




A long-term diabetic complication, fatigue, which is a direct result of treatment and psychological processes, is a common symptom in diabetic individuals.
AimsTo determine the reliability and validity of Functional Assessment of Chronic Illness Treatment-Fatigue Scale in Turkish patients with type 2 diabetes.
Study designA methodological study.
MethodsThe sample consisted of 133 patients with type 2 diabetes who agreed to participate in the study and met the criteria for the study. Data were collected using the descriptive information form prepared by the researcher and the Scale obtained from FACIT System. The research data were collected by face-to-face interviews with the patients. Language and content validity of the Turkish version of the Scale was provided, Cronbach's Alpha coefficient, test–retest analysis and item analysis methods were used as reliability analysis.
ResultsThe total Cronbach Alpha coefficient of the scale was found to be 0.92. According to the results of factor analysis, unlike the original scale, two sub-dimensions emerged in the Turkish version of the scale.
ConclusionsAs a result of the validity and reliability analysis of the FACIT-Fatigue Scale, it can be said that it provides psychometric measures that can be used to determine the level of fatigue of type 2 diabetes patients in Turkish society.
La fatiga, una complicación a largo plazo de la diabetes que es consecuencia directa del tratamiento y de procesos psicológicos, es un síntoma frecuente en los diabéticos.
ObjetivosDeterminar la fiabilidad y la validez de la escala de fatiga de la valoración funcional del tratamiento de enfermedades crónicas (FACIT) en pacientes turcos con diabetes tipo 2.
Diseño del estudioEstudio metodológico.
MétodosLa muestra constaba de 133 pacientes con diabetes tipo 2 que aceptaron participar y cumplían los criterios del estudio. Se recogieron datos mediante el impreso informativo descriptivo preparado por el investigador y la escala obtenida del sistema FACIT. Los datos se recogieron en entrevistas personales con los pacientes. Se informa de la validez del idioma y el contenido de la versión turca de la escala, y se utilizaron el coeficiente alfa de Cronbach, el análisis prueba-reprueba y métodos de análisis de ítems para analizar la fiabilidad.
ResultadosEl coeficiente alfa total de Cronbach de la escala era 0,92. Según los resultados del análisis de factores, a diferencia de la escala original, en la versión turca de la escala surgieron 2 subdimensiones.
ConclusionesBasándose en el resultado de los análisis de validez y fiabilidad de la escala de fatiga de la FACIT, puede afirmarse que proporciona medidas psicométricas que pueden emplearse para determinar el grado de fatiga de los pacientes con diabetes tipo 2 en la sociedad turca.
Fatigue is a general complaint that accompanies many chronic diseases, both physical and mental. Left uncontrolled, it will lead to a decrease in the quality of life for the individual and prevent them from experiencing life satisfaction.1,2 The subjective nature of fatigue leads to a lack of specific assessments and treatments on the matter, which in turn may cause fatigue to be ignored by clinicians.2 Studies have identified fatigue as one of patients’ most problematic aspects in the context of chronic diseases such as Multiple Sclerosis, cancer, RA and diabetes.3–10
Diabetes, one of the most common diseases worldwide, is a complex and chronic disease that requires continuous medical care with multifactorial risk reduction strategies as well as glycemic control. The most common long-term diabetic complication, fatigue, occurring in more than 60% of diabetic individuals, is a direct result of the treatment and psychological processes.11,12 Fatigue disturbs the diabetic patient's concentration, causing emotional fluctuations, increasing complication risk and reducing quality of life.12 Fatigue is also a possible hindrance to health-promoting behaviors such as a healthy eating plan or regular exercise following diabetes self-care participation.13 Fatigue in diabetes is a multidimensional situation that includes physiological, psychological and lifestyle factors. The physiological dimension can be a result of hypoglycemia/hyperglycemia or large fluctuations between the two, whereas the psychological dimension can be associated with depression related to the diagnosis, emotional stress, or the intensity of diabetes self-management regimes. Additional lifestyle factors may include physical inactivity and/or overweight.1
Fatigue in diabetic patients presents a major risk for acute and chronic complications associated with diabetes. Successful self-management includes participation in exercise, hypoglycemia/hyperglycemia management, and the calculation of insulin doses.12 Nurses should stress the importance of symptom assessment in self-management education of diabetic individuals. For this purpose, the symptom of fatigue should be used as a starting point for evaluating comorbid conditions, including diabetic complications and clinical or subclinical psychological disease.13 Assessing the fatigue of diabetic patients and ensuring that they deal with fatigue, contribute to nursing care plans and the quality of care, as well as the quality of individual life.
