




To reach the diagnosis of giant cell arteritis (GCA), signs, symptoms, laboratory tests, imaging findings, and occasionally anatomopathological results from temporal artery biopsy are evaluated. This study describes the results of an algorithm analysis based on clinical and ultrasound evaluation of patients with suspected GCA, highlighting its diagnostic utility by contrasting its use in different clinical suspicion scenarios.
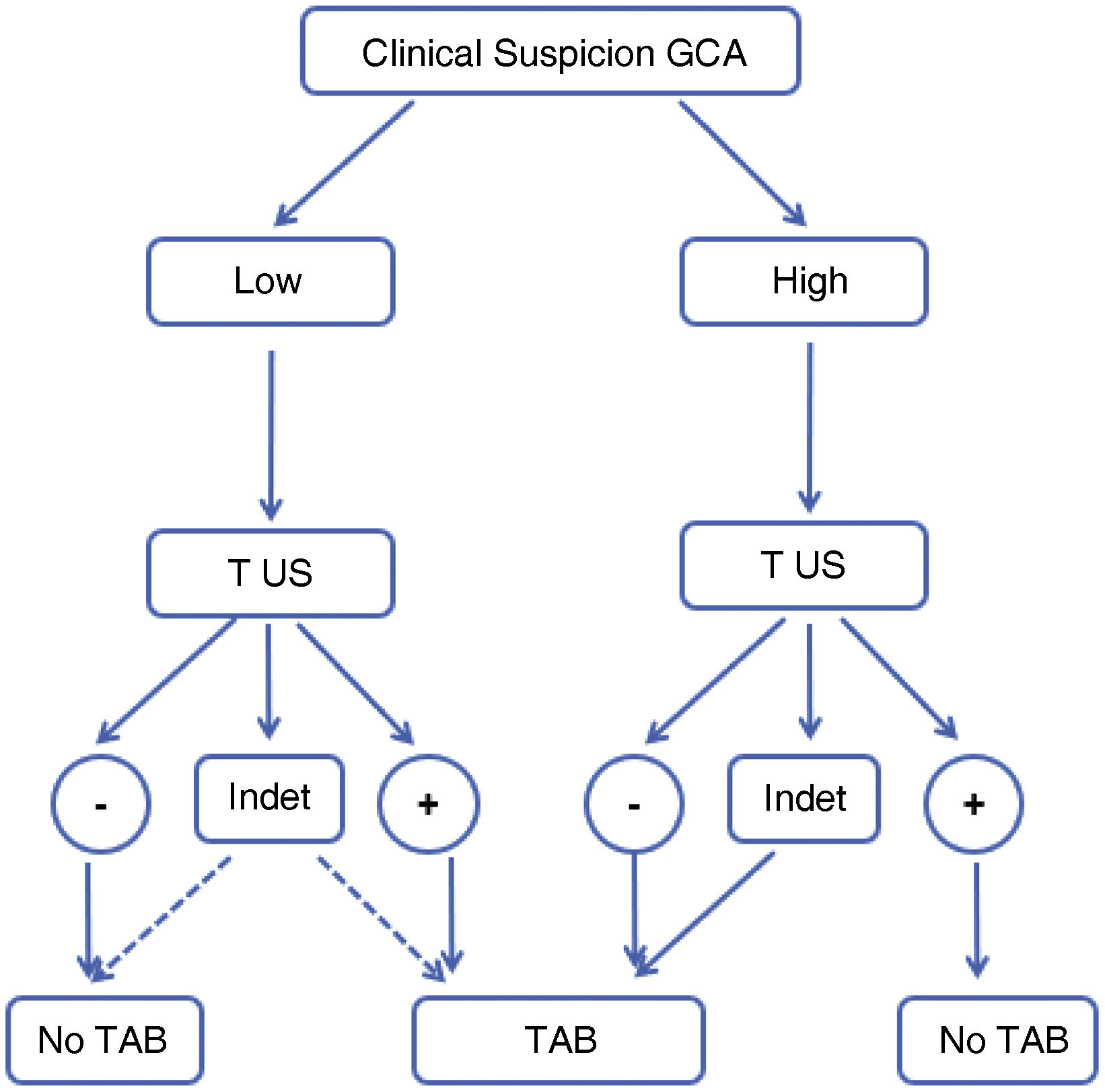
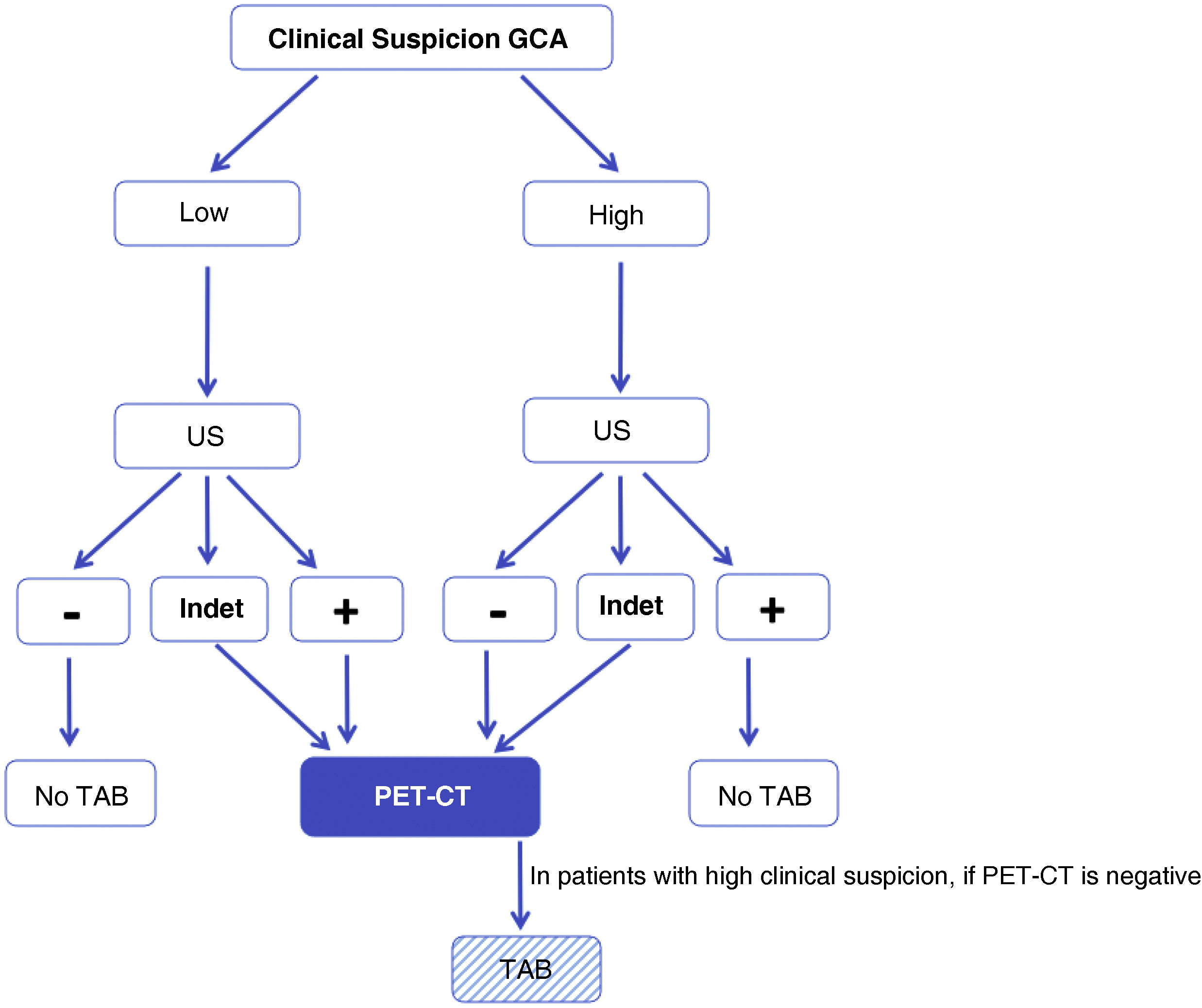
MethodProspective multicenter study evaluating patients referred with suspected GCA through a preferential circuit (fast track), grouping them according to low or high clinical suspicion of GCA. Each of these scenarios is evaluated by biopsy and ultrasound for all patients, resulting in positive, indeterminate, or negative outcomes, yielding six possible groups. Potential areas of improvement are explored, emphasizing that, following a negative or indeterminate ultrasound, 18-FDG-PET-CT could be recommended. We analyze the results and application of a diagnostic algorithm, confirming its efficiency and applicability based on whether there is high or low clinical suspicion.
