




Información del artículo
Texto completo
Bibliografía
Descargar PDF
Estadísticas
Tablas (1)
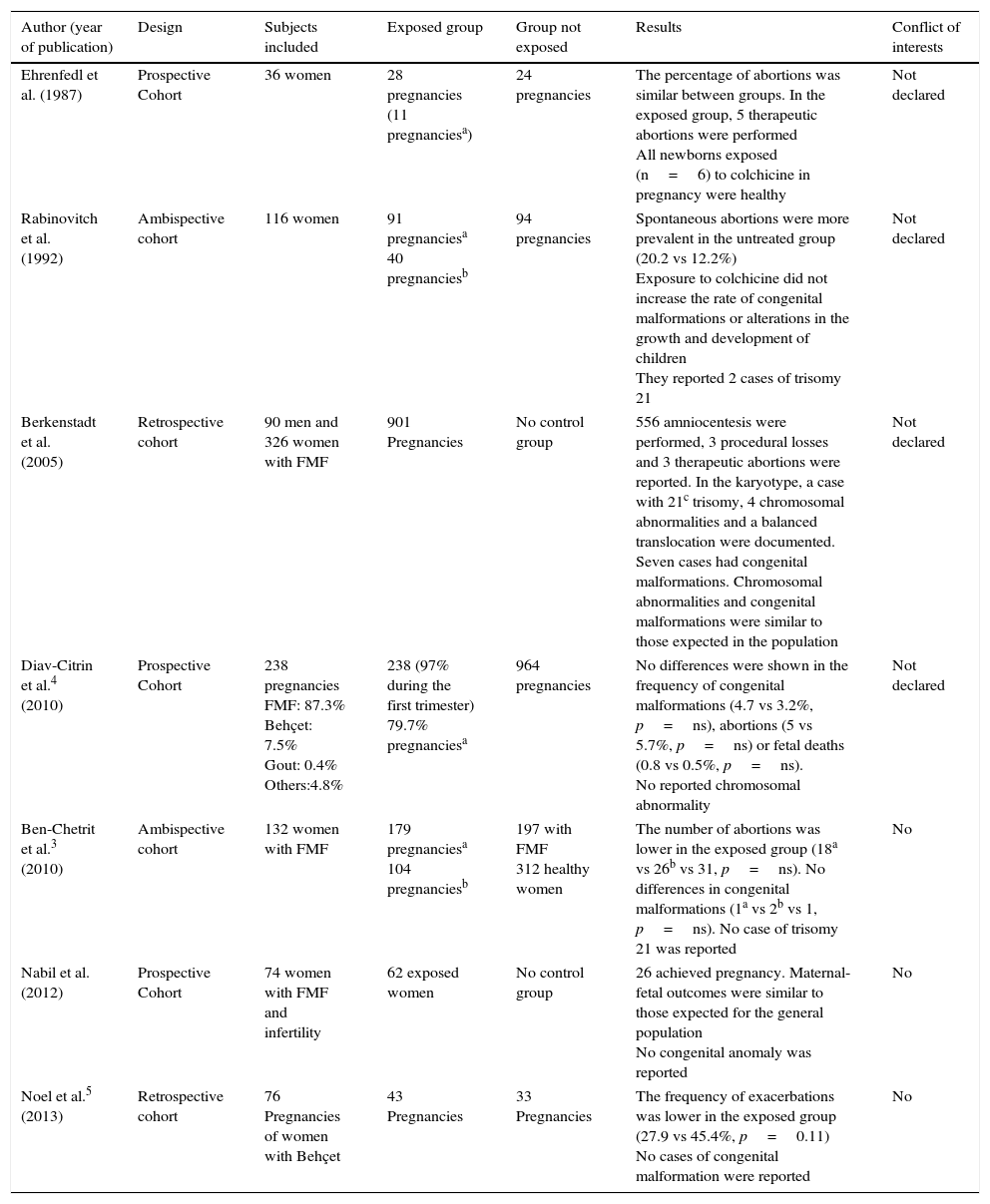
Table 1. Summary of studies assessing colchicine exposure during pregnancy in women with familial Mediterranean fever and Behçet's disease.
Artículo
Opciones para acceder a los textos completos de la publicación Medicina Clínica (English Edition)
Suscriptor
Suscribirse

Comprar
Comprar acceso al artículo
Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora
Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora
Contactar
Teléfono para suscripciones e incidencias
De lunes a viernes de 9h a 18h (GMT+1) excepto los meses de julio y agosto que será de 9 a 15h
Llamadas desde España
932 415 960
Llamadas desde fuera de España
+34 932 415 960
E-mail
