




To analyze the current available evidence on non-pharmacological interventions for increasing the withdrawal of patients with substance use disorder.
MethodA systematic review of randomized clinical trials with a control group has been carried out where a non-pharmacological intervention is carried out in which nurses participate. The search was carried out in Pubmed, Cinahl, Web of Science, Scopus and Cochrane. randomized clinical trials with a control group published between 2018 and 2023 were selected.
Results15 articles were selected. A longer abstinence time was observed in the interventions that proposed a personalized telematic follow-up with a health worker, the establishment of the figure of the care coordinator or financial rewards based on the abstinence time. No significant differences regarding abstinence were observed in the formative interventions or with relaxation techniques only. However, relaxation techniques combined with other interventions could be effective.
ConclusionsThe identified interventions can be incorporated into nursing practice. They present encouraging results, although it would be advisable to study their long-term effectiveness.
Analizar la evidencia actual disponible sobre intervenciones no farmacológicas para aumentar el tiempo de abstinencia de pacientes con trastorno por consumo de sustancias.
Métodose ha realizado una revisión sistemática de ensayos clínicos aleatorizados con grupo control donde se lleve a cabo una intervención no farmacológica en la que haya participación enfermera. La búsqueda fue realizada en Pubmed, Cinahl, Web of Science, Scopus y Cochrane. Se seleccionaron ensayos clínicos aleatorizados con grupo control publicados entre 2018 y 2023.
ResultadosSe seleccionaron 15 artículos. Se observó mayor tiempo de abstinencia en las intervenciones que planteaban un seguimiento telemático personalizado con un sanitario, el establecimiento de la figura del coordinador de cuidados o recompensas económicas en función del tiempo de abstinencia. No se observaron diferencias significativas en la abstinencia en estudios que planteaban EPS o técnicas de relajación únicamente. No obstante, las técnicas de relajación combinadas con otras intervenciones sí podrían ser efectivas.
ConclusionesLas intervenciones identificadas pueden ser incorporadas a la práctica enfermera. Presentan resultados esperanzadores, aunque sería recomendable estudiar su efectividad a largo plazo.
- •
The increase in morbidity and mortality associated with substance use disorders means that researching and implementing nursing activities must continue to promote detoxification and its maintenance over time.
- •
Telematic monitoring, mentoring between patients and a system of financial rewards seem to increase abstinence times, and have a positive impact on the level of health of patients with substance use disorders.
Substance-related disorders (SRD) are a major public health problem. Their DSM-5 definition is "a maladaptive pattern of substance use, leading to clinically significant impairment or distress".1 The United Nations noted that between 2010 and 2019 the number of drug users worldwide increased by 22%.2 Similarly, the Spanish National Drugs Observatory recorded an increase in deaths due to acute reactions to substance use: 493 deaths in 2003 compared to 974 in 2020.3 This leads to lower adherence to antiretroviral treatment (ART) in HIV patients, increased risk of infection, and increased morbidity and mortality.4
A multidisciplinary approach, including nurses, is essential for a holistic perspective. Nursing activities related to SRD are listed in intervention 4514 of the Nursing Interventions Classification (NIC) "Substance Use Treatment: Drug Withdrawal", defined as "care of a patient experiencing drug detoxification".5 It was validated in 1992 and revised in 2013. However, the increase in morbidity and mortality associated with SRDs requires evidence-based nursing activities to promote detoxification to be ongoing.
A systematic review found that the use of digital devices (online platforms/applications) increased abstinence.6 Another study linked the practice of mindfulness to a reduction in stress and withdrawal symptoms.7 Physical exercise is also associated with better adherence to treatment and withdrawal symptoms.8 Another systematic review analysed the benefits of involving a family member during the patient’s detoxification, resulting in better maintenance of abstinence.9 However, some of these studies do not conduct post-intervention follow-up and therefore knowledge about long-term outcomes is lacking.6–12
The prevalence of SRD and their complications is increasing. It is imperative to explore the process of detoxification in depth and to investigate which activities are effective. Previous systematic reviews highlight the importance of learning what works for SRD patients to remain abstinent during and especially after intervention. Analysing different interventions such as incorporating a care coordinator or reward systems could foment a patient-centred approach and patient motivation to prevent drop-outs, and to prolong abstinence.
Which non-pharmacological nursing interventions are most effective in increasing abstinence in patients with an SRD? The main objective is to analyse the current available evidence on non-pharmacological interventions - which have emerged in the last 5 years - to increase abstinence time in patients with SRD that can be undertaken in part or in full by nurses.
The specific aim is to analyse the efficacy of non-pharmacological nursing interventions on:
- -
Partial or total reduction of use.
- -
Mental health measured as a reduction in stress, anxiety, or depression.
- -
Physical health understood as an improvement in adherence to pharmacological treatment, improvements in vaccination status, or implementation of healthy habits.
This systematic review was published according to PRISMA recommendations.13
Eligibility criteriaRandomised clinical trials (RCTs) were selected that involved a non-pharmacological intervention with a control group. We did not look for a specific intervention because there is a lack of literature, therefore, we looked for non-pharmacological interventions that could be performed in part or in whole by nurses. We chose studies whose results assessed abstinence, partial or total reduction of substance use, repercussions on physical health - such as improved adherence to pharmacological treatment, improvements in vaccination status, and implementation of healthy lifestyle habits - and/or mental health, such as a reduction in stress, anxiety, or depression.
Original published and control group RCTs were included. Participants had to be over 18 years of age, of either gender, with a diagnosis of SRD. Studies were included both in the general population and in patients belonging to a specific clinical centre. The interventions of the studies had to be within the competence framework of nurses. RCTs in Spanish or English published between 2018 and 2023 were selected as there are already systematic reviews on the same subject prior to 2018.10–12
Studies conducted in patients with tobacco or alcohol use disorders exclusively were excluded as there are specific nursing interventions for these addictions such as 4512 (Substance Use Treatment: alcohol withdrawal) and 4490 (Smoking Cessation Assistance).5 Unfinished studies, RCT protocols, or pilot studies were excluded.
Information sourcesThe following databases were consulted: SCOPUS, PUBMED, CINAHL, COCHRANE Database of Systematic Reviews, and WEB OF SCIENCE CORE COLLECTION.
