influenced the learners’ responses. There is a need for further research to elucidate these effects on learning outcomes, along with the impact of the training level, the cause or the time of the animal's death during surgery.
Conflict of interestsThe authors declare no conflict of interest. Hospital virtual Valdecilla (Santander, Spain) is affiliated with the Center for Medical Simulation (Boston, MA, USA), with the mission of improving patient safety by means of expert training and development of healthcare professionals. Both are nonprofit, educational, charitable organizations that offer instructor and clinical training courses with tuition.
FinancingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
We would like to thank Wolters Kluwer Author Services for English language editing.



