


Diabetes knowledge has been shown to improve glycemic control and associate with several demographic parameters. In Greece, a country with high obesity rates, disease knowledge has never been evaluated in diabetic patients. This cross sectional study aimed to assess diabetes knowledge and its associations between social and demographic parameters, among Greek type 2 diabetes mellitus (T2DM) patients.
MethodsOne hundred fifty nine patients with T2DM were recruited from an urban and a rural clinic in Greece. Diabetes knowledge was assessed with the Brief Diabetes Knowledge Test (DKT). Basic anthropometry was performed. Data regarding glycemic control and sociodemographic characteristics were collected from the patients’ medical files.
ResultsGreek T2DM patients demonstrated poor disease knowledge (mean DKT score 8.3±2.2/14.0 and mean DKT as a percent of correct answers 59.6±15.8%). No differences were observed between sex, place of residence, or glycemic control, among subjects. Patients with higher education demonstrated greater diabetes knowledge. Simple obesity with concurrent central obesity or suboptimal glycemic control decreased diabetes knowledge among participants. Additionally, waist circumference was inversely correlated to diabetes knowledge.
ConclusionsBased on the DKT, Greek patients exhibit poor diabetes knowledge. This study provides evidence for the need for better diabetes education in order to ameliorate disease outcome.
Se ha demostrado que el conocimiento de la diabetes mejora el control de la glucemia y se asocia con varias características demográficas. En Grecia, un país con tasas de obesidad elevadas, no se ha evaluado nunca el conocimiento de la diabetes de quienes la sufren. El objetivo de este estudio transversal es valorar el conocimiento de la diabetes y su asociación con parámetros sociales y demográficos en los pacientes griegos con diabetes mellitus tipo 2 (DMT2).
MétodosSe reclutaron a 159 pacientes con diabetes mellitus tipo 2 (DMT2) de una consulta urbana y otra rural de Grecia. El conocimiento de la diabetes se valoró mediante el Brief Diabetes Knowledge Test (DKT). Se recogieron datos antropométricos básicos. Los datos sobre el control de la glucemia y las características sociodemográficas se recogieron de los historiales médicos de los pacientes.
ResultadosLos pacientes griegos con DMT2 mostraron un conocimiento deficiente de la enfermedad (puntuación DKT media de 8,3±2,2/14,0 y DKT media como porcentaje de respuestas correctas 59,6±15,8%). No se observaron diferencias entre los sujetos en función del sexo, del lugar de residencia ni del control de la glucemia. Los pacientes con mayor grado de educación mostraron mayor conocimiento de la diabetes. La obesidad simple con obesidad central o control subóptimo de la glucemia concurrente coincidía con un menor conocimiento de la diabetes por los participantes. Además, había una relación inversa entre el perímetro de la cintura y el conocimiento de la diabetes.
ConclusionesBasándose en el DKT, los pacientes griegos tienen un conocimiento deficiente de la diabetes. Este estudio demuestra la necesidad de una mejor educación sobre la diabetes para mejorar la evolución de la enfermedad.
Type 2 Diabetes mellitus (T2DM) is one of the most common non-communicable diseases, afflicting millions of people worldwide.1 The total burden of the disease is constantly increasing as a result of economic development, urbanization, physical inactivity and obesity.1 During the year 2014, the global estimated prevalence in the adult population reached 9.0%2 and according to projections by the year 2030, diabetes will be the 7th leading cause of all-cause-mortality worldwide.3 T2DM patients are at increased risk for developing complications and comorbidities,4,5 which can only be hampered, once patients participate actively in the management of the disease.6 For self-management to be successful, several skills and competences must be attained by the patient, including a certain level of health literacy, as well as knowledge concerning the disease, decision-making, problem-solving and planning.7–9 Frequent evaluation of diabetes knowledge is required in order to provide more focused and personalized diabetes education and subsequently ameliorate disease outcome.
In Greece, a country with alarming obesity rates,10 the concurrent prevalence of DM in the adult population reaches 8.6%.1Despite the high prevalence of comorbidities and complications recorded among Greek T2DM patients,5 diabetes knowledge has never been evaluated. Thus, the present cross-sectional study was designed, in order to assess diabetes knowledge and its associations between social and demographic values, among T2DM patients in Greece.
