




In November 2019, a new virus appeared, SARS-CoV-2, causing the disease known as COVID-19, which rapidly spread among the world population, in many cases exceeding hospital resources and causing a significant number of deaths.
At the beginning of this pandemic, scientific recommendations were scarce and based mainly on recommendations related to the prevention and treatment of the COVID-19 disease itself. However, emergency surgery for patients with or without COVID-19 infection had to be safeguarded in its entirety by ensuring the protection of patients and professionals.
Surgical teams had to work out their own action protocols based on recommendations from scientific societies, adapting them to that particular setting. With the occurrence of the first case in our hospital, the General Surgery and Digestive System Department developed a series of protocols and protection measures.
Both, a patient circuit in the emergency area1 as well as an independent healthcare circuit for the circulation of suspected patients who required emergency surgery were established. This protocol establishes the steps to be followed by each professional who comes into contact with the infected patient.
Due to the particular considerations of the need for asepsis in the surgical patient, donning and doffing personal protective equipment (PPE) for surgery personnel is complex. A video-tutorial for the training of professionals in donning and doffing of sterile PPE has been prepared. In addition, a check list2 for an assistant to guide and check that the person donning or doffing the surgical PPE performs all the necessary steps to ensure their protection.
In addition to the mentioned measures and the general protection measures, we have introduced two additional protection measures. The first consists of a clinical screening carried out both to patients admitted to the hospital and to their companions by three residents trained for this function. Suspected patients underwent the polymerase chain reaction (PCR) test.
As we did not have a universal screening test available for all asymptomatic patients who had to undergo emergency surgery and clinical screening may not be entirely reliable in patients with urgent surgical pathology, we incorporated a radiological screening3 in these patients through a chest computed tomography (CT). A PCR test was performed in the case of those patients who were suspected through clinical and epidemiological screening and in patients with CT findings.
The COVID-19 infection rate has been analysed in healthcare professionals and patients operated on during the period from 13th March to 24th April 2020. The combination of the protective measures employed has resulted in a low rate of occupational and patient infections. Of the 183 professionals in the Department, only 2 doctors and 2 nurses were infected by SARS-CoV-2 during the analysed period (2.1%). These figures contrast with published data, in which health personnel suffer a high rate of infection4.
The screening team identified 9 suspected cases on the hospital ward. These cases were initially isolated, and after the PCR test for COVID-19, 4 of them were positive (2 patients and 2 relatives).
According to the chest CT detection protocol, 65 preoperative CT scans were performed. Six patients (9.2%) had a test with findings compatible with SARS-CoV-2 infection that were not confirmed by the PCR test.
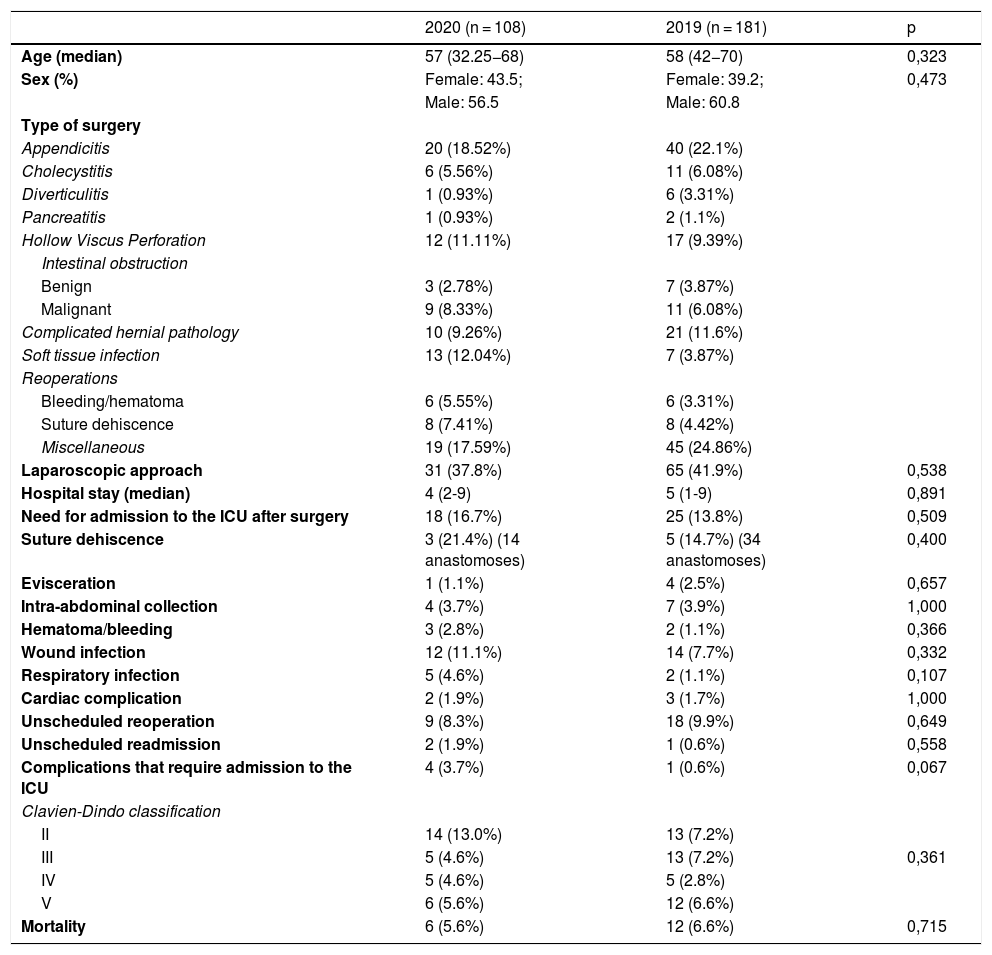
Emergency surgery has shown a significant decrease in the period analysed (181 surgeries with admission in 2019 and 108 in 2020). Despite the increase in morbidity and mortality in surgical patients described in other studies during the pandemic period5, no statistically significant difference has been identified in the morbidity and mortality of our patients when comparing both periods (Table 1Table 1).