There is no standardized definition of measurement and diagnostic criteria for fatigue in diabetes.11 Even though diabetes is expressed as a global epidemic in the world, there was no diabetes-specific fatigue assessment scale in the literature. Although assessment of fatigue does not require a multidimensional approach, it is difficult to talk about a common consensus on a standard method of measurement because it is a subjective symptom. Daily use of fatigue scales can help nurses in identifying activities that increase the level of fatigue. This information is useful in developing a plan for the management of fatigue and for establishing rest periods.14
In this context, a specific fatigue measure is needed in assessing fatigue in diabetic patients.
Materials and methodsDesignIn scale validity and reliability studies conducted for another culture adaptation of a scale, it is suggested that the sample size be 5–10 times the number of items in the measure.15–17 It is reported that at least 30 pairs of data are required for test–retest evaluation.18 Since the FACIT-Fatigue (FACIT-F) Scale used in this study was composed of 13 items, it was aimed to reach 130 patients for the first application and at least 30 patients for the test–retest analysis. In the study, the Scale was first administered to 133 patients, and the first 31 patients who were re-visited for the second application and who agreed to repeat the test were re-administered.
Data collection procedureRegular visits were made to the Diabetes Monitoring and Education outpatient clinics by the researchers between February 1 and April 30, 2015 for the data collection. Data were collected face to face with type 2 diabetes patients who met the sample criteria and agreed to participate in the study. Study data were collected at the hours of the outpatient clinic, usually in the morning (09.00–12.00) and after lunch (14.00–17.00). Data collection tools are applied to the patients who have accepted to participate in the research. Written and verbal approvals were obtained by giving information about the purpose of the research. Data were collected using the Questionnaire for Descriptive Characteristics and the FACIT-F Scale. Data collection time was 20min on average for each participant.
The participants’ socio-demographic characteristics (such as age, gender, marital, and education status) and certain other identifying characteristics (including night sleep time, sleep quality, smoking habits and alcohol use, activity and exercise level) were collected by face-to-face interviews with the patients. Clinical features (such as duration of illness (diabetes), treatment forms, presence of other chronic diseases, presence of complications of diabetes, etc.) and laboratory measurements of the patients (most recent HbA1c and fasting blood glucose (FBG) levels) were obtained from patient files registered beforehand.
ParticipantsThis study was a methodological research to determine the reliability and validity of Functional Assessment of Chronic Illness Treatment-Fatigue Scale in Turkish patients with type 2 diabetes. The study sample consists of three hospitals located in Balıkesir province, which were diagnosed with type 2 diabetes and were treated at The Diabetes Monitoring and Training Polyclinics between February 1 and April 30, 2015. The Sample consists of 133 patients who agreed to participate in the study and met the inclusion criteria for the study.
Criteria to be included in the study:
- •
Ability to speak and understand Turkish
- •
Voluntary participation with written approval
- •
Age over 18
- •
Having been diagnosed with type 2 diabetes at least six months prior
- •
Ability to attend diabetes follow-up and outpatient clinic, as well as respond to research questions
For determining the participants’ socio-demographic and diabetes-related health status of a “Patients Characteristics Questionnaire” prepared by the researchers was used. The first part of the questionnaire covers age, gender, marital status, and education. The second part concerns the characteristics of the patient's illness, such as duration of illness (diabetes), treatment forms, most recent HbA1c and fasting blood glucose (FBG) levels. The HbA1c assay has been measured according to the DCCT standard.13
FACIT-fatigue scaleFACIT-F Scale consists of 13 questions evaluating self-reported fatigue and daily activities and functions. The Scale was originally developed to assess fatigue associated with anemia in patients with cancer and has a strong internal consistency (Cronbach's alpha α=0.95), and therefore found to be valid and reliable in assessing fatigue in cancer patients.19 Other than cancer patients in the literature, the FACIT-F Scale was found to be reliable and valid in many chronic diseases, including Parkinson's disease,20 Inflammatory Bowel Disease (IBD),21 Chronic Obstructive Pulmonary Disease (COPD),22 SLE23 and thrombocytopenia.24 In the validity and reliability study of COPD patients, the Cronbach alpha coefficient of the scale was 0.91,22 0.95 in cancer patients,19 0.94 in IBD.21 It has been translated into over 50 languages other than English.