Search strategyThe following descriptors and Boolean operators were used: ([“Substance-related Disorders”] OR ([“Opioid-related disorders”] OR [“Cocaine-related disorders”] OR [“Amphetamine-related disorders”] OR [“Heroin dependence”] AND [“Nurs*”] AND [“Clinical Trial”]).
Study selectionThe search and selection of studies took place from May 2022 to April 2023. The articles were reviewed individually with subsequent consensus.
Duplicate articles were identified and removed. Abstracts and titles were then reviewed by the reviewers for compliance with the criteria after a preliminary reading.
The full texts were read later. Articles were selected according to exclusion and inclusion criteria. Any disparity of opinion between reviewers was resolved by discussion and later consensus between reviewers and a non-reviewing external reviewer.
Extraction of resultsThree evaluators extracted the data. The type of intervention and its duration were collected. Data extraction was reflected in a table with the following variables:
- -
Type of drug(s) consumed
- -
Concomitant alcohol consumption: yes or no.
- -
Type of intervention performed.
- -
Duration of intervention and follow-up: weeks or months.
- -
Effectiveness of the intervention: in terms of abstinence time, total or partial reduction of use, impact on physical and/or mental health.
The results were synthesised in the form of tables containing the calculation of means, standard deviation, interquartile range, percentages, confidence intervals, and odds ratio. Given the heterogeneity of the included studies and their contexts, the variability of the interventions and the results, a meta-analysis was not performed because this could lead to bias in obtaining an overall effect estimator.13
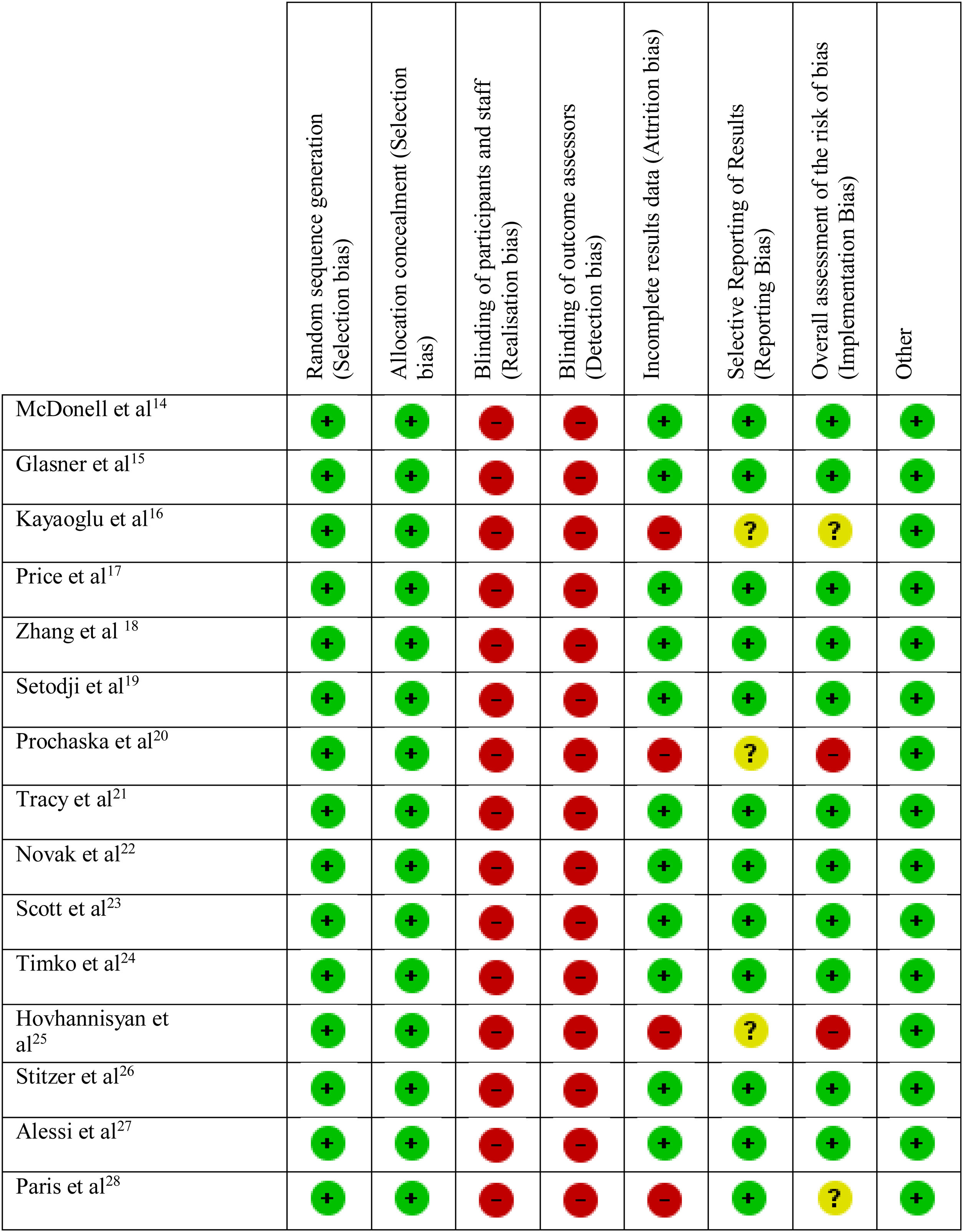
Risk of biasFollowing the recommendations of the Cochrane Collaboration, a risk of bias analysis was performed to analyse directly the specific characteristics of the studies and their results.13 We used the RCT risk of bias assessment tool recommended by the Cochrane Collaboration, which identifies five potential biases: selection, performance, detection, attrition, and reporting bias.13 These biases are broken down into the following domains: generation of the randomisation sequence, concealment of cluster allocation status, blinding of participants and/or the investigator, incomplete outcome data handling, selective outcome reporting, and other biases. Risk of bias is presented using the figure recommended by the Cochrane Collaboration.13
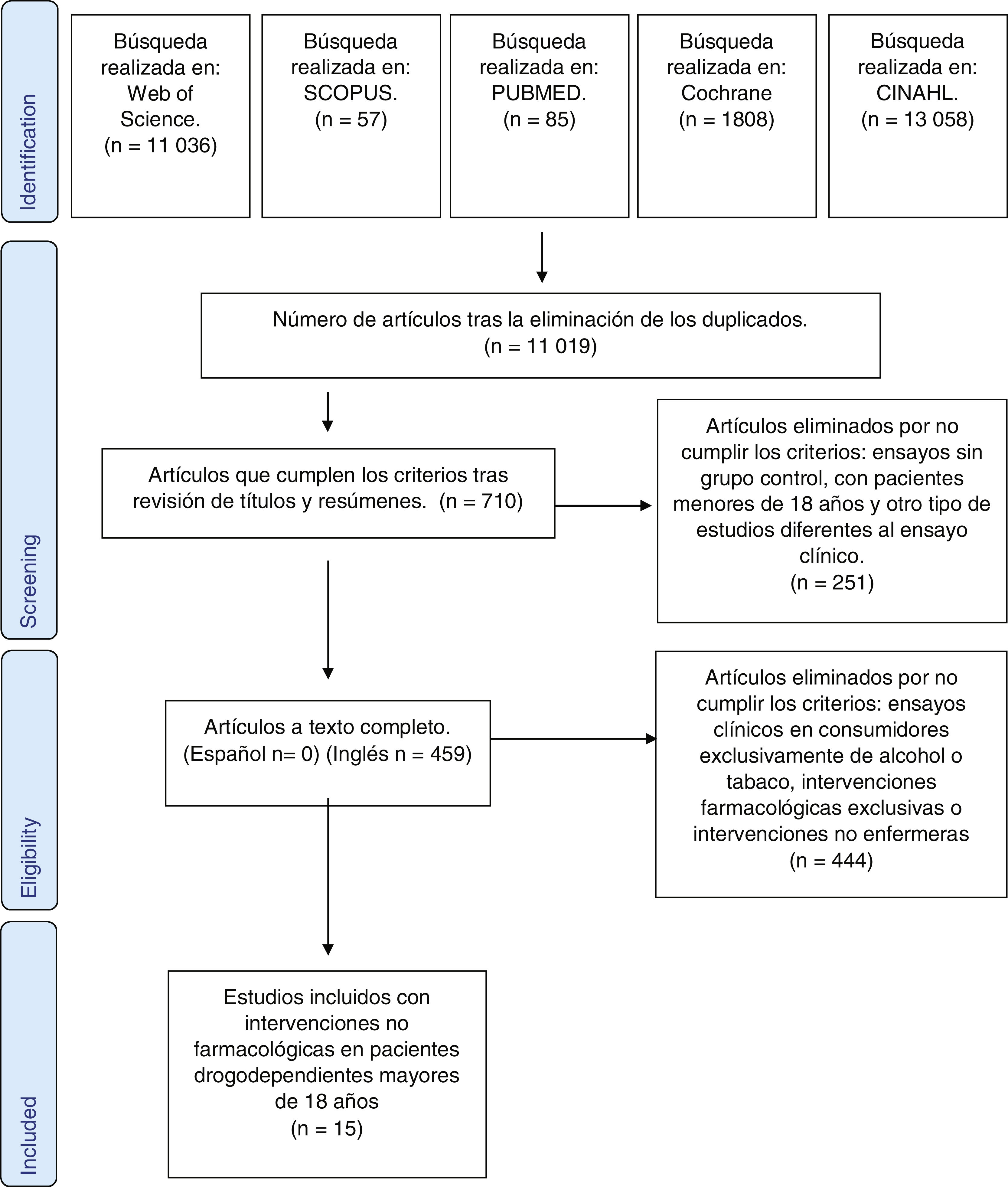
ResultsSelection of articlesAfter the search, duplicate articles were eliminated, and 11,019 articles were obtained. After reviewing titles and abstracts, 710 articles were obtained and reviewed in full text. Those that did not provide empirical data, were not relevant to the proposed objectives, were not RCTs, or did not have a control group were removed. Of the remaining 459 articles, those that reported data on alcohol and/or tobacco use only, as well as articles whose interventions did not fall within the competence of nurses, or were exclusively pharmacological, were eliminated. Finally, 15 articles were selected. The selection of studies is shown in the PRISMA diagram in Fig. 1.
Descriptive results of the studies
The characteristics of the studies are listed in Table 1. All studies were RCTs with varying sample sizes, from n = 50 patients to n = 801, including 3,382 patients in total.
Description of selective studies.
| Authors, year of publication, and country. | Sample size and study type. | Drugs used | Patient age and gender | Intervention time | Intervention type | Effects on abstinence time and relapses | Effects on physical or mental health |
|---|---|---|---|---|---|---|---|
| McDonell et al.14 (2022) USA | 114 subjects RCT | AmphetaminesCannabisCocaineMethamphetaminesOpioidsAlcohol | 49.12% male50.88% female. Mean age: 35.80 years (SD:10.40 years) | 12 weeks and 6 months subsequent follow-up. | Study where the intervention consists of giving a financial incentive to patients who remain abstinent and attend follow-up appointments with the research team. Intervention groups: 3 groups receive CM and a financial reward for abstinence time (mean amount: $155.22 (SD: $324.64)1.CM in the alcoholic group2.CM in the drug dependent group3.CM in the alcohol and drug group. Control group: follow-up in primary care on an individual basis. Prior to and during the study, weekly meetings were held between the team, the principal investigator, and the coordinators of the dispensing centre. The staff in charge of providing financial incentives were experts in CM.Urine samples were collected to monitor substance use. | The three groups receiving CM had a higher percentage of alcohol-abstinent urine samples at 12 weeks.Percentage of stimulant-, cannabis-, and opioid-abstinent urine samples at 12 weeks, 3 months, and 6 months: CM + drugs: 94.42%, 68.53%, 96.83%.CM + drugs and alcohol: 87.80%, 78.86%, 96.33%.Control group: 65.90%, 51.92%, 96.92%.OR in the CM + Drugs group: 4.770 (95% CI: 3.004−7.573)OR in the CM + Alcohol and drugs group: 4.231 (CI: 2.641−6.777)The urine specimen submission protocol was more strictly adhered to in all intervention groups compared to the control group. Percentage of samples not submitted: Control group: 47.46% CM + drugs: 36.98% CM + drugs + alcohol: 23.56%. | There were no differences in attendance at routine health checks between groups. |
