


During the past decades, an increasing incidence of thyroid cancer (TC) has been reported worldwide. In Argentina there is no national cancer registry, and its incidence has therefore not been established. The aim of our study was to determine the incidence of TC in the province of Neuquén and to compare it to that reported in the literature. The medical records of 229 patients admitted over a period of 12 years (2001–2012) were used for data analysis.
Tumor size, age, sex, and histological type were evaluated. The study period was divided into four three-year periods, and differences in each of these features were analyzed. We found an incidence of 4.72/100,000 inhabitants/year, and almost all patients had papillary TC. TC was five times more common in females as compared to males (7.78 and 1.55 respectively). Mean tumor size was 22.2±1.1mm. Tumor size was significantly greater in men (31.8±3.7mm) than in women (20.4±1.0mm). When grouped by three-year periods, a higher number of cases were found in the last one (47, 49, 49 and 84 respectively). As regards tumor distribution by size, there was a significant decrease in mean tumor size in the fourth period and an increase in the proportion of tumors <10mm.
We report an increase in TC incidence in the Argentinean province of Neuquén which is similar to the overall increase reported in the international literature.
En los últimos años se ha demostrado un aumento en la incidencia de cáncer de tiroides (CT). En nuestro país no existe un registro nacional de cáncer por lo que la incidencia del mismo no ha sido establecida. Con el objetivo de conocer su incidencia en la provincia del Neuquén y compararla con la reportada en la literatura revisamos los informes histopatológicos con diagnóstico de CT en el periodo 2001-2012.
Se evaluó tamaño tumoral, edad, sexo y tipo histológico. Se dividió el periodo en 4 trienios y se analizó la diferencia de estas características en cada uno de los mismos. Encontramos una incidencia de 4,72/100.000 hab/año, a expensas casi exclusivamente de carcinoma papilar, y 5 veces mayor en mujeres que en hombres (7,78 y 1,55 respectivamente). Al analizar trienios, se observó un aumento en el número de casos en el último de ellos (47, 49, 49 y 84 respectivamente). La media de tamaño tumoral fue de 22,2±1,1mm. El tamaño tumoral en hombres (31,8±3,7mm) fue significativamente mayor que en mujeres (20,4±1,0mm). En cuanto a la distribución de los tumores por tamaño, hay una disminución significativa en la media del tamaño tumoral en el 4.° trienio y un aumento en la proporción de tumores <10mm.
La incidencia de CT en la provincia argentina de Neuquén es similar a la reportada en la literatura observando un aumento de casos incidentes.
Thyroid cancer (TC) is the most common endocrine malignancy, accounting for 1% of all cancers. Differentiated thyroid carcinoma, including papillary and follicular carcinomas, accounts for 80–90% of all thyroid cancers.1
TC is one of the few cancers with an increased incidence, as documented in various studies in Canada, the United States, and Europe.2–7 By contrast, its mortality has decreased slowly.7,20
In the United States, annual incidence has increased 2.4 times, from 3.6/100,000 population in 1973 to 8.7/100,000 in 2002, and this trend is apparently continuous.2 Such increase, attributed to papillary thyroid carcinoma, has similarly affected men and women, and the female-male ratio has therefore changed little in recent years (3:1). A high proportion of such cancers are tumors 1cm in size or smaller.8,10
In Argentina there are virtually no statistics. Only two studies conducted by Niepomniszcze et al.9 in 1986 and by Faure et al.10 in 2012 on members of the mutual society of the Argentinean federal police report a sample that may be considered representative.
It is thus important to have data from other regions in Argentina. For this purpose, it was decided to retrospectively evaluate all histological reports with a diagnosis of TC in the province of Neuquén during the 2001–2012 period. The primary study objectives were to provide data about TC incidence, to assess if incidence is similar to reported in the literature, and to verify if a progressive increase had occurred in the number of cases. TC distribution by sex, age, histological type and size was also assessed.
Patients and methodsHistological reports issued by all pathology departments of all public and private centers in the province of Neuquén (5 in the city of Neuquén and one in Cutral Co) during the 2001–2012 period were reviewed. Diagnoses of TC in total and partial thyroidectomies in the adult population (15 years or older) in the province of Neuquén (having a population of 404,649 according to the 2010 census) were selected, and projection calculations were made to estimate the population at risk during the period evaluated in this study. Reports of TC in non-thyroid tissue, isolated nodal metastases, and other organs were disregarded in order to avoid overestimation of the incidence. The pediatric population was excluded because pediatric cases are referred to hospitals in Buenos Aires.