The FACIT-F Scale is composed of 13 expressions that measure the fatigue that the patients had in the last seven days.7 The expressions on the scale consist of Likert type question form which is scored between 0 and 4 and consists of “Not at all”, “A little bit”, “Somewhat”, “Quite a bit”, and “Very much”. The total score range of your scale is 0–52. The higher the scale score, the lower the fatigue level of the patient and vice versa. Items 1, 2, 3, 4, 5, 6, 9, 10, 11, 12, 13 in the scale were reverse scored while items 7 and 8 were scored normally.19–25
The language and content validity of FACIT-F scaleThe English and Turkish versions of the Scale were provided by the website. For the Turkish version of the Scale to be used for the study of validity and reliability on patients with type 2 diabetes, written permission was received. Since the Turkish version of the Scale provided by the website mentioned above was not valid, the studies of the Turkish version of the scale were conducted by using the ‘back translation’26 and the Content Validity Index method (CVI)18 and following the steps below, and then it was compared with the Turkish version from the web site.
Language validity steps- 1.
The English Version of the Scale was translated into Turkish separately by two teaching staff working at the School of Foreign Languages at the University where the researchers were working.
- 2.
These two translations were combined (in Turkish) by another bilingual teaching staff whose native language is English and from the same department.
- 3.
The combined Scale was compared with the original Turkish Scale provided by the website. Both scale items were very close in meaning and grammar.
- 4.
The combined Scale was translated back to Turkish by two different teaching staff.
- 5.
The Scale which was translated back into English and the original English Scale were also compared by the researchers. The scale translated into English was very close to the original. For this reason, the original Turkish version provided by the website was decided to be used in accordance with the opinion of a faculty member from the School of Foreign Languages in the University.
Content validity was accomplished by following these steps:
- 1.
The Scale was examined in terms of eligibility and clarity of translation by a total of five nursing faculty members, three of whom had previous studies of validity and reliability, and two of which had studies regarding chronic diseases and studies in the field of diabetes. Each of the five faculty members were asked to evaluate the appropriateness and clarity of each item of the Scale with scores ranging from 1 to 4 according to the CVI (4: Very suitable, 3: Fairly appropriate but slight changes required, 2: Moderately appropriate, revision of the text is required, 1: Not applicable).
- 2.
According to the opinion of the experts, the CVI value of the Scale was calculated to be 98% and it came to the conclusion that it provides content validity.
- 3.
After the expert opinion, a preliminary application of the Scale was carried out with 18 people. As each item was understood in preliminary application, no changes were made to the Scale afterwards.26 Data from preliminary application were not included in the sampling.
The data obtained in the research were transferred to the SPSS 20.0 (SPSS Inc., Chicago, IL, USA) program in the computer environment and statistical analysis was performed using this program. The number (n) and percentage (%) for categorical variables and the mean±standard deviation value for continuous variables were used in the representation of data.
- a.
Normality analysis: The normality analysis of the FACIT-F Scale was conducted with Kolmogrov–Smirnov and Shapiro–Wilk tests. It has been determined that the distribution of the item point average of the scale does not fit the normal distribution (Kolmogrov–Smirnov=0.10, p=0.002; Shapiro–Wilk=0.96, p=0.001). For this reason, the correlation coefficients were calculated by Spearman's test.