| Glasner et al.15 (2022)USA | 50 subjectsRCT | AmphetaminesCannabisCocaineOpioidsStimulantsAlcohol | 80.00% male20.00% female. Mean age: 47.70 years (SD: 8.20) | 12 weeks | Study establishing telematic follow-up and reinforcement of abstinence by text message.Intervention group: TXT-CBT: the patients received a daily text message for 12 weeks to prevent relapse, avoid risk behaviours, manage abstinence, HE on lifestyle changes, social support, and positive reinforcement of achievements.Control group: information leaflet on HIV and drug abuse. The healthcare worker responsible for communication with patients received prior training in cognitive behavioural therapy. Data were collected by research staff with expertise in data collection.Urine samples were collected to monitor substance use. | No significant differences in amphetamine or stimulant use were observed in the urine samples for substance monitoring. The intervention group had lower OR for opioid use (OR = .50, p = .04, 95% CI:.25,.98) and for cocaine use (OR = .48, p = .05, 95% CI:.22,.99) | Adherence to anti-retroviral treatment is higher in the intervention group. At the end of the intervention, it was observed that the HIV viral load of the intervention group was: 3.38 copies/mL, SD = 2.03) VS. the HIV viral load of the control group: 4.88 copies/mL, SD = 2.34), t(49) = 2.42, p = .02; d = .68 |
| Kayaoglu et al.16 (2021) Turkey | 62 subjects RCT | Alcoholand drugs (does not specify) | 100.00% males. 20 subjects aged between 18.00 and 23.00 years.42 subjects over 24.00 years. | 3 weeks with subsequent follow-up at 4 and 6 months. | A study where the intervention consists of cognitive therapy sessions followed by listening to relaxing music. Intervention group: 25−30 min. of psychoeducation and cognitive therapy and 30 min. of relaxing Turkish music ("Maqams") followed by relaxation exercises). Control group: routine follow-up at the patient’s request. Measurement of stress level at the end of the intervention, at 4 months, and at 6 months using the perceived stress scale.The topics of the psychoeducation sessions were agreed beforehand in a preliminary session with the intervention group. The principal investigator with training in cognitive therapy conducted the sessions. It is not specified whether the principal investigator had received previous training in relaxation techniques. | There were no statistically significant differences in abstinence time at 4 months post-intervention as measured by the PSS questionnaire. At 6 months there was 66.7% abstinence in the intervention group vs. 40.6% abstinence in the control group. (χ2 = 4.21) (Δ: 60; SD: 15.38) | Mean post-test, 4-month, and 6-month PSS scores: Intervention group: 31.36 (SD: 10.72)37.06 (SD: 9.53)42.13 (SD: 8.36)Control group: 45.43 (12.06)45.15 (8.52)44.34 (7.51) |
| Price et al.17 (2019) USA | 187 subjectsRCT | CannabisAlcoholPrescription opioidsNarcotics | 100.00% female.Mean age 35.00 years (SD: 20.00−61.00) | 3 months of intervention with follow-up at 6 and 12 months. | Study where one intervention consists of a continuity of care programme including psychoeducation sessions on relapse prevention, abstinence, and mindfulness; and another intervention consisting of HE on sexual and reproductive health and cardiovascular health and healthy lifestyle habits. TAU group (control): 2−3 sessions per week for 1.5 h over 14 weeks based on a continuing care programme (follow-up, relapse prevention)WHE + TAU group: HE for women on reproductive health, nutrition, and cardiovascular health beginning with a 30-min discussion, 45 min of HE, and 15 min discussion of what was learned. MABT + TAU: psychoeducation (30 min) mindfulness, and physical and emotional awareness (45 min) and discussion about practice (15 min). The sessions were delivered by health research staff with expertise in the field of addictions and psychoeducation. Data on emotional dysregulation were collected through interviews, telephone calls, and consultation of medical records. Results were collected by questioning patients and through questionnaires. | At 6 months the MABT and WHE groups had more mean days of abstinence compared to the TAU: 11.6 (95% CI: 2.2−21.0) and 10.6 (95% CI: .7−20.6) At 12 months the MABT group saw more days of abstinence compared to the TAU group: 22.4 (95% CI: 4.5−40.3) (χ2 = 6.95)No reduction in withdrawal symptoms was observed between the MABT and WHE groups. Significant differences were observed between the MABT and TAU groups in withdrawal symptoms at 6 and 12 months respectively (-5.5; 95% CI: −8.5 to −2.5) (−4.0; 95% CI: −7.4 to −.5) (χ2 = 13.7) | At 3 months less emotional dysregulation was observed in the MABT compared to the TAU group (−14.2 (95% CI: −23.6 to −4.9) as well as for the MABT and WHE group (−13.8; 95% CI: −24.3 to −3.3) No significant differences in the degree of depression were observed between the three groups. |