The annual incidence rate (IR) of TC per 100,000 population was calculated using the formula: I/PT×years, where I=number of new cases of TC diagnosed in the 12 years, and PT=population over 15 years of age at risk of experiencing TC each year. Results were adjusted for the age-standardized rate.11
Sex, age, histological type, and tumor size were analyzed in the cases detected. A retrospective study by three-year periods (1/1/2001–31/12/2003; 1/1/2004–31/12/2006; 1/1/2007–31/12/2009, and 1/1/2010–31/12/2012) was conducted to assess whether a progressive increase had occurred in the number of cases of TC in the population at risk.
All values are given as mean±SEM. Differences between the groups were analyzed using a one-factor ANOVA test and a Tukey test. INSTAT Version 4.0 software (GraphPadSoftware, San Diego, California, USA) was used, and a value of p<0.05 was considered statistically significant.
The study was evaluated and approved by the Advisory Committee in Biomedical Research in Humans (CAIBSH) ascribed to the Subsecretariat of Health of the province of Neuquén, in accordance to provision No. 1302, dossier No. 442-55950/10, and the Register of Health Researchers (RIS) No. 07.00.10.
ResultsTC was diagnosed in 229 patients, 192 women (83.8%) and 37 men (16.2%). The data correspond to all patients seen in the province of Neuquén. Frequency by histological type was: papillary thyroid carcinoma, 208 (90.8%); follicular TC, 8 (3.5%); medullary TC, 7 (3.1%); mixed TC, 3 (1.3%); and anaplastic TC, 4 (1.3%).
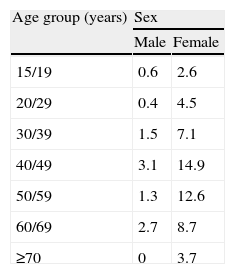
