




In 2020, our society was struck by the COVID-19 pandemic. Many measures were adopted to prevent the virus from spreading, including lockdowns with permission to leave home only to engage in activities deemed essential. This resulted in a great deal of occupational activity coming to a stop. In Spain, the strictest lockdown period, which lasted from 15 March to 4 May, was followed by a gradual decrease in restrictive measures. Given this situation, society had to adapt to a new reality and with it make lifestyle modifications.
In people with diabetes mellitus type 1 (DM1), a suitable lifestyle is known to play a role in glycaemic control and therefore disease management. In fact, predictive estimates warned of a probable worsening of glycaemic control during this lockdown period.1
The objective of this study was to assess the effects of the lockdown on glycaemic control in people with DM1. To achieve this objective, 100 patients using a FreeStyle® system included on the LibreView® platform of the Department of Endocrinology and Nutrition at Hospital Universitario Central de Asturias [Asturias Central University Hospital] with up-to-date data at the time of sample selection were randomly selected. Data were collected for three 14-day periods: pre-lockdown (Pre: 1 February to 15 March), lockdown (LD: 15 March to 4 May) and post-lockdown (Post: 4 May to 31 May). Thirty-two patients were excluded as in at least one period it was not possible to collect data with sensor use over 70%. The following were recorded for each patient: age, sex and parameters for assessment of glycaemic control recommended by Advanced Technologies & Treatments for Diabetes (ATTD) (time in range [TIR] 70−180 mg/dl, time in hypoglycaemia <70 mg/dl and time in hyperglycaemia >180 mg/dl).2 The SPSS® v.25.0 software programme was used for statistical analysis. Comparisons between the three periods were made using analysis of variance (ANOVA) or Friedman and Wilcoxon tests, depending on whether or not the criteria for a normal distribution were met. Statistical analysis was used to assess differences between the three groups, with p < 0.05 corresponding to statistical significance. Where differences were found, subanalyses were performed to look for between-group differences (with p < 0.017 corresponding to statistical significance). In the subgroup analysis (by sex, age and glucose management indicator [GMI]), only pre-lockdown and lockdown were compared using percentage change and Student’s t test.
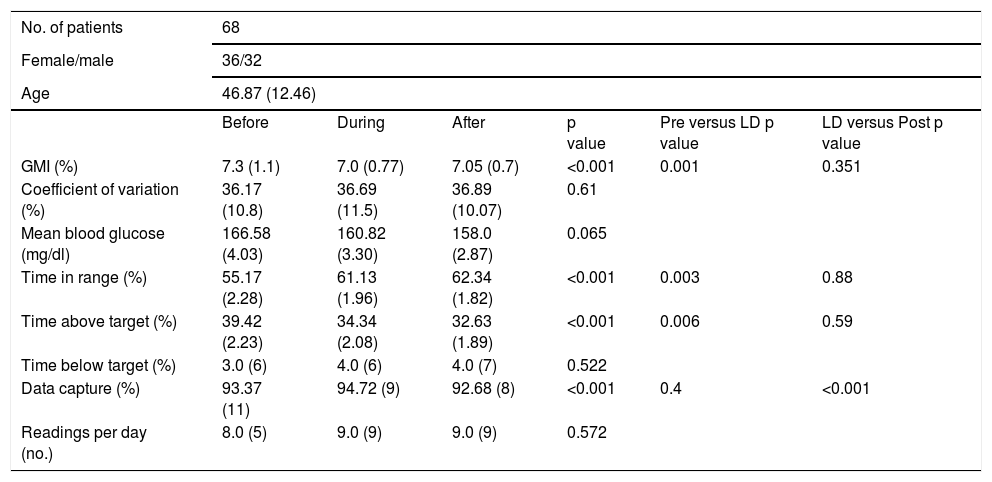
The results obtained, shown in Table 1, reflected significant differences in several parameters of glycaemic control during lockdown compared to pre-lockdown. These differences held, without significant changes, in the comparison to the post-lockdown period. Increased TIR (Pre: 55.17%; LD: 61.13%; Post: 62.34%; p < 0.001), decreased GMI (Pre: 7.3%; LD: 7.00%; Post: 7.05%; p = 0.001) and decreased time in hyperglycaemia (Pre: 39.42%; LD: 34.34%; Post: 32.63%; p < 0.001) were found; no significant changes in hypoglycaemia were detected (Pre: 3%; LD: 4%; Post: 4%; p = 0.522). In 28 patients (41%), the decrease in GMI was >0.4%.