| Zhang et al.18 (2018) USA | 451 subjects.RCT | AmphetaminesMethamphetaminesCocaine | 100.00% subjects of non-binary sex. Mean age: 34.25 years (SD: 8.20) | 12 weeks with follow-up at 4 and 8 months. | Study where the intervention consists of a nurse case manager undertaking follow-up, HE on vaccination, substance use, SRD prevention, and positive reinforcement to maintain abstinence. Nurse Case Management (NCM) + CM: 8 20-min sessions. Training on the benefits of vaccination, reduction of stimulant use, SRD prevention, reinforcement of positive behaviour, and patient empowerment. SE (Standard education) + CM: One 20-min session on the risks of substance dependency and hepatitis A/B vaccination. The CM nurses belonged to teams of nurses specifically addressing and researching coping strategies, interpersonal relationship management, community resources, promotion of vaccination and health education. Urine samples were collected for substance use monitoring. | Reduction in urine samples positive for methamphetamine, amphetamine, and cocaine in both groups (p: .001)(t = 2.04)Initial percentage of cocaine- positive samples: NCM + CM: 31.85% and SE + CM: 33.33%Percentage at 8 months of cocaine-positive samples: NCM + CM: 10.37% and SE + CM: 6.09%Initial percentage of methamphetamine-positive samples: NCM + CM: 73.33% and SE + CM: 72.34%Percentage at 8 months of cocaine-positive samples: NCM + CM: 24.44% and SE + CM: 29.79%Initial percentage of amphetamine-positive samples: NCM + CM: 49.63% and SE + CM: 48.74%Percentage at 8 months of cocaine-positive samples: NCM + CM: 21.48% and SE + CM: 24.82% | At 8 months 85.9% of the NCM + CM group had received vaccines against HBV and HAV compared to 84.8% of the SE + CM group (t = 11.75; d: .13). |
| Setodji et al.19 (2019) USA | 258 subjects. RCT | OpioidsAlcohol | 24.04% female,75.96% male. Mean age: 42.10 years (SD: 12.10) | 30 days and follow-up of 6 months. | Study that evaluates the effectiveness of collaborative care through the nurse case manager in charge of monitoring patients for their detoxification.Intervention group: Collaborative care model: there is a care coordinator with a database to recruit patients with addictions. After confirming substance dependence, they refer them to a health professional for follow-up and addiction treatment. The patient's progress and absences from therapy are tracked by a computer programme that notifies the care coordinator.Both the care coordinator and the health professionals receive prior training in motivational interviewing and cognitive therapy from the “Motivational Interviewing Network of Trainers” programme. Control group: subjects were given a telephone number of medical centres and offered the possibility to talk to a therapist. Consumption was monitored by interviewing the patients. | Collaborative care increased abstinence in the intervention group by 11.7% at baseline. ([95% CI: .9%, 22.3%, p: .03] or 32% proportion of the total effect).There is no significant difference in maintenance of abstinence over 6 months between the two groups. | In the group of drug and alcohol users, abstinence was 19.4% compared to 11.7% in the alcohol-only group.The patients in the control group did not seek medical or therapeutic help. |
| Prochaska et al.20 (2021) USA | 180 subjects RCT | BenzodiazepinesCannabisCocaineMethamphetaminesOpioidsAlcoholPrescription opioidsHallucinogens | 65.00% female and 35.00% male.Mean age: 40 years (SD: 12.00) | 8 weeks. | Study where the intervention is a smartphone application with educational content, where the user also registers each day their status in relation to detoxification.Intervention group: daily messages offering treatment support, tools to reduce use and withdrawal symptoms delivered via an app (Woebot) to the user. It offers mindfulness services, relapse prevention, and content related to CBT. Users can record their mood, withdrawal symptoms, and degree of pain.Control group: healthcare services on demand (hospitalisation and primary care).The research team received prior training on how the application works. | Reduction in substance use in the intervention group (F [1.148] = 4.53)In the first 30 days mean reduction in use was greater in the intervention group (−9.6 [SD: 2.3]) versus the control group (−3.9 [SD:2.2]; eta2: .029)There were no significant differences in substance use at the end of the study. | There were no significant differences in the degree of depression, anxiety, or pain between the two groups. |
| Tracy et al.21 (2020) USA | 65 subjects (RCT) | CannabisCocaineOpioidsAlcohol | 73.84% male 23.16% female. Mean age: 47.00 years (SD: 13.00) | 12 weeks with follow-up up to 24 weeks. | Study where the intervention is client-to-client mentorship. Patients who have been in withdrawal for the longest time mentor those who are starting the process. Intervention group: a group of ex-users (mentors) were trained for more than 6 months, 2 h per week for 1 month (explanation of the process, setting boundaries, tools for the mentee to remain abstinent, maintaining the mentor's own abstinence, managing self-harm attempts, reducing HIV risk behaviours, and managing mental health problems. Mentors coach their mentees through the process of detoxification (1−4 hours per week in person or by text message) An abstinence-based relationship is formed. Mentors, mentees, and healthcare professionals meet for 1 h once a week for monitoring and conflict resolution. Control group: pharmacological treatment and follow-up in consultation. A healthcare professional with previous training in mentoring and goal achievement coordinates this project. Abstinence was measured using the Addiction Severity Index (ASI-6) and urine analysis. | A decrease in the mean time of substance use, measured in days, was observed in the intervention group versus the control group over the first 12 weeks. (Intervention group: 4.10 [SD: 7.30] VS. Control group: 16.60 [SD:21.00]) (Z [1]: 2.50, D: .6)A decrease in the mean time of substance use, measured in days, was observed in the intervention group versus the control group during weeks 13−24.(Intervention group: 1.90 [SD: 4.80] VS. Control group: 5.60 [SD: 7.40]) (Z [1] = −2.03, d: .76) | Reduction in ASI-6 scores between weeks 13 and 24 on drug use (b: −.02 SD: .01, t (47): −2.36) compared to the control group, where they increased (data not available). |