Kuder & Richardson 20, 21 (KR-20,21) and Cronbach Alpha methods are widely used to determine internal consistency in scale validity and reliability studies. If the measurement is a dichotomy, the KR method is used, and if the measurement is a Likert-type measurement, the Cronbach Alpha method is used.18 The FACIT-F Scale used in this study was a Likert-type scale and the Cronbach's Alpha method was used to determine internal consistency.
- b.
Test–retest reliability: Reliability is defined as “the ability to deliver consistent results in every application of a measure”.15 The correlation between the scores obtained from the two applications in order to find the test–retest reliability of the FACIT-F Scale adapted to Turkish was calculated by Spearman's Correlation. The difference between the mean scores obtained from the first and last application of the scale was tested using the Wilcoxon Signed Ranks Test.
- c.
Factor analysis: In order to be able to perform factor analysis on a scale, the correlation of the sample must be large enough to ensure its reliability. The Kaiser-Meyer-Olkin (KMO) test was performed to determine this. A value approaching 1 in the KMO test indicates suitable. The value below 0.5 in the KMO test indicates unsuitable.27
The FACIT-F Scale was tested for its suitability for factor analysis and the KMO value was found to be 0.90 (p<0.05). This result shows that the number of samples in the research is sufficient for factor analysis.27 After the sample consistency was determined, the Explanatory Factor Analysis Method was used for the factor analysis and its steps are as follows:
- •
Obtaining factors: Eigenvalues statistic was applied. Factors greater than 1 were considered significant.
- •
Factor rotation: Varimax rotation technique was used.
- •
Nomenclature of the factors: According to the results obtained, names were given according to the meanings expressed by the materials, taking into consideration the factors that the substances are heavily accumulated.
Statistical significance was accepted as 95% confidence interval and p<0.05.
ResultsCharacteristics of the sampleThe patients included in the study were between the ages of 31–84, the mean age was 56.77±11.46 and 52.6% (n=70) of the participants were female. Most of the patients (94%) were married, 46.6% of them were primary school graduates, and 46.6% was pre-obese according to the obesity classification of the World Health Organization.
Participants were found to have a mean HbA1c level of 8.14±2.29% and HbA1c level of 64.6% (n=86) of participants was found to be 7% and above. It was seen that the FBG average of the patients was 182.88±75.09mg/dL and FBG level of 72.2% (n=96) of participants was 131mg/dL and above. It was seen that 31.6% (n=42) of the patients included in the study had been diagnosed with diabetes for 11 years or longer and 50.4% (n=67) were using oral antidiabetic drugs (OAD) for diabetes treatment. While 56.4% (n=75) of the patients had no other chronic disease except diabetes, 37.6% (n=50) of those with chronic disease had hypertension.
50.4% of the patients were specified as receiving oral antidiabetic drugs (OAD), 38.3% insulin and OAD, and 15% as receiving insulin treatment.
The complications of diabetes were present in the 48.1% (n=64) of the Type 2 diabetes patients included in the study. There observed only one complication of diabetes in 75% (n=48) of patients. Patients with only one complication were found to have 45.8% (n=22) of neuropathy, 41.6% (n=20) of retinopathy, 8.3% (n=4) of nephropathy and 4.1% (n=2) of diabetic foot.
When we analyzed the mean scores of patients (with type 2 diabetes) according to the descriptive characteristics of the FACIT Fatigue Scale, a statistically significant correlation was found between gender and general fatigue score (p<0.005). Female patients were found to have higher levels of fatigue than men.
Internal consistency and correlation between the scale itemsThe Cronbach's Alpha coefficient of the items is a measure of the homogeneity of a scale's internal consistency.28,29 According to Özdamar,30 Cronbach's alpha internal consistency coefficient of a scale; 0.80≤α<1.00 indicates that the reliability of the scale is high. In this study, the Cronbach's alpha value of the FACIT-F Scale was calculated as 0.92, and therefore, the reliability coefficient of the Scale was found to be quite high.