Baseline characteristics and glycaemic control parameters.
| No. of patients | 68 | |||||
|---|---|---|---|---|---|---|
| Female/male | 36/32 | |||||
| Age | 46.87 (12.46) | |||||
| Before | During | After | p value | Pre versus LD p value | LD versus Post p value | |
| GMI (%) | 7.3 (1.1) | 7.0 (0.77) | 7.05 (0.7) | <0.001 | 0.001 | 0.351 |
| Coefficient of variation (%) | 36.17 (10.8) | 36.69 (11.5) | 36.89 (10.07) | 0.61 | ||
| Mean blood glucose (mg/dl) | 166.58 (4.03) | 160.82 (3.30) | 158.0 (2.87) | 0.065 | ||
| Time in range (%) | 55.17 (2.28) | 61.13 (1.96) | 62.34 (1.82) | <0.001 | 0.003 | 0.88 |
| Time above target (%) | 39.42 (2.23) | 34.34 (2.08) | 32.63 (1.89) | <0.001 | 0.006 | 0.59 |
| Time below target (%) | 3.0 (6) | 4.0 (6) | 4.0 (7) | 0.522 | ||
| Data capture (%) | 93.37 (11) | 94.72 (9) | 92.68 (8) | <0.001 | 0.4 | <0.001 |
| Readings per day (no.) | 8.0 (5) | 9.0 (9) | 9.0 (9) | 0.572 | ||
Results for the three periods expressed in terms of mean and standard deviation. Result for the statistical analysis comparing the three periods (significant if p < 0.05). If significant, to its right is a comparison between the pre-lockdown and lockdown periods and between the lockdown and post-lockdown periods (significant if p < 0.017).
The subgroup analysis found no significant differences by sex. By age, a difference was indeed found in modification of time in hyperglycaemia (−10.32% in those <45 years of age versus −2.23% in those >45 years of age; p = 0.032); however, no differences were detected in GMI or TIR. Patients with an initial GMI > 7.5% showed a greater reduction in time in hyperglycaemia (−23% versus +4%; p = 0.005), with no significant differences in TIR or in GMI.
Hence, these results contrasted with the above-mentioned estimates and studies showing worsening of control.1,3 They were, however, consistent with a larger number of studies showing an improvement in glycaemic control both in adults4–6 and children and adolescents,7,8 with a response to lockdown similar to that seen in our sample.
We can conjecture as to the cause of these changes in glycaemic control. Cessation of occupational activity in many patients brought about an increase in free time that might have enabled them to invest in self-care and disease management. Indeed, other studies have shown that patients who did keep their jobs did not experience changes in glycaemic control.4 Increased diabetes care may have also led to increased use of correct doses of insulin, and with it improved glycaemic control. Nutrition is essential in managing DM1, and changes in eating patterns seen in this period with a higher likelihood of having a regular schedule could have been another factor accounting for this improvement.9 Physical activity during lockdown was difficult to assess and varied by patient profile,10 but it predominantly decreased.3,5,9 Ultimately, we understand that improvements in glycaemic control were primarily due to patients finding themselves with more free time and fewer day-to-day tasks. This shift would have enabled them to focus on improving their self-care, and with that, better managing their disease, thus achieving good outcomes despite their reduced healthcare system access. This demonstrates proper knowledge and capacity for action in relation to diabetes mellitus. It could be useful to determine whether this improvement persisted over time beyond the post-lockdown period or instead patients returned to their prior glycaemic control values when their regular activities resumed.
Our study had a suitable sample size and highly reliable data. Its limitations included its lack of assessment of other parameters of interest in DM1 management, such as weight and insulin units. In addition, sample selection itself excluded patients with suboptimal monitoring use (<70% data capture). It could be of interest to assess whether changes in sensor use occurred in relation to lockdown in this other patient profile.
In conclusion, this study showed that lockdown improved glycaemic control parameters in our sample of patients with DM1 using the FreeStyle® system with a data capture rate over 70%.
Main authors of the article.
Please cite this article as: Rodriguez Escobedo R, Alonso Felgueroso C, Martinez Tames G, Sanchez Ragnarsson C, Menendez Torre EL. Consecuencias del confinamiento por la COVID-19 en el perfil glucémico en diabetes mellitus tipo 1. Endocrinol Diabetes Nutr. 2022;69:305–307.

recomendados