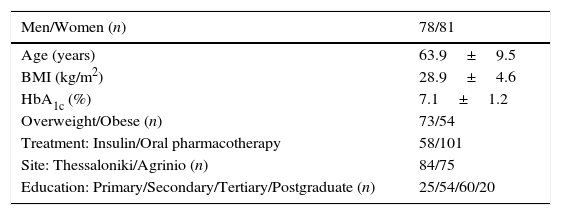
MethodsSample and study designThe sample consisted of 159 adult T2DM patients (78 men), aging between 34 and 88 years old, recruited during 2008 as outpatients from three clinics, two situated in the metropolitan area of Thessaloniki, and one in rural Agrinio (Rural Hospital of Gavalou), Greece. The study's protocol was approved by the Ethical Committee of the Alexander Technological Educational Institute, as well as from each clinic's Director. Participants provided their written consent after being informed of the study's nature. The sample's general characteristics are presented in Table 1.
Patients’ general characteristics (n=159) (Mean±SD or n).
| Men/Women (n) | 78/81 |
|---|---|
| Age (years) | 63.9±9.5 |
| BMI (kg/m2) | 28.9±4.6 |
| HbA1c (%) | 7.1±1.2 |
| Overweight/Obese (n) | 73/54 |
| Treatment: Insulin/Oral pharmacotherapy | 58/101 |
| Site: Thessaloniki/Agrinio (n) | 84/75 |
| Education: Primary/Secondary/Tertiary/Postgraduate (n) | 25/54/60/20 |
BMI, body mass index; SD, standard deviation.
The same, experienced researchers performed basic anthropometry. Weight was measured during morning hours to the nearest 0.1kg (SECA 874, Seca GmbH & Co., Hamburg, Germany) and height to the nearest centimeter with a stadiometer (SECA 214, Seca GmbH & Co., Hamburg, Germany). Waist circumference was measured with a common anelastic tape to the nearest 0.5cm, midway between the inferior margin of the ribs and the superior border of the iliac crest. Body mass index (BMI) was calculated as the weight (kg) divided by the squared height (m). Overweight was defined as 25≤BMI<30kg/m2and obesity as BMI≥30kg/m2, according to the World Health Organization Criteria.11 Central obesity was diagnosed according to the IDF criteria for people of European Origin.12,13
MeasuresGeneral data concerning each patient's age, educational background, and the most recent (within the last 3 months) glycemic control levels via HbA1c concentration were collected from the patients’ medical records. According to the NICE criteria,14 those with HbA1c levels ≤7.0% were considered euglycemic, whereas in patients with HbA1c levels greater than 7.0%, glycemic control was considered suboptimal.
Diabetes knowledgeDiabetes knowledge was evaluated with the Brief Diabetes Knowledge Test (DKT),15 after approval for use was granted from the main author, through personal communication. The DKT consists of a 23-item tool with two subscales. The general knowledge subscale consists of the first 14 questions and can be used on patients with any type of DM. The second subscale consists of the last 9 questions, appropriate only on insulin dependent individuals. In this study, only the first subscale was used, since the majority of patients were treated with oral glucose lowering agents. The DKT has been validated and used in the Greek population in previous pilot studies.16
Data analysesPredictive Analytics Software (PASW) (SPSS, Hong Kong, Hong Kong) was used for data analyses. Since all data were normally distributed, parametric tests were conducted. Comparisons of categorical values between sexes were conducted with chi square tests. ANOVA and independent t-test were used to examine differences between mean values. A p value of 0.05 was considered significant. DKT score was also calculated in quartiles, in order to provide a more graphic presentation of the results.
ResultsMean DKT score was 8.3±2.2 and mean DKT as a percent of correct answers was 59.6±15.8%. No differences were observed regarding recruitment area, place of residence, sex or glycemic control and diabetes knowledge.
