




Ignatzschineria is a recently-described bacterium that on rare occasions has been associated with infection in humans. We report the first case of sepsis due to Ignatzschineria indica in Spain.
The patient was an impoverished 44-year-old male with a history of chronic alcoholism who was seen at the emergency department of our hospital with intense leg pain and a fever of 38.6°C. On examination, he had superficial ulcers on the anterior tibial region of the right leg, macerated skin with areas of necrosis, and cellulitis with a loss of continuity in the interdigital sulcus between the third and fourth toe of the left foot, where the presence of larvae was observed. Laboratory tests revealed leukocytosis of 16,400×109/l and CRP of 65mg/l. Radiography and Doppler ultrasonography of the lower right leg ruled out osteomyelitis and vein thrombosis. Following the collection of blood and exudate cultures, he was admitted under treatment with intravenous amoxicillin/clavulanic acid and corticosteroids due to significant associated oedema.
On the third day, the growth of gram-negative bacilli was observed in an aerobic blood culture bottle. After 24h, oxidase- and catalase-positive colonies grew in blood agar. The VITEK® 2 GN ID card (bioMérieux) identified Acinetobacter lwoffii/Moraxella spp. In light of doubts between the phenotype characteristics and the result obtained, the strain was sent to the reference hospital for confirmation by means of mass spectrometry, Bruker Microflex® LT MALDI-TOF MS (Bruker Daltonics), with Bruker Biotyper® 3.1 software (Bruker Daltonics) and the Biotyper library database, v 6.0 (6903 entries), which identified Ignatzschineria indica. This was confirmed by 16s rRNA sequencing with an ABI PRISM® 3130xl Genetic Analyzer (Applied Biosystems), using the leBIBIQBPP and GenBank (NCBI) databases. In the exudate from the cutaneous lesions, Alcaligenes faecalis and Proteus hauseri were isolated, also confirmed by MALDI-TOF. Ignatzschineria indica was not detected in the exudate cultures. Sensitivity was analysed with the AST-N243 card. The isolate was sensitive to ampicillin (≤2μg/ml), amoxicillin/clavulanic acid (≤2μg/ml), cefotaxime (≤1μg/ml), ciprofloxacin (≤0.25μg/ml), gentamicin (≤1μg/ml), imipenem (≤0.25μg/ml), trimethoprim/sulfamethoxazole (1/19μg/ml). Treatment with amoxicillin/clavulanic acid was maintained for 10 days, with a positive evolution.
The Ignatzschineria genus belongs to the gammaproteobacteria group. It was first reported in 2001 by Tóth et al.6,7 as Schineria, in honour of the entomologist Ignatz Rudolph Schiner (1813–1873), who described the Wohlfahrtia magnifica fly in 1862. In 2007, it was renamed Ignatzschineria. There are three known species: I. indica, I. larvae and I. ureiclastica. All three have been isolated from the Wohlfahrtia magnifica fly and are associated with myiasis or fly larva parasitisation in animals and, exceptionally, humans. These microorganisms are gram-negative aerobic, non-glucose-fermenting, non-spore-forming, non-haemolytic bacilli which are oxidase-, urease- and catalase-positive. They have been isolated in the anterior portion of the larva's digestive tract.
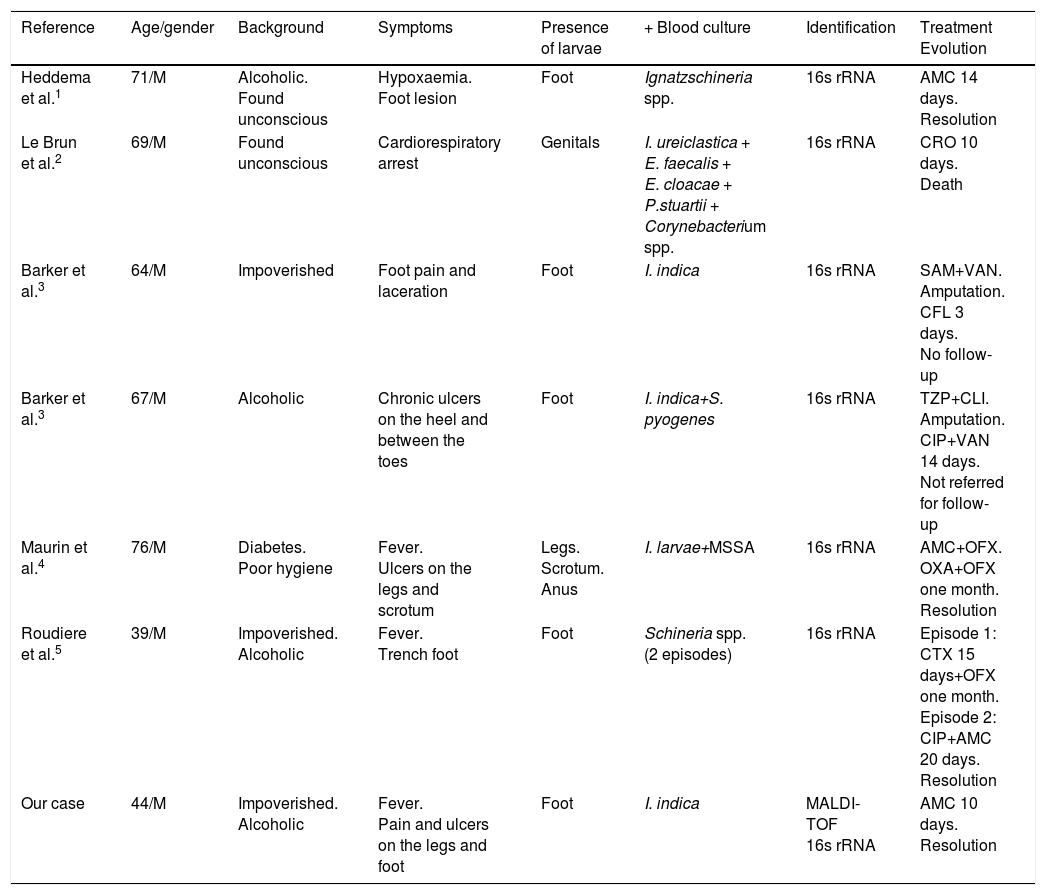