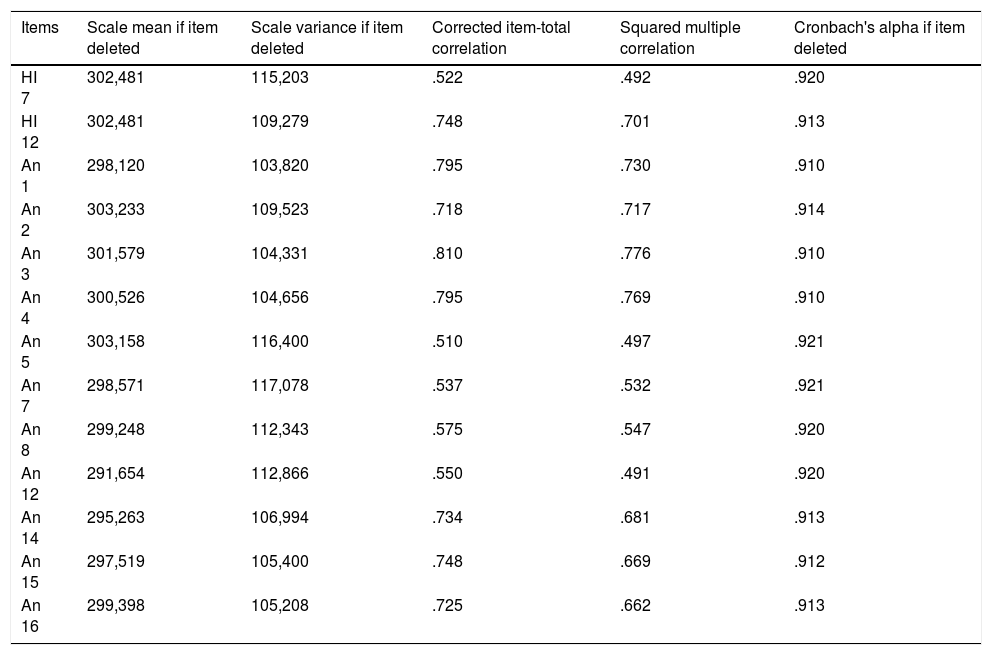
Table 1 shows the distribution of the Cronbach's alpha coefficients of the FACIT-F Scale when the item is deleted. According to Table 1, the reliability of the 13-item Scale was found to be very high with a reliability score of 0.922. When the Cronbach's alpha coefficient was calculated for each item, the values of An1, An3, An4 items were found to be 0.910, and the values of An 5 and An7 were 0.921. All items have an effect on the overall coherence of the scale and there is no item that needs to be removed from the scale (Table 1).
Cronbach alpha coefficients FACIT-F scale when the item deleted (n=133).
| Items | Scale mean if item deleted | Scale variance if item deleted | Corrected item-total correlation | Squared multiple correlation | Cronbach's alpha if item deleted |
|---|---|---|---|---|---|
| HI 7 | 302,481 | 115,203 | .522 | .492 | .920 |
| HI 12 | 302,481 | 109,279 | .748 | .701 | .913 |
| An 1 | 298,120 | 103,820 | .795 | .730 | .910 |
| An 2 | 303,233 | 109,523 | .718 | .717 | .914 |
| An 3 | 301,579 | 104,331 | .810 | .776 | .910 |
| An 4 | 300,526 | 104,656 | .795 | .769 | .910 |
| An 5 | 303,158 | 116,400 | .510 | .497 | .921 |
| An 7 | 298,571 | 117,078 | .537 | .532 | .921 |
| An 8 | 299,248 | 112,343 | .575 | .547 | .920 |
| An 12 | 291,654 | 112,866 | .550 | .491 | .920 |
| An 14 | 295,263 | 106,994 | .734 | .681 | .913 |
| An 15 | 297,519 | 105,400 | .748 | .669 | .912 |
| An 16 | 299,398 | 105,208 | .725 | .662 | .913 |
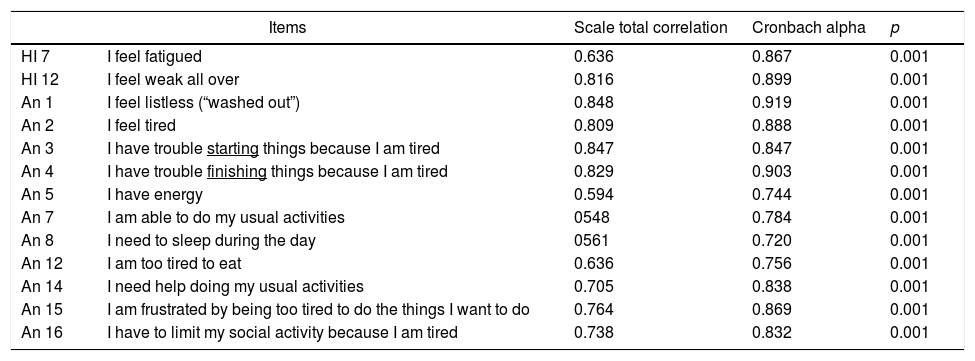
When the total correlations of each item with the Scale are examined, the lowest correlation was of item An 7 with the value of 0.54 and the highest value was 0.84 of item An1. The lowest Cronbach's alpha coefficient was of item An 8 with the value of 0.72 and the highest value was 0.91 of item An 1. The relationship between all items and the scale total score was found to be statistically significant (p<0.05) (Table 2).