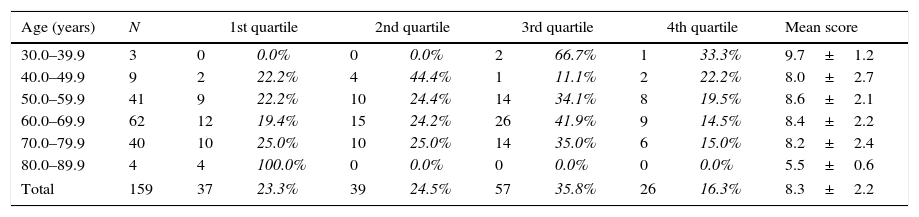
For better DKT results comparison, DKT score was divided in quartiles (Table 2). The majority of participants (35.8%) scored between the 50th and 75th percentile of the DKT, 23.2% scored at the lowest quartile of the test, for 24.5% of the patients their answers ranged between the 25th and the 50th percentile and the remaining 16.3% demonstrated the highest quartile score. All patients belonging to the younger decade of age (30.0–39.9 years) scored above the ≥50th percentile of the test, exhibiting a mean score of 9.7±1.2. All participants aged between 80.0 and 89.9 years old scored at the lowest two quartiles, with a mean test score of 5.5±0.6. The frequency of DKT quartiles was significantly different between patients at the 8th decade of life compared to those at the 3rd (p≤0.03), 5th (p≤0.0013), 6th (p≤0.004) and 7th decade of life (p≤0.024).
Prevalence of DKT score in each quartile, according to the age of participants (n, %, mean±SD).
| Age (years) | N | 1st quartile | 2nd quartile | 3rd quartile | 4th quartile | Mean score | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| 30.0–39.9 | 3 | 0 | 0.0% | 0 | 0.0% | 2 | 66.7% | 1 | 33.3% | 9.7±1.2 |
| 40.0–49.9 | 9 | 2 | 22.2% | 4 | 44.4% | 1 | 11.1% | 2 | 22.2% | 8.0±2.7 |
| 50.0–59.9 | 41 | 9 | 22.2% | 10 | 24.4% | 14 | 34.1% | 8 | 19.5% | 8.6±2.1 |
| 60.0–69.9 | 62 | 12 | 19.4% | 15 | 24.2% | 26 | 41.9% | 9 | 14.5% | 8.4±2.2 |
| 70.0–79.9 | 40 | 10 | 25.0% | 10 | 25.0% | 14 | 35.0% | 6 | 15.0% | 8.2±2.4 |
| 80.0–89.9 | 4 | 4 | 100.0% | 0 | 0.0% | 0 | 0.0% | 0 | 0.0% | 5.5±0.6 |
| Total | 159 | 37 | 23.3% | 39 | 24.5% | 57 | 35.8% | 26 | 16.3% | 8.3±2.2 |
In the total sample, a significant inverse correlation was noticed between DKT% and waist circumference (r=−0.301, p≤0.01). After testing between urban participants only, this association became stronger (r=−0.620, p≤0.014), but among the rural population it was eliminated. Additionally, waist circumference was inversely correlated with DKT among women patients (r=−0.515, p≤0.001). A weaker, yet significant correlation was also noted between DKT and years of education in the total sample (r=0.184, p≤0.05), and in the women (r=0.285, p≤0.01). In men, BMI was negatively correlated with DKT (r=−0.230, p≤0.043). DKT score did not correlate with glycemic control.
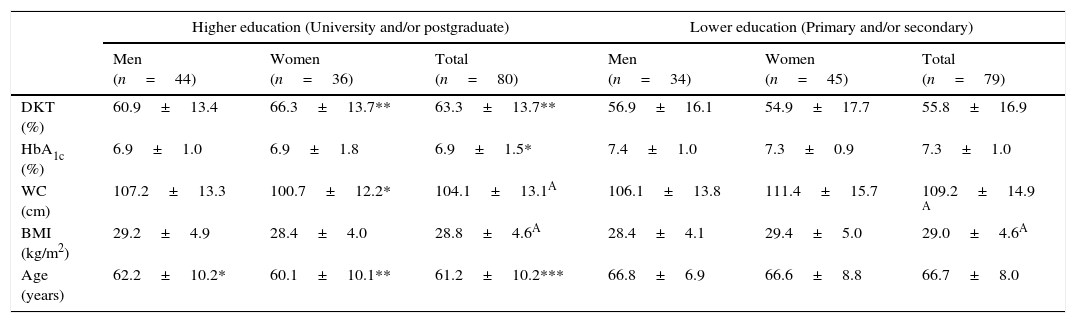
No differences were observed between diabetes knowledge and sex or glycemic control. With respect to the educational background, those with graduate or postgraduate education scored 7.5% more than high school or primary school graduates. Additionally, university graduates exhibited a significantly higher diabetes knowledge score (8.4%) compared to lower education graduates (p≤0.002) (Table 3), as well as lower HbA1c levels (6.9±1.5% vs. 7.3±1.0%, p≤0.032). Women with higher education achieved had better diabetes knowledge and smaller waist circumference compared to the women with primary/secondary education. These associations were not extended in men.