Mean age was 43 years, with a greater incidence between 40 and 49 years of age in both sexes. An incidence of 4.72/100,000 inhabitants/year was estimated, 3.31 after adjustment for age-standardized rate. Incidence was 7.78/100,000/year in women and 1.55/100,000/year in men, with a female/male ratio of 5.2:1 (192:37 cases). Table 1 shows the incidence by sex and age group.
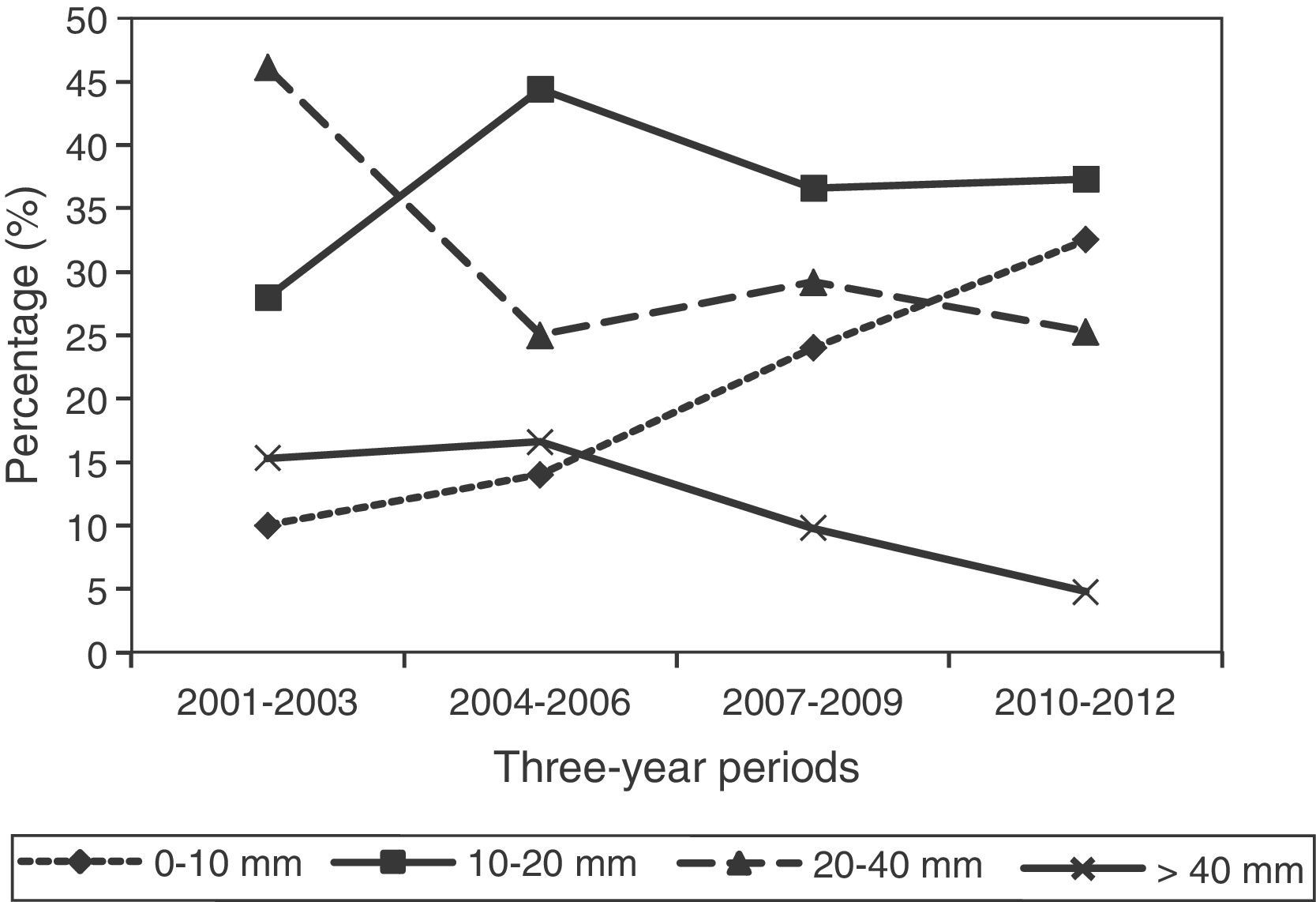
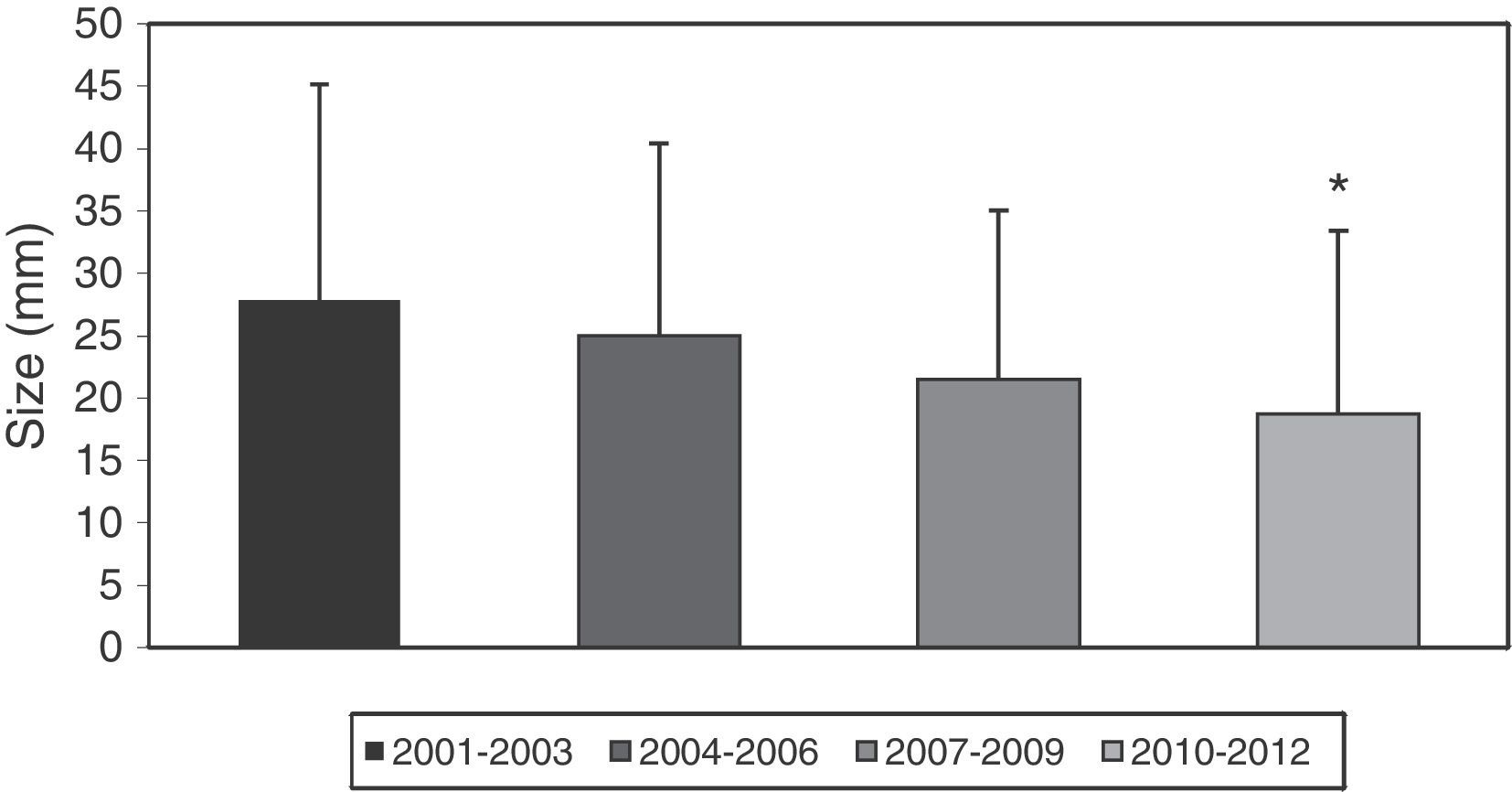
When the number of cases was divided into three-year periods, there were 47, 49, 49, and 5 cases in the first, second, and third periods respectively, with incidence rates of 3.87, 4.03, 4.03, and 6.91 for those periods. Tumor size data were found for 211 of the 229 cases (92.1%). Mean size was 22.2±1.1mm, with tumor sizes ≤10mm in 49 cases (23.2%), of 10–20mm in 77 cases (36.5%), of 20–40mm in 64 cases (30.3%), and >40mm in 21 cases (10%). Tumor size was significantly greater in men as compared to women (31.8±3.7mm vs 20.4±1.0mm, p<0.0001). Fig. 1 shows the percentage corresponding to each tumor size by three-year period. A trend to an increase in tumors ≤10mm and to a decrease in those >40mm is seen. Fig. 2 shows the decrease in size by three-year period (2001–2003: 27.88±17.3mm; 2004–2006: 25.03±15.4mm; 2007–2009: 21.51±13.5mm, and 2010–2012: 18.69±14.7mm), which is significant when mean tumor sizes of the first and last three-years periods are compared (p<0.05). On the other hand, after the decrease in the number of greater tumors (>20mm) in the second and third three-year periods, values of the first period were again found in the third.
