




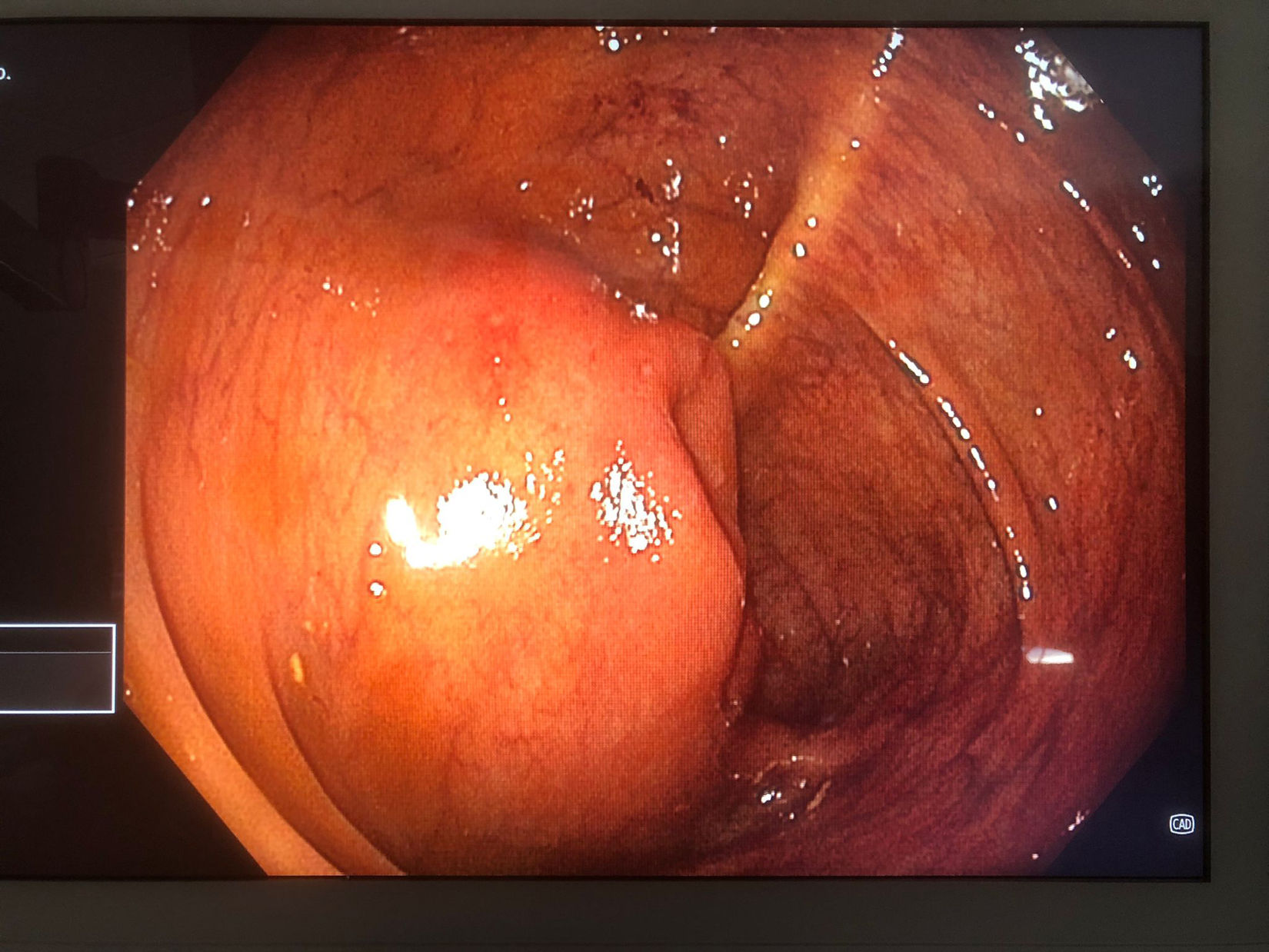

A 31-year-old woman was evaluated in the gastroenterology clinic because of chronic diarrhea. The patient had been in her usual state of good health until 14 months before the current presentation, when non-bloody, watery diarrhea progressively developed up to 8 times during the day, with urgency, no nocturnal symptoms, and no weight loss. She also complained of mild epigastric pain and abdominal bloating. Laboratory evaluation was unremarkable, including stool samples. The SeHCAT test showed excessive bile acid loss (0.06% on day 7). A colonoscopy revealed an augmented ileocecal valve with normal-looking mucosa and normal terminal ileum (Fig. 1). Ileum and colon biopsies were normal. MRI enterography identified a slightly irregular concentric thickening of the walls of the terminal ileum (Fig. 2, arrow), approximately 5.5cm in length from the ileocecal valve. Additionally, a markedly hypointense soft tissue component with spiculated morphology between the uterine body's posterior margin and the rectosigmoid's anterior wall (Fig. 3A and B, arrow), suggestive of endometriotic implant, was observed. A hemorrhagic cystic lesion was observed in the right ovary (Fig. 2C and D, arrowhead), indicative of endometrioma. The patient underwent an ileocecal resection, partial cystectomy, adhesiolysis, and excision of a retrocervical nodule. The pathology report confirmed endometrial implants in surgical specimens. The patient was prescribed cholestyramine but presented oral intolerance, so she was switched to colesevelam pending evaluation of response. Endometriosis is characterized by the presence of endometrial tissue outside the uterine cavity.1 Small bowel involvement is uncommon and typically asymptomatic, unlike our patient, who presented with severe bile acid malabsorption.