Item-scale total score correlations and Cronbach alpha coefficients of Turkish version of FACIT-F scale (n=133).
| Items | Scale total correlation | Cronbach alpha | p | |
|---|---|---|---|---|
| HI 7 | I feel fatigued | 0.636 | 0.867 | 0.001 |
| HI 12 | I feel weak all over | 0.816 | 0.899 | 0.001 |
| An 1 | I feel listless (“washed out”) | 0.848 | 0.919 | 0.001 |
| An 2 | I feel tired | 0.809 | 0.888 | 0.001 |
| An 3 | I have trouble starting things because I am tired | 0.847 | 0.847 | 0.001 |
| An 4 | I have trouble finishing things because I am tired | 0.829 | 0.903 | 0.001 |
| An 5 | I have energy | 0.594 | 0.744 | 0.001 |
| An 7 | I am able to do my usual activities | 0548 | 0.784 | 0.001 |
| An 8 | I need to sleep during the day | 0561 | 0.720 | 0.001 |
| An 12 | I am too tired to eat | 0.636 | 0.756 | 0.001 |
| An 14 | I need help doing my usual activities | 0.705 | 0.838 | 0.001 |
| An 15 | I am frustrated by being too tired to do the things I want to do | 0.764 | 0.869 | 0.001 |
| An 16 | I have to limit my social activity because I am tired | 0.738 | 0.832 | 0.001 |
The test–retest method was used to determine the FACIT-F Scale time invariance. Two weeks after applying the FACIT-F Scale to 133 patients with type 2 diabetes, the FACIT-F Scale was re-applied to the first 31 who accepted to take the test again. When the FACIT-F Scale was first applied to the patients the mean score was calculated as 26.84±10.35 and the mean score of second application was 25.40±9.38. The relationship between the two measurements comparison results was found to be statistically significant (r=0.98; p=0.001). The significance test of the difference between the first and last measurements of the FACIT-F Scale in the same sample (31 patients) was made with the Wilcoxon Signed Ranks test; the difference between two measurements was not statistically significant (z=−0.338, p=0.735).
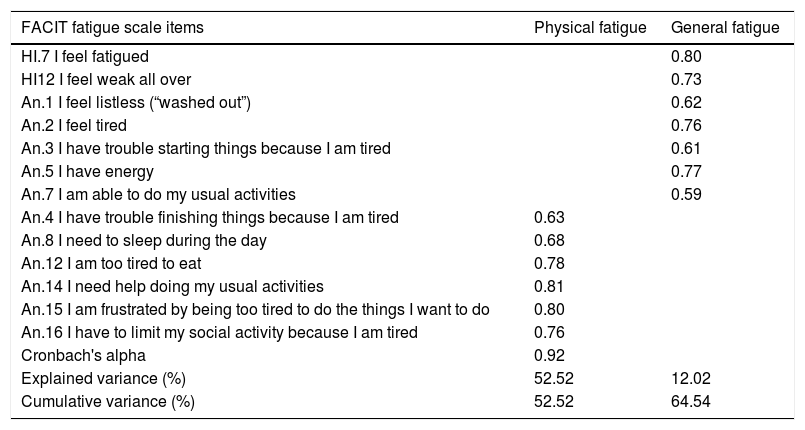
Factor analysisFactor analysis of the FACIT-F Scale was determined by the KMO test, which is suitable for factor analysis and the KMO value is 0.90. While the original Scale consisted of one dimension, two sub-dimensions occurred in the Scale adapted to Turkish. These sub-dimensions were named by the researchers as “general fatigue” and “physical fatigue”. In Type 2 diabetes patients, the lowest factor load according to the factor structure of the FACIT-F Scale was found to be 0.61 of the item An.3 and the highest factor load was 0.81 of the item An14. According to this result, it is seen that ‘physical fatigue’ sub-dimension explains 52.52% of the feature to be measured by this scale and ‘general fatigue’ sub-dimension accounts for 12.02%. Both factors account for 64.54% of the total variance (Table 3).