Discussion
. *p<0.05 vs 2001–2003.")
TC is the most common endocrine tumor, and its incidence has constantly increased in different parts of the world.12 The reasons for such increase are controversial. Some authors suggest that it is due to increased medical controls and use of ultrasonography. However, other factors such as lifestyle changes, radiation exposure, increased obesity in the population, lower iodine intake, heredity, and other environmental factors cannot be ruled out.13–16
Incidence of TC in the province of Neuquén (4.72/100,000 population) is similar, on average, to that reported in the literature,2–7 but lower than reported by Faure et al.10 (7.28/100,000 population) in the only study estimating the incidence of TC in Argentinean cities (the federal capital and Great Buenos Aires). The reason for this could be that this study was conducted on members of the mutual society of the Argentinean federal police, an ideal population because of their access to care and greater medical monitoring. A progressive increase in incident cases was noted during the study period. This increase was almost 80% in the last three-year period as compared to the first, with an incidence rate of 6.92/100,000 population, close to the rate reported by Faure et al. Such increase appears to be due to advances in diagnostic methods and to a greater social medical coverage. The province of Neuquén is located in the Argentinean Patagonia and borders to the west on Chile, from which it is separated by the Andean mountains, including a number of volcanoes, some of them active. In this regard, a greater incidence of TC has been seen in volcanic areas.17 On the other hand, crops in the province are treated with pesticides, and exposure to these may increase incidence of thyroid disease.18,19
A control performed by the Program of the Argentinean Endemic Goiter Committee in two important towns of the province (Junín de los Andes and Chiuquillihuin) found no endemic goiter. Urinary iodine levels were adequate.20 In addition, studies in the towns of Allen and Cipolletti, in the province of Río Negro, bordering on Neuquén, found the same results, suggesting an adequate iodine intake in these provinces.21 It should be reminded that iodination of salt for human use is mandatory in Argentina.
Most cases of TC are of the papillary variant. As regards follicular carcinoma, 50% of the cases were diagnosed in the first three-year period. This agrees with the results reported by Faure et al., and may be due to introduction of iodine prophylaxis, which altered the proportion of papillary and follicular carcinomas.22,23 As to tumor size, a significant decrease in mean size and an increase in the proportion of tumors <10mm were seen in the last three-year period. This may be due to early diagnosis due to widespread use of ultrasonography and FNA, although environmental factors cannot be ruled out. However, the number of tumors of greater size did not decrease in the last three-year period as compared to the first. On the other hand, Pazaitou-Panayiotou et al.24 noted that the increased incidence in the 1971–2010 period was not only due to microcarcinomas. Faure et al.10 did not find a marked increase in smaller tumor in the period of their study (2003–2011), but reported an increase as compared to the years prior to 2000.
While the greater incidence in women, probably associated to hormone factors, is well known, we found a lower incidence in men than reported in most studies. Tumor size was significantly greater in men as compared to women. We think that the reason for this is that men seek medical help less frequently and later.
In conclusion, TC incidence in the province of Neuquén was similar to that reported in the literature, and an increase was seen in incident cases.
Conflicts of interestThe authors state that they have no conflicts of interest.
Please cite this article as: Cohen Sabban MA, Palmero C, Bertrand B, Aiello A, Ghiglioni A, Mac Donell MC, et al. Incidencia de cáncer de tiroides en la provincia de Neuquén (2001–2012). Endocrinol Nutr. 2014;61:455-459.