Comparison of DKT and other parameters between patients of higher vs. lower education.
| Higher education (University and/or postgraduate) | Lower education (Primary and/or secondary) | |||||
|---|---|---|---|---|---|---|
| Men (n=44) | Women (n=36) | Total (n=80) | Men (n=34) | Women (n=45) | Total (n=79) | |
| DKT (%) | 60.9±13.4 | 66.3±13.7** | 63.3±13.7** | 56.9±16.1 | 54.9±17.7 | 55.8±16.9 |
| HbA1c (%) | 6.9±1.0 | 6.9±1.8 | 6.9±1.5* | 7.4±1.0 | 7.3±0.9 | 7.3±1.0 |
| WC (cm) | 107.2±13.3 | 100.7±12.2* | 104.1±13.1A | 106.1±13.8 | 111.4±15.7 | 109.2±14.9 A |
| BMI (kg/m2) | 29.2±4.9 | 28.4±4.0 | 28.8±4.6A | 28.4±4.1 | 29.4±5.0 | 29.0±4.6A |
| Age (years) | 62.2±10.2* | 60.1±10.1** | 61.2±10.2*** | 66.8±6.9 | 66.6±8.8 | 66.7±8.0 |
Significantly different compared to the same sex participants of lower education (*p≤0.05,**p≤0.01,***p≤0.001) according to the Independent Samples t-test.
Between BMI tiers, normoweight women exhibited higher DKT score compared to the normoweight men (p≤0.017). Patients with both simple and central obesity scored lower at the DKT compared to the rest of the patients (p≤0.023). Additionally, patients with both simple obesity and suboptimal glycemic control (HbA1c>7%) had significantly lower diabetes knowledge compared to the rest of the participants (p≤0.015).
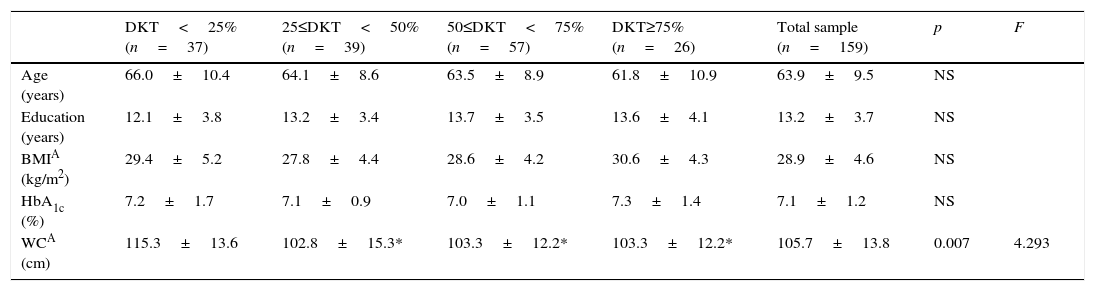
Associations between the quartiles of DKT, age, waist, BMI and HbA1c levels are summarized in Table 4. The one-way multivariate analysis of variances failed to show differences between the means of each quartile for BMI, age, total years of education or the HbA1c levels of participants. A significant difference was observed between the waist circumference of the 1st quartile and all other three (1st vs. 2nd, 1st vs. 3rd, 1st vs. 4th, p≤0.026, p≤0.010 and p≤0.031, respectively for each pair).