| Novak et al.22 (2019) USA | 91 subjectsPhase 2 of an RCT. | OpioidsCocaine | 55.00% male, 45.00% female. Mean age: 48.00 (SD: 8.05) | 12 months with post-intervention follow-up at 3, 6, 9, and 12 months. | A study where the intervention was abstinence-contingent wage supplements and community work.Participants are eligible for payment for undertaking community work. They start with basic computer training and are then eligible for a paid activity.Intervention group: Participants are employed in community jobs and get paid ($8 per hour). They are mentored by an employment specialist.In addition, they submit urine samples for drug testing 3 times a week. If the sample is opiate- and cocaine-positive, $1 is deducted from their pay.Control group: access to pharmacological treatment and consultation with health professionals on demand.It is not specified whether the team received prior training.Results were collected by questioning patients and through questionnaires | At the end of the intervention, the percentage of opiate- and cocaine- negative urine samples was higher in the intervention group (63.6%) compared to the control group (44.1%).(OR: 2.76 [95% CI: 1.35−5.63])No significant differences were found in urine samples over the following 12 months post intervention. | The percentage of employability in the intervention group (38.10%) was higher than in the control group (10.10%) at the end of the intervention.(OR: 5.91 [95% CI: 2.40−14.58])At the end of the intervention, the percentage of patients out of poverty was higher in the intervention group (25.00%) compared to the control group (9.00%).(OR: 3.37 [95% CI: 1.37−8.28]) |
| Scott et al.23 (2020) USA | 401 subjects(RCT) | AlcoholStimulantsOpioidsCannabisOther | 39% female 61% male. Mean age: 44.20 years (SD: 11.00) | 6 months with 6 months post-intervention follow-up. | Study where the intervention is a smartphone application with HE content in relation to substance use and habits, relapse prevention, and hotlines with nurses in the case of substance use.The team received prior training on how to use the application. There were 3 intervention groups where subjects were given a smartphone with an EMI or EMA-based application. All received one hour of pre-training on the use of the smartphone and one hour of training on relapse prevention. EMI ("Ecological Momentary Interventions"): an application based on relapse prevention: it sets up hotlines, treatment centre locators, web pages to make face-to-face or online appointments with professionals. It includes mindfulness tools, music, games, and physical and mental exercise. It also includes schedule organisers and recovery literature. EMA ("Ecological Momentary Assessments"): a set of 28 items where users record their use and the characteristics of the environment 30 min prior to use (people, feelings, physical places, thoughts, activities). If they remain abstinent, they record the protective factors that favour abstinence (people, feelings, physical places, thoughts, activities). The questions about the substance use environment are randomised and the response time is 2−3 min. EMI + EMA: subjects use both applications. When they complete the EMA, they receive a message about their relapse risk from 1 to 3, and the app redirects them to the EMI. Control group: They received a 1 -h training on relapse prevention. The research team received prior training on the use of the app. Outcomes were measured by analysing urine samples and questioning patients. | EMI group: increase in mean abstinence time at 6 months. In the EMI group, abstinence was observed from 58 to 66 days (Z-indicator: .21), compared to 62 to 59 days in the EMA and control groups (Z-indicator: −.01).(F(2,734) = 4.85, effect size f = .11, 95% C.I. [.02, .18])EMA group: No significant differences were found in the mean days of abstinence between the group using the EMA application versus the control group. EMI + EMA group: There were no significant differences in mean abstinence time. Patients in this group used the EMI app more (92% in the EMI group vs. 96% in the EMI + EMA group (F (1,199): 4.1, Cohen's f: .14 (95% CI [.00−.28]) | The variables ("proportion of weeks using EMI" and "frequency of listening to music via EMI") predicted 7.2% of the variance in days of abstinence (F [2.195.]: 7.56. 95% CI: .01−.14). |
| Timko et al.24 (2019) USA | 298 subjects. (RCT) | AlcoholOpioids | 94.96% male, 5.04% female. Mean age: 50.14 years (SD: 13.20) | 12 weeks with follow-up at 3 and 6 months. | Study evaluating the efficacy of telephone monitoring during detoxification.Intervention group: ETM ("Enhanced telephone monitoring"): single, individual 50-mi session and 12 15-min sessions via telephone over 12 weeks with the same health professional as the initial session. In the initial session, the health professional explains how telephone monitoring works, encourages empathy, reinforces the patient's commitment to abstinence and their tools for maintaining abstinence. Pharmacological alternatives are explained, and the patient is invited to weekly meetings with other patients in the same situation. The patient completes the "Risk Assessment Worksheet" over the 12 weeks. In addition, the patient is reminded that