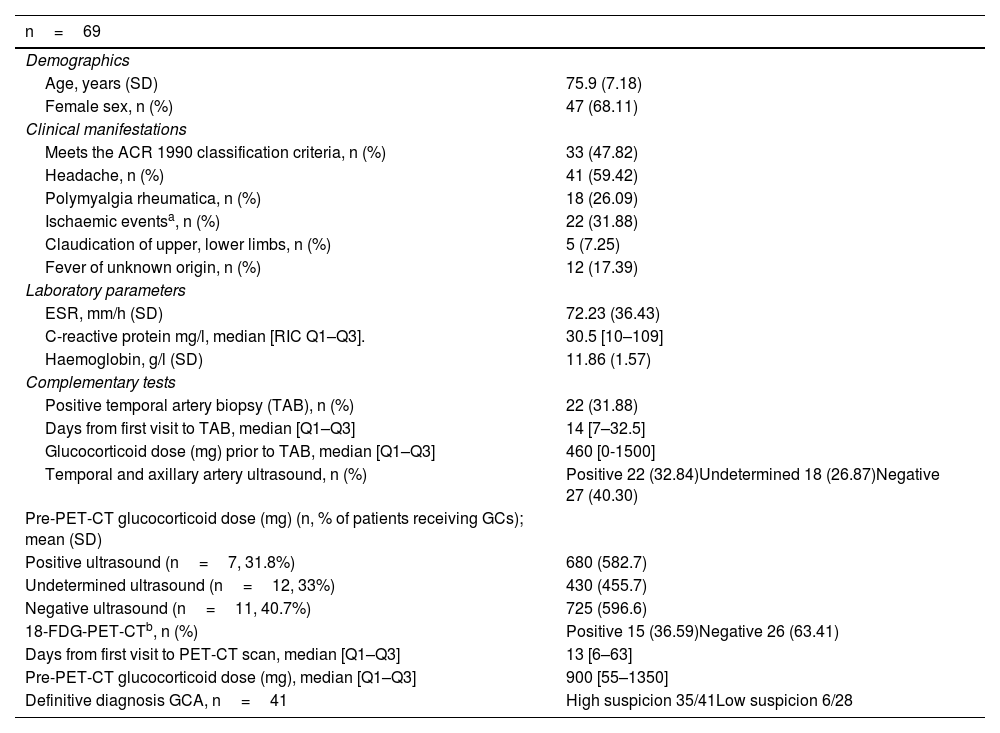
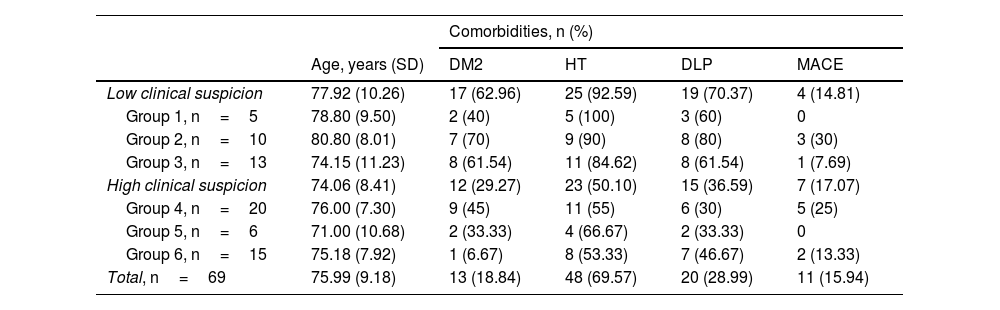
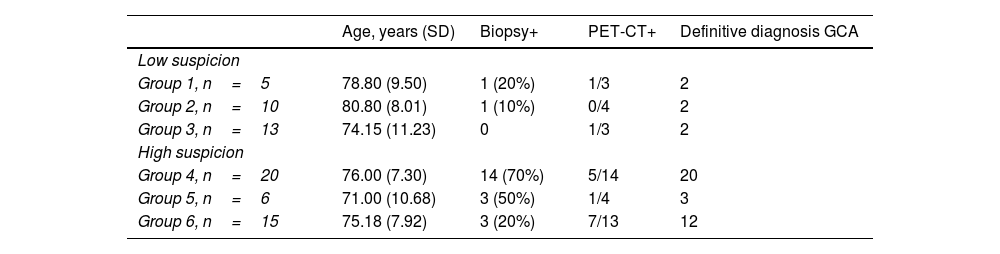
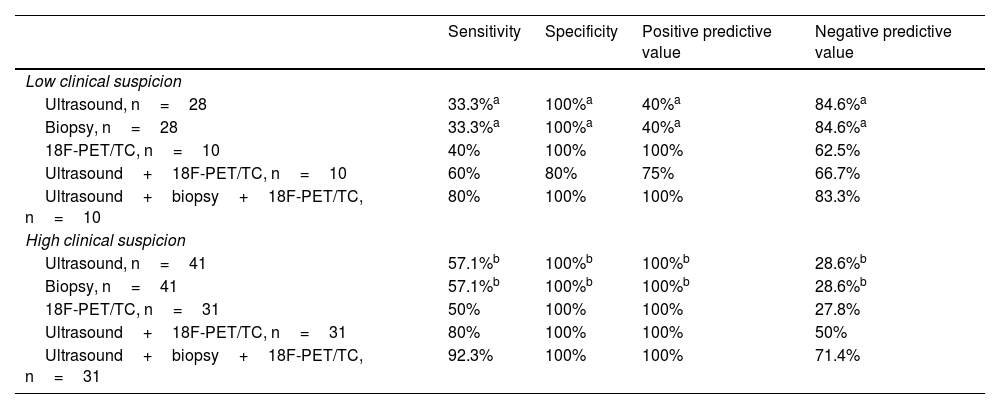
ResultsSixty-nine patients (41 in the high suspicion group and 28 in the low suspicion group). There were 41 new diagnoses of GCA, 35 in the high suspicion group and 6 in the low suspicion group. Using ultrasound alone, the initial algorithm has an overall diagnostic efficiency of 72.5%, which improves to 80.5% when including 18F-FDG-PET/CT. The negative predictive value of ultrasound in patients with low clinical suspicion is 84.6%, and the positive predictive value of ultrasound in patients with high suspicion is 100%, improving sensitivity from 57.1% to 80.8% with 18F-FDG-PET/CT in this scenario. Temporal artery biopsy was performed on all patients, with no differences in sensitivity or specificity compared to ultrasound. In cases where all three tests—ultrasound, biopsy, and 18F-FDG-PET/CT—are performed, sensitivity increases to 92.3% in patients with high clinical suspicion.
ConclusionIn situations of high clinical suspicion, the algorithm provides sufficient information for the diagnosis of GCA if ultrasound is positive. A negative ultrasound is sufficient to rule out the diagnosis in the context of low clinical suspicion. 18-FDG-PET-CT may be useful in patients with high suspicion and negative or indeterminate ultrasound results.
Para llegar al diagnóstico de ACG, se evalúan signos, síntomas, pruebas de laboratorio, hallazgos de pruebas de imagen y en ocasiones los resultados anatomopatológicos de la BAT. El presente estudio describe los resultados del análisis de un algoritmo basado en la clínica y ecografía de los pacientes con sospecha de ACG, destacando su utilidad diagnóstica, al contrastar su utilización en diferentes escenarios de sospecha clínica.
MétodoEstudio prospectivo multicéntrico que evalúa mediante un circuito preferente (fast track) a los pacientes derivados con sospecha de ACG, para la realización de una ecografía de arterias temporales y axilares, agrupándose según: baja o alta sospecha clínica de ACG. Cada uno de estos supuestos es evaluado por ecografía, el resultado puede ser positiva, indeterminada