Factor structure of FACIT-F scale.
| FACIT fatigue scale items | Physical fatigue | General fatigue |
|---|---|---|
| HI.7 I feel fatigued | 0.80 | |
| HI12 I feel weak all over | 0.73 | |
| An.1 I feel listless (“washed out”) | 0.62 | |
| An.2 I feel tired | 0.76 | |
| An.3 I have trouble starting things because I am tired | 0.61 | |
| An.5 I have energy | 0.77 | |
| An.7 I am able to do my usual activities | 0.59 | |
| An.4 I have trouble finishing things because I am tired | 0.63 | |
| An.8 I need to sleep during the day | 0.68 | |
| An.12 I am too tired to eat | 0.78 | |
| An.14 I need help doing my usual activities | 0.81 | |
| An.15 I am frustrated by being too tired to do the things I want to do | 0.80 | |
| An.16 I have to limit my social activity because I am tired | 0.76 | |
| Cronbach's alpha | 0.92 | |
| Explained variance (%) | 52.52 | 12.02 |
| Cumulative variance (%) | 52.52 | 64.54 |
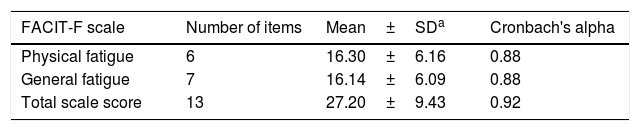
Confirmatory factor analysis to validate the factor structure of the original scale was found to be inappropriate for one sub-dimensional factor structure, and therefore, two sub-dimensional factorial structures were accepted. The reason for the original factor structure of the scale was not accepted may be due to cultural differences. While the general fatigue sub-dimension includes the items of HI.7, HI12, An.1, An.2, An.3, An.5, An.7, physical fatigue sub-dimension has An.4, An.8, An.12, An .14, An.15, An.16. Cronbach's alpha value of physical fatigue and general fatigue sub-dimensions of the scale were 0.88 (Table 4).
Mean, standard deviation and Cronbach alpha values of the sub dimensions of the FACIT-F scale in Turkish type 2 diabetic patients.
| FACIT-F scale | Number of items | Mean±SDa | Cronbach's alpha |
|---|---|---|---|
| Physical fatigue | 6 | 16.30±6.16 | 0.88 |
| General fatigue | 7 | 16.14±6.09 | 0.88 |
| Total scale score | 13 | 27.20±9.43 | 0.92 |
The correlation between sub-dimension scores and Scale total score of type 2 diabetic patients was positive and significant. The correlation for physical fatigue was calculated as r=0.89 and r=0.95 for general fatigue.
DiscussionFatigue is a common symptom that is directly related to the physiological effects, treatment and complications of diabetes. More than 60% of diabetic patients have shown fatigue symptoms.12 For this reason, it is self-evident that the symptom of fatigue is so widely experienced that it must be quantified and objectively measured. There are very few studies in the literature to measure the fatigue levels of people with type 2 diabetes.11–13 In our country, there is no study using the original scale to determine the fatigue levels of type 2 diabetes patients.