Comparison of DKT% quartiles among age, education, BMI, HbA1c levels and WC.
| DKT<25% (n=37) | 25≤DKT<50% (n=39) | 50≤DKT<75% (n=57) | DKT≥75% (n=26) | Total sample (n=159) | p | F | |
|---|---|---|---|---|---|---|---|
| Age (years) | 66.0±10.4 | 64.1±8.6 | 63.5±8.9 | 61.8±10.9 | 63.9±9.5 | NS | |
| Education (years) | 12.1±3.8 | 13.2±3.4 | 13.7±3.5 | 13.6±4.1 | 13.2±3.7 | NS | |
| BMIA (kg/m2) | 29.4±5.2 | 27.8±4.4 | 28.6±4.2 | 30.6±4.3 | 28.9±4.6 | NS | |
| HbA1c (%) | 7.2±1.7 | 7.1±0.9 | 7.0±1.1 | 7.3±1.4 | 7.1±1.2 | NS | |
| WCA (cm) | 115.3±13.6 | 102.8±15.3* | 103.3±12.2* | 103.3±12.2* | 105.7±13.8 | 0.007 | 4.293 |
Statistically different compared to the DKT≤25% group (*p=0.05).
Patients who scored above average on the DKT had 82% greater chances of being euglycemic (PR=1.82, CI:1.12–2.94, p≤0.005), compared to those who scored below the average. Women with optimal glycemic control and women with higher education had greater chances of scoring above average on the DKT (PR=1.47, CI:1.07–2.02, p≤0.013 and PR=1.67, CI:1.24–2.24, p≤0.001, respectively).
DiscussionTo the best of our knowledge, this is the first study investigating diabetes knowledge in T2DM patients, with the use of a validated instrument on a Greek population. In the present study, Greek T2DM patients demonstrated a mean DKT score of 8.3±2.2 and mean DKT as a percent of correct answers equal to 59.6±15.8%. No differences were observed between men and women, place of residence, or glycemic control among subjects. Patients with higher education demonstrated greater diabetes knowledge. Simple obesity with concurrent central obesity or suboptimal glycemic control decreased diabetes knowledge among participants. Additionally, waist circumference was inversely correlated to diabetes knowledge.
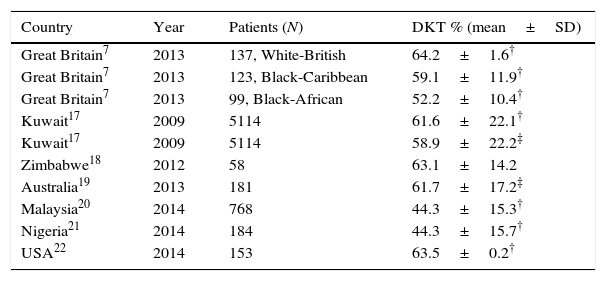
Table 5 presents a summary of published studies assessing diabetes knowledge with DKT. Our patients exhibited limited disease knowledge (DKT score 59.6±15.8%), although similar results have also been reported in studies conducted in Kuwait and Zimbabwe, with the use of the same instrument.17,18 Within Europe, only one study has assessed diabetes knowledge in Caucasian patients of British origin,7 and independent of the population, throughout literature, overall scores appear mediocre.7,19 Moreover, as far as raw results are concerned, a relatively small study of 40 patients conducted by Zheng and associates23 reported a score as low as 10.6±3.6. The etiology behind the limited knowledge exhibited by T2DM patients is unclear. However, this unanimous finding is indicative of the need for the delivery of structured diabetes education, by diabetes health-professionals.
A summary of published studies assessing diabetes knowledge with the DKT.
| Country | Year | Patients (N) | DKT % (mean±SD) |
|---|---|---|---|
| Great Britain7 | 2013 | 137, White-British | 64.2±1.6† |
| Great Britain7 | 2013 | 123, Black-Caribbean | 59.1±11.9† |
| Great Britain7 | 2013 | 99, Black-African | 52.2±10.4† |
| Kuwait17 | 2009 | 5114 | 61.6±22.1† |
| Kuwait17 | 2009 | 5114 | 58.9±22.2‡ |
| Zimbabwe18 | 2012 | 58 | 63.1±14.2 |
| Australia19 | 2013 | 181 | 61.7±17.2‡ |
| Malaysia20 | 2014 | 768 | 44.3±15.3† |
| Nigeria21 | 2014 | 184 | 44.3±15.7† |
| USA22 | 2014 | 153 | 63.5±0.2† |
Unlike other published studies, the present one failed to correlate age with diabetes knowledge. Research suggests that older T2DM patients tend to demonstrate significantly poorer knowledge when compared to younger individuals.24,25 According to Islam,24 every 10 years of increasing age are associated with decreased knowledge. However, multivariable adjustment for each decade or grouping for those aged 65 years or older did not produce any associations in our sample.