there are weekly meetings where it is advisable to attend with patients in the same situation and it is insisted that they attend to receive their pharmacological treatment at the detoxification centre (if the patient is receiving medication) Patients received reinforcements in the form of a certificate plus medallion. Control group: pharmacotherapy and outpatient follow-up by the health staff of the detoxification centre. The professionals did not receive any prior training. Substance use was monitored by means of questionnaires (ASI-6 and "Risk Assessment Worksheet") | At three months after the intervention, a higher percentage of patients in the control group had to be admitted to hospital for additional detoxification compared to those in the intervention group who required fewer hospital admissions. Control group: 38.60% VS. 24.43% of the intervention group (B/F: −.670)ASI-6 scores were lower for the intervention group than the control group. At 3 months: Intervention group: Drug Addiction Severity: .04 (SD: .07) Control group: Drug Addiction Severity: .06 (SD: .09) At six months, the severity of drug addiction is lower in the intervention group (.05 [SD: .09] compared to the control group [.07 SD: .10]) | The degree of self-confidence using the Brief Situational Confidence Questionnaire. Patients in the intervention group showed higher rates than the control group. At 3 months and at 6 months: Intervention group: 3 months: 75.84 (SD: 25.15), 6 months: 72.94 (SD: 26.80)Control group: 3 months: 68.98 (SD: 28.91)6 months: 68.94 (SD: 26.82) |
| Hovhannisyan et al.25 (2020) Sweden | 212 subjects (RCT) | AlcoholDrugs (not specified) | 6 weeks with 12 months follow-up. | Study evaluating the effect of a HE intervention on healthy habits. Intervention group: VIP ("Very Integrated Programme"): observation and recording of patient habits (smoking, diet, physical activity). 60–90-min meeting to define the changes to be achieved in terms of lifestyles. Advice on smoking cessation, nutritional and physical exercise advice, and HE on comorbidities and drug use were included. Control group: pharmacological treatment and consultations with health professionals on demand.The team received prior training on motivational interviewing. Use was monitored by means of questionnaires. | No statistically significant differences were observed in the mean number of days without substance use, the percentage of relapses or the mean number of treatment days at 6 months.At 12 months, a longer time without substance use was observed in the control group compared to the intervention group (265 days vs. 139) | No statistically significant differences in cardiovascular risk factors were found at any time point. | |
| Stitzer et al26 (2021) USA | 801 subjects(RCT) | CannabisOpioidsCocaineAlcoholAmphetaminesEcstasy | 67% male 33% female. Mean age: 45.00 (SD: 12.10) | 6 months | Study where the intervention consists of giving users abstinence-contingent financial incentives, attending healthcare appointments, and taking ART.Patient navigation (PN) intervention group: patients work with a patient navigator over 11 sessions. The navigator highlights the participants' capabilities, reinforces their motivation, informs them about drug substitution treatment, and encourages adherence to ART.Intervention group: PN + CM: subjects have the same sessions as the PN group but receive financial incentives of up to $1160 ($220 for attending sessions with the PN, $80 for completing documentation and questionnaires, $230 for attending HIV follow-up visits, $90 for taking substance abuse treatment, $220 for providing drug-negative urine samples).It is not specified whether the professionals received prior training.Use was monitored by analysing urine samples and completing questionnaires. | The percentage of adherence to substance abuse treatment was higher in the PN + CM group than in the CM group (PN = 25.5%; PN + CM = 47.6%; p < .001) (χ2: 28.07 df = 1)Patients in the PN + CM group submitted more urine samples than those in the PN group (PN mean: 2, IQR = .5; PN + CM mean: 8, IQR = 5,10; p < .0001).At 3 months only 20% of urine samples in the PN group were negative, compared to 50% in the PN + CM group.At 6 months only 18% of urine samples from the PN group were negative, compared to 52% from the PN + CM group.(OR = 4.5, 95% CI 3.0−6.7) | Viral load suppression in the NP + CM group was 54% (χ2: 4.50) compared to 50% suppression in the NP group 50% (χ2: 6.70) |
| Alessi et al.27 (2020) USA | 120 subjects (RCT) | CocaineOpioidsMarihuanaMethamphetaminesAlcohol | 75.83% male, 24.17 female. Mean age: 38.00 years (SD: 10.35) | 15 weeks and 12 weeks subsequent follow-up. | Study where there are two types of interventions, either receiving contingency management financial incentives or a physical exercise programme.CM group: the patient receives contingency management financial incentives on attending group therapy sessions and submitting urine samples. Incentives could be stereos, TVs, or $100 gift cards.Intervention group: CM + exercise: The American College of Sports Medicine gave an informative talk on healthy exercise. They prescribed exercises for each patient based on their physical condition and gave exercise recommendations for withdrawal. The target was 15−20 min of brisk walking, 3 or 4 times a week. In addition, achievements were positively reinforced as in the CM group.Use was monitored by analysis of urine samples and questionnaires. | No statistically significant differences were observed in the percentages of drug-negative urine samples.There were no statistically significant differences in the mean number of days of abstinence | The CM + exercise group recorded improvements in sleep quality (Pittsburgh Index).At baseline, time β1 for the CM group: −.01, at 12 months, −0.07(t-ratio: −2.41 and −0.97 respectively).At baseline, time β1 for CM + exercise group: −.01, at 12 months, .01.(t-ratio: −2.86 and −2.59 respectively) (d: .50) |