The Cronbach's alpha coefficient of the items is a measure of the homogeneity of the scale internal consistency.28,29 The higher the Cronbach's alpha coefficient is, the more reliable the scale is.29,30 According to Özdamar,30 if the Cronbach alpha internal consistency coefficient of scale is .80≤α<1.00, it indicates that the reliability of the scale is high. In this study, the Cronbach's alpha value of the FACIT F Scale was calculated to be 0.92 and the reliability coefficient of the scale was found to be quite high.
In the literature, when the total scores of the scale and the scores of each item are calculated, the average of the item total score correlation coefficients shows the reliability of the test.31 The item total score reliability test is used to determine which items of the scale are appropriate or which items should be changed.15,28 In our study, the relationship between all items and scale total score was statistically significant (p<0.05). The way any of the items affects the general Cronbach's alpha coefficient of the scale is examined. It was observed that the total correlation coefficient (0.92) of the scale was not increased when the item was removed, and therefore, it was not necessary to remove any material from the scale.29,30,32
The Application interval of the test-retest method should be long enough to prevent reminders on the same conditions for the same sample group, but not to allow significant changes in the qualities to be measured.33 In our study, the test–retest method, which we conducted to determine the time-invariant characteristic of the FACIT-F Scale, was applied to 133 patients with type 2 diabetes and re-applied to 31 of them who were contacted two weeks after the first application. In this study, the mean values obtained from the first and second applications were 26.84±10.35 and 25.40±9.38 respectively (p<0.05). The correlation between the two measurements was statistically significant (r=0.98; p=0.001). This shows that the Scale is not influenced by time, and it always measures the same thing even when time passes. According to the results obtained, the test–retest Cronbach's alpha value of the FACIT-F Scale was 0.98 showing that the Scale was very reliable.30
Factor analysis is done in order to assess whether the items in the measure are aggregated under different dimensions.15 There were some structural differences between the results when compared to the original structure of the scale. While the original scale consisted of one dimension, two sub-dimensions occurred in the scale adapted to Turkish. These sub-dimensions are called general fatigue and physical fatigue. Confirmatory factor analysis to validate the factor structure of the original scale was found to be inappropriate for one sub-dimensional factor structure and factor structure with two sub dimensions were accepted. The reasons for the original factor structure of the scale not to be accepted are cultural differences and the fact that it was applied to patients with type 2 diabetes.
LimitationsThe study was conducted with 133 patients with type 2 diabetes in three hospitals located in province center of Balıkesir of Turkey. It has been suggested that the study should be applied to different regions and larger sample groups and that the invariance should be demonstrated in future studies.
ConclusionThis study concludes that FACIT-F Scale provides psychometric measures that can be used to determine the level of fatigue of type 2 diabetic patients in Turkish society as a result of validity and reliability analysis.
The FACIT-F Scale, which is valid and reliable for patients with type 2 diabetes, should determine the fatigue levels of the patients with the disease and develop nursing care and treatment approaches. Optimal metabolic control should be provided by identifying the patient's’ fatigue, placing appropriate targets at the cognitive level and supporting their performance at the highest level. By identifying the fatigue levels of patients with type 2 diabetes many problems can be avoided. In patients with type 2 diabetes, the FACIT-F Scale can be applied to different regions and larger sample groups to investigate invariance. It can be used with qualitative studies to identify other factors affecting the sub-dimensions of the FACIT-F Scale in patients with type 2 diabetes.
Ethical ConsiderationsPrior to commencing work, the University's local ethics committee (Ethics Committee Approval Number: 2015-003) approval and written consent was obtained from the hospitals where the work was conducted.
Informed consentWritten informed consent was obtained from the adolescents who participated in this study and their parents.
Author contributionsConcept – D.Ç., A.Y.; Design – A.Y.; Supervision – D.Ç, A.Y.; Resource – D.Ç, A.Y.; Materials – D.Ç.; Data Collection and/or Processing – D.Ç.; Analysis and/or Interpretation – D.Ç, A.Y.; Literature Search – D.Ç, A.Y.; Writing – D.Ç, A.Y.; Critical Reviews – D.Ç., A.Y.
Financial disclosureThe authors declared that this study has received no financial support.
Conflict of interestNo conflict of interest was declared by the authors.