Demographic characteristics and clinical results in each period.
| 2020 (n = 108) | 2019 (n = 181) | p | |
|---|---|---|---|
| Age (median) | 57 (32.25−68) | 58 (42−70) | 0,323 |
| Sex (%) | Female: 43.5; | Female: 39.2; | 0,473 |
| Male: 56.5 | Male: 60.8 | ||
| Type of surgery | |||
| Appendicitis | 20 (18.52%) | 40 (22.1%) | |
| Cholecystitis | 6 (5.56%) | 11 (6.08%) | |
| Diverticulitis | 1 (0.93%) | 6 (3.31%) | |
| Pancreatitis | 1 (0.93%) | 2 (1.1%) | |
| Hollow Viscus Perforation | 12 (11.11%) | 17 (9.39%) | |
| Intestinal obstruction | |||
| Benign | 3 (2.78%) | 7 (3.87%) | |
| Malignant | 9 (8.33%) | 11 (6.08%) | |
| Complicated hernial pathology | 10 (9.26%) | 21 (11.6%) | |
| Soft tissue infection | 13 (12.04%) | 7 (3.87%) | |
| Reoperations | |||
| Bleeding/hematoma | 6 (5.55%) | 6 (3.31%) | |
| Suture dehiscence | 8 (7.41%) | 8 (4.42%) | |
| Miscellaneous | 19 (17.59%) | 45 (24.86%) | |
| Laparoscopic approach | 31 (37.8%) | 65 (41.9%) | 0,538 |
| Hospital stay (median) | 4 (2-9) | 5 (1-9) | 0,891 |
| Need for admission to the ICU after surgery | 18 (16.7%) | 25 (13.8%) | 0,509 |
| Suture dehiscence | 3 (21.4%) (14 anastomoses) | 5 (14.7%) (34 anastomoses) | 0,400 |
| Evisceration | 1 (1.1%) | 4 (2.5%) | 0,657 |
| Intra-abdominal collection | 4 (3.7%) | 7 (3.9%) | 1,000 |
| Hematoma/bleeding | 3 (2.8%) | 2 (1.1%) | 0,366 |
| Wound infection | 12 (11.1%) | 14 (7.7%) | 0,332 |
| Respiratory infection | 5 (4.6%) | 2 (1.1%) | 0,107 |
| Cardiac complication | 2 (1.9%) | 3 (1.7%) | 1,000 |
| Unscheduled reoperation | 9 (8.3%) | 18 (9.9%) | 0,649 |
| Unscheduled readmission | 2 (1.9%) | 1 (0.6%) | 0,558 |
| Complications that require admission to the ICU | 4 (3.7%) | 1 (0.6%) | 0,067 |
| Clavien-Dindo classification | |||
| II | 14 (13.0%) | 13 (7.2%) | |
| III | 5 (4.6%) | 13 (7.2%) | 0,361 |
| IV | 5 (4.6%) | 5 (2.8%) | |
| V | 6 (5.6%) | 12 (6.6%) | |
| Mortality | 6 (5.6%) | 12 (6.6%) | 0,715 |
During the pandemic, when all efforts are focused on the treatment and control of infected patients, we cannot forget that there are patients who will require our assistance without delay.
An early response by developing clear protocols for the care of emergency surgery patients in the period of the COVID-19 pandemic has been essential to achieve a low rate of contagion between professionals and patients treated.
Please cite this article as: Durán-Muñoz-Cruzado VM, Pareja-Ciuró F, Padillo-Ruiz J. Análisis de los resultados en seguridad de pacientes y profesionales durante la pandemia COVID-19 en el contexto de la cirugía urgente. Med Clin (Barc). 2020;156:34–35.