Six cases of bacteraemia due to Ignatzschineria spp. have been published in PubMed up to September 2017 (Table 1). All of them mention poorly cared for wounds with the presence of larvae being the likely bacteraemia source: 3 cases in France4,5,2; 2 in the USA3 and one in the Netherlands.1 The cases reported, which were treated with beta-lactam antibiotics, evolved favourably, with the exception of one patient who had been found unconscious and died.2 Evolutions were not disclosed in two patients.3 The strains were sensitive to beta-lactam antibiotics, quinolones and aminoglycosides, with varying antibiotics tested, since there is no standardised antimicrobial susceptibility test or cut-off point.
Reported cases of sepsis due to Ignatzschineria spp.
| Reference | Age/gender | Background | Symptoms | Presence of larvae | + Blood culture | Identification | Treatment Evolution |
|---|---|---|---|---|---|---|---|
| Heddema et al.1 | 71/M | Alcoholic. Found unconscious | Hypoxaemia. Foot lesion | Foot | Ignatzschineria spp. | 16s rRNA | AMC 14 days. Resolution |
| Le Brun et al.2 | 69/M | Found unconscious | Cardiorespiratory arrest | Genitals | I. ureiclastica + E. faecalis + E. cloacae + P.stuartii + Corynebacterium spp. | 16s rRNA | CRO 10 days. Death |
| Barker et al.3 | 64/M | Impoverished | Foot pain and laceration | Foot | I. indica | 16s rRNA | SAM+VAN. Amputation. CFL 3 days. No follow-up |
| Barker et al.3 | 67/M | Alcoholic | Chronic ulcers on the heel and between the toes | Foot | I. indica+S. pyogenes | 16s rRNA | TZP+CLI. Amputation. CIP+VAN 14 days. Not referred for follow-up |
| Maurin et al.4 | 76/M | Diabetes. Poor hygiene | Fever. Ulcers on the legs and scrotum | Legs. Scrotum. Anus | I. larvae+MSSA | 16s rRNA | AMC+OFX. OXA+OFX one month. Resolution |
| Roudiere et al.5 | 39/M | Impoverished. Alcoholic | Fever. Trench foot | Foot | Schineria spp. (2 episodes) | 16s rRNA | Episode 1: CTX 15 days+OFX one month. Episode 2: CIP+AMC 20 days. Resolution |
| Our case | 44/M | Impoverished. Alcoholic | Fever. Pain and ulcers on the legs and foot | Foot | I. indica | MALDI-TOF 16s rRNA | AMC 10 days. Resolution |
AMC: amoxicillin/clavulanic acid; CFL: cephalexin; CIP: ciprofloxacin; CLI: clindamycin; CRO: ceftriaxone; CTX: cefotaxime; M: male; MSSA: methicillin-sensitive Staphylococcus aureus; OFX: ofloxacin; OXA: oxacillin; SAM: ampicillin/sulbactam; TZP: piperacillin/tazobactam; VAN: vancomycin.
Ours is the first case described in Spain and the first one identified using MALDI-TOF; in the only other case that mentions the implementation of MALDI-TOF, no conclusive identification was achieved.1 We stress the difficulty of identification with standard microbiological methods. Thus, the isolation of gram-negative bacilli should be taken into account in blood cultures from patients with myiasis and adverse social circumstances (chronic alcoholism, hygiene deficit, poverty), which could belong to the Ignatzschineria genus. In case of patients with any of the cited risk factors, identification with MALDI-TOF mass spectrometry or 16s rRNA amplification and sequencing is required.
Please cite this article as: Rodríguez-Zúñiga D, González-Galiano N, Leal-Negrado Á, Hidalgo-Pérez E. Primer caso de sepsis por Ignatzschineria en España asociada a miasis. Descripción de un caso y revisión de la literatura. Enferm Infecc Microbiol Clin. 2019;37:64–65.