In agreement to previous research, no difference was observed between the DKT of men and women patients.17,18,26 There is only one study in literature,24 reporting greater knowledge among men.
Of all the anthropometric indices measured, only waist circumference correlated significantly with DKT. Multivariate analysis revealed that those who scored below 25% on the DKT had greater WC compared to participants with DKT score above 25%. This association is a novel one, since no other study has reported similar findings. According to an Australian study, BMI is correlated to diabetes knowledge,19 however, this association was not produced in the sample herein. Few interventional studies have noted that an increment in diabetes knowledge is followed by a reduction in both BMI and waist circumference,27,28 or in waist circumference alone.29–31 The aforementioned results could be proposing an inverse association between diabetes knowledge and waist circumference, and strengthen our original result.
Our findings suggest that educational background has an impact on both diabetes knowledge and glycemic control. DKT% score demonstrated a weak correlation to the total years of education, in agreement with a recent study on Malaysian patients.20 Post hoc multivariate analysis of DKT% score by educational level pointed out that those who where university graduates scored significantly better on the DKT than those who were only high school graduates, a result consistent with literature.7,19,24 Having higher education increased the chances of scoring above average on the DKT score by 38% (PR=1.38, CI:1.11–1.73, p≤0.01). When tested for sex, only women with higher education exhibited better diabetes knowledge. Overall it was expected that educational level would correlate with disease knowledge, as better education attainment is indicative of better understanding of the disease, its pathophysiology and management.26
Mean HbA1c level of the sample was 7.1±1.2%, slightly above the optimal 7.0% cutoff suggested by the NICE.14 According to Fenwick,19 elevated HbA1c is associated with worse DKT score. Furthermore, interventional studies have proved that improvement in diabetes knowledge has a positive impact on glycemic control.29–31 In contrary to these results, the present study failed to correlate glycemic control to diabetes knowledge. Likewise, DKT% score did not differ significantly between those with and without optimal glycemic control. A possible explanation for this could be the overall low mean HbA1c levels recorded in the present study. It is highly possible, that studies with greater HbA1c variation or mean HbA1c levels would produce better associations with diabetes knowledge, however for the majority of the patients herein glycemic control was close to the optimal target. Indicative of this scenario is the fact that a significant association was noted between the optimal glycemic control group and scoring above average on the DKT.
As far as weight status is concerned, normoweight women demonstrated better diabetes knowledge compared to the normoweight men. Additionally, obese patients, regardless sex, with either concurrent central obesity or suboptimal glycemic control demonstrated lower disease knowledge. Obesity and central obesity are both independent risk factors contributing to the prevalence of T2DM.32 This finding indicates that the clustering of risk factors associated with T2DM is associated with lower disease knowledge. It is possible that the clustering of diabetes risk factors might prevail among patients with poor compliance; however, adherence to the therapy was not assessed in the present study.
Unfortunately, information on demographics known to be associated with diabetes knowledge, like the duration of diabetes, were not used in our study, mainly due to incomplete medical files and failure from the patients’ part to remember the exact onset of the disease. We also speculate that using additional validated instruments assessing diabetes knowledge would provide more trustworthy results. However, due to the lack of similar research on the Greek population, the results on diabetes knowledge among T2DM patients are interesting and useful both for patient education and disease management.
ConclusionsGreek T2DM patients exhibit poor diabetes knowledge, based on the DKT. This study provides evidence for the need of screening patients for disease knowledge, as well as the need for better patient education.
FundingNo funding was received for conducting this study.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors wish to express their sincere gratitude to both clinic Directors for approving this study, as well as to all participating patients, for their collaboration.