| Paris et al.28 (2018) USA | 92 subjects (RCT) | CocaineMarihuanaOpioidsAlcoholBenzodiazepinesHeroin | 33% female and 66% male. Mean age: 43 years (SD: 7.03) | 8 weeks with 6 months follow-up after the intervention. | Study in which the intervention consists of a computer programme with content on cognitive behavioural therapy, HE on detoxification, and maintenance of abstinence.Intervention group: CBT4CBT (Computer Cognitive Behavioural Therapy plus treatment as usual): website for Spanish speakers with cognitive behavioural therapy on coping with craving, problem solving, assertiveness, decision making, recognising, and changing thoughts. Various strategies are used such as graphics, voice-overs, interactive exercises, and true-false questions to check that the subject has learned the content. A video shows how to operate the website. The contents were translated and adapted to the values of Latino culture (respect, trust, gender-specific values, family orientation, fatalism, wisdom, and value of interpersonal relationships)Control group: conventional treatment: group therapy, follow-up in consultation and pharmacological treatment.It is not specified whether the team of professionals received prior training.Consumption was monitored by analysing urine samples and completing questionnaires. | The mean percentage of days abstinent is higher in the intervention group than the control: 76.90% (SD: 24.70) versus 62.20 (SD: 37.60) (f: 4.54).The percentage of urine negative for all drugs was 42.90% in the intervention group versus 37.40% in the control group (f: 0.37; d: .12) | The degree of anxiety or depression was not found to have any effect on abstinence time. |
Results with p < .05 were considered statistically significant differences.
The percentage of females ranged from 0% to 100%. One study included a non-binary gender population (n = 451 patients).
All studies were conducted in the USA (n = 13), except two, undertaken in Turkey and Sweden.
The studies included general population, inpatients, outpatients, patients in detoxification and/or rehabilitation programmes, or HIV-positive patients with inpatient follow-up. One study included patients from a rural American Indian community.14
The main substances used were opioids, cannabis, cocaine, and concomitant alcohol. All patients received their usual pharmacological treatment.
Post-intervention follow-up ranged from 30 days to 12 months.
Abstinence was monitored by collecting urine samples for toxicity analysis (amphetamines, methamphetamines, cannabis, cocaine, and opioids) (n = 9), questioning patients (n = 4), or through questionnaires (n = 9). In two studies they interviewed patients and used questionnaires. Five used questionnaires and urine samples.
The main questionnaires used were the Addiction Severity Index (n = 4), the Drug Screening Questionnaire (n = 1), the Brief Addiction Monitor (n = 1), and the 15-item-Short Inventory of Problems- Alcohol and Drugs (n = 1).
Effectiveness of interventions with telematic or virtual follow-up on abstinenceIn 5 studies, patients were followed up telematically or virtually. All patients received information on maintenance of abstinence. In two studies, patients received this information by text message.15,20 In another study, patients completed questionnaires and activities on a website.28 The message service of the study by Glasner et al. offers an individualised relapse prevention plan.15 In the study by Scott et al., the app offers a relapse action plan with emergency hotlines, treatment locators, and the possibility to meet with a healthcare professional in person or online.23 In the study by Timko et al., follow-up was by telephone and personalised with the same professional throughout the intervention.24
The studies included post-intervention follow-up during which patients periodically submitted urine samples for drug testing and reported their substance use.
All found significant differences in abstinence between the intervention and control groups. Those providing personalised management recorded higher post-intervention abstinence. The two studies where the content of the apps was formative, or communication was with an automated agent recorded significant differences only at the beginning of the intervention (F [1.148]: 4.53; eta:2 .029)20 (F: 0.37; d: .12).28
Effectiveness of interventions including physical exercise and/or relaxation on abstinenceTwo studies found that mindfulness and listening to relaxing music increased abstinence only in the first six months combined with cognitive therapy sessions.16,17 In one study, 66.7% of the patients in the intervention group remained abstinent compared to 40.6% in the control group (χ2: 4.21; (Δ: 60; SD: 15.38).16 The implementation of an exercise plan did not seem to have an impact on abstinence.17
Effectiveness of health education (HE) on abstinenceAnother study used healthy lifestyle education as an intervention.25 No changes in consumption or abstinence were observed between the intervention and control groups.