, approximately 5.5cm in length from the ileocecal valve, with a maximum wall thickness of 10mm. This results in stenosis of the lumen and retrograde dilation of ileal loops (star), showing significant enhancement after intravenous contrast administration.")
Abdominal MRI enterography: T2 and T1 FS post-contrast coronal sequences. A slightly irregular concentric thickening of the walls of the terminal ileum is identified (arrow), approximately 5.5cm in length from the ileocecal valve, with a maximum wall thickness of 10mm. This results in stenosis of the lumen and retrograde dilation of ileal loops (star), showing significant enhancement after intravenous contrast administration.
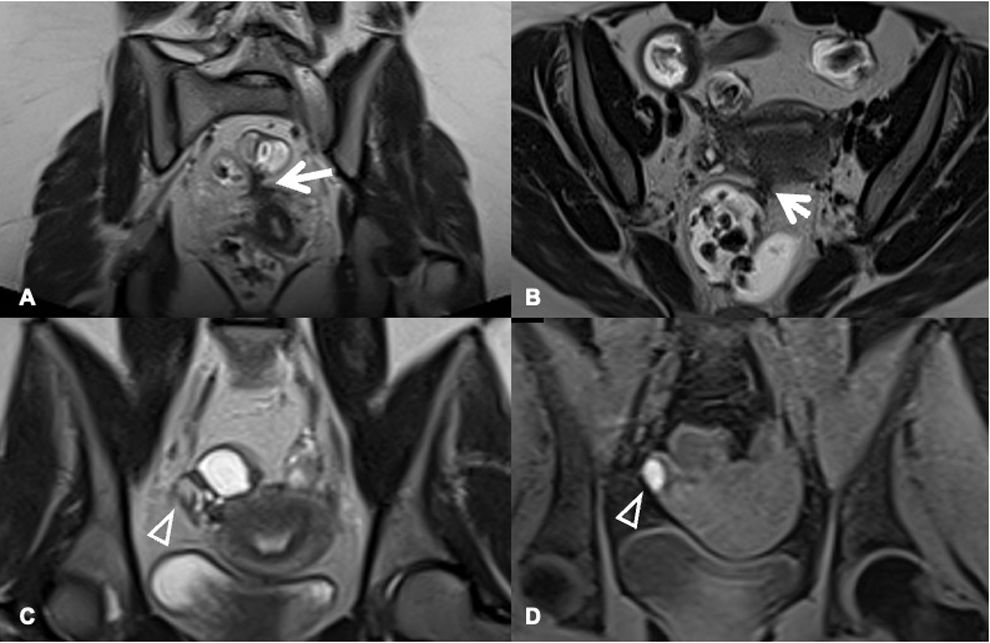
 A markedly hypointense soft tissue component is identified in T2 with spiculated morphology between the posterior margin of the uterine body and the anterior wall of the rectosigmoid (arrow), suggestive of an endometriotic implant. (C and D) A hemorrhagic cystic lesion is observed in the right ovary (arrowhead), indicative of an endometrioma.")
Abdominal MRI enterography: T2 sequences in coronal and axial planes and T1 with fat suppression. (A and B) A markedly hypointense soft tissue component is identified in T2 with spiculated morphology between the posterior margin of the uterine body and the anterior wall of the rectosigmoid (arrow), suggestive of an endometriotic implant. (C and D) A hemorrhagic cystic lesion is observed in the right ovary (arrowhead), indicative of an endometrioma.