In another study, training and follow-up provided by nurses increased abstinence in both groups. An overall decrease in methamphetamine use of 70% from baseline was observed (p: .001).18
The study by Setodji et al. observed that a care coordinator, who manages the patient from intake to referral for treatment with other professionals, increased abstinence by 11.7% in the intervention group in the first 30 days (95% CI: .9%, 22.3%; p: .03).19
Effectiveness of mentoring on abstinenceTracy et al. established that patients who had been abstinent for more than six months mentored patients initiating detoxification. Less substance use was observed at follow-up (Intervention group: 1.90 [SD: 4.80] VS. Control group: 5.60 [SD: 7.40]) (Z [1]: −2.03, d, d: .76).21
Effectiveness of financial incentives on abstinenceIn three studies, patients received a financial reward for remaining abstinent, taking treatment, and attending consultations.14,22,26 In all studies, abstinence was higher in the intervention group. In one study, the percentage of abstinent patients in the intervention group increased from 94.42% to 96.83% at 6 months post intervention (OR: 4.770 [95% CI: 3.004−7.573]).14 In another, at 6 months post-intervention, 52% abstinence was observed in the intervention group compared to 18% in the control (OR: 4.5, 95%CI 3.0−6.7).26
Effectiveness of interventions on physical and/or mental healthTwo studies found that after cognitive therapy and then listening to relaxing music, stress levels decreased and emotional regulation increased.16,17
Two studies encouraged physical exercise.25,27 One showed no significant differences after including healthy lifestyle habits.25 In another study, sleep quality increased in the intervention group (t-ratio: −2.59, d: .50).27
Two studies observed a relationship between telematic follow-up during weaning and improved adherence to ART in HIV patients (t [49] = 2.42; d: .68)15 (53% VS. 37%; χ2 = 13.06, p < .005).26 In a study where follow-up was performed by nurses, an HBV/HAV vaccination rate of 85.9% was observed in the intervention group VS. 84.8% in the control (t: 11.75; d: .13).18
Analysis of biasOf the fifteen studies selected, eleven were rated at low risk of bias, two at high risk, and two at unclear risk of bias. The overall assessment of the risk of bias is shown in Fig. 2. The absence of blinding could lead to an overestimation of the effect, where patient perception could vary because they are aware of the intervention. Another potential bias is regression to the mean in studies where patients completed questionnaires resulting in an attenuation of the real effect of the interventions.
Discussion
The aim of this systematic review is to analyse non-pharmacological interventions that can be performed by nurses within the multidisciplinary team to support the detoxification of patients with SRDs. In view of the results, nurses can approach this disorder from various perspectives.
Health education - defined as "the action taken in individuals to bring about changes in their behaviour and environment"29 - is part of the competence framework of nurses. In none of the studies that included education on healthy lifestyle habits were improvements in abstinence observed,25,27 although the combination of HE and telematic monitoring does seem to increase abstinence. The results are more positive when the follow-up is personalised and the patient can communicate daily with the professional, especially in the event of withdrawal symptoms.15,20,23,24,28 This personalised follow-up has other benefits such as increasing the HBV/HAV vaccination rate and adherence to ART in patients with HIV.15,18 Both of these actions fall within the competence of nurses.
Relaxation techniques seem to reinforce abstinence, but not for the entire follow-up time. This is in line with another systematic review where meditation and relaxation were found not to be associated with longer abstinence time.30 However, relaxation techniques combined with personalised telephone follow-up may promote abstinence.17,24 Lagisetty et al. observed how the combination of several non-pharmacological interventions (cognitive therapy, exercise, mindfulness, and educational reorientation) promoted abstinence.10
Positive reinforcement is key to entrenching behaviours.12 Sustained positive results were observed in studies where patients were remunerated financially for attending follow-ups and remaining abstinent.11,19,23 This raises an ethical conflict as other patients are not remunerated for attending follow-up.12 It would be interesting to analyse whether patients experience more relapses after the remuneration has come to an end. One alternative is that proposed by Novak et al.22 where patients received money for doing community work and not just for remaining abstinent. Another possibility would be to reward patients' progress with responsibilities, such as client-to-client mentoring.21 Nurses can take on this competence by managing this remuneration or structuring the mentorship system. There is already the nurse case manager role, which has been found to reduce relapse and increase abstinence.18,19
Telematic monitoring, relaxation techniques, HE, case management, client-to-client mentoring, and reward management can be developed autonomously by nurses, as these activities, based on a continuum of care, belong to the fields of nursing care, management, and teaching. Physical exercise programmes, cognitive therapy, or the prescription of ART are activities that nurses can undertake interdependently with other professionals.
The main strength of the study is that it summarises the most relevant findings of the non-pharmacological interventions delivered in the last 5 years that can be conducted simultaneously while the patient is receiving pharmacological treatment. It highlights the figure of the care coordinator, emphasising the importance of nurse management. It also proposes using new tools such as apps that did not exist when the intervention was reviewed in 2013. Finally, it proposes nursing interventions with clear benefits in reducing substance use during the first year of follow-up.
The main limitation is the lack of blinding in the interventions. This could positively influence the results; as well as the heterogeneity of the interventions and their follow-up time. The lack of literature made it impossible to choose a single intervention. Studies with longer post-intervention follow-up and implementation of interventions in homogeneous populations with similar substance use patterns would be desirable.
In conclusion, telematic follow-up, reinforcement of abstinence through financial rewards and mentorship between SRD patients are effective methods to increase abstinence. These interventions could be delivered by nurses, but studies with longer follow-up are needed to assess the long-term effectiveness of these interventions.
FundingNo funding was received to undertake this study.
Conflict of interestThe author has no conflict of interests to declare.
Acronyms and abbreviations in alphabetical orderART: Antiretroviral therapy.
ASI: Addiction Severity Index.
CBT4CBT: Computer Cognitive Behavioural therapy plus treatment as usual.
CI: Confidence Interval.
CM: Contingency Management: A technique that provides incentives to reinforce achievement.
D: Cohen’s D.
DSM-5: Diagnostic and Statistical Manual of Mental Disorders.
EMA: Ecological momentary assessments.
EMI: Ecological momentary interventions.
ETM: Enhanced Telephone Monitoring.
HAV: Hepatitis A virus.
HBV: Hepatitis B virus.
HIV: Human immunodeficiency virus.
HE: Health education.
IQR: Interquartile range.
MABT: Mindful Awareness in Body-oriented Therapy.
M: Mean.
NCM: Nurse case Management.
NIC: Nursing interventions classification.
OR: Odds Ratio.
PN: Patient Navigation.
PSS: Perceived Stress Scale.
RCT: Randomised clinical trial.
SD: Standard deviation.
SE: Standard Education.
STD: Sexually transmitted disease.
TAU: Treatment as usual.
USA: United States.
SRD: Substance related disorder.
VIP: Very integrated programme.
VS: Versus.
WHE: Women's Health Education.
$: Dollars.
Thanks are due to all the staff of the library of the Universidad.
Complutense de Madrid for their help in obtaining the articles for this systematic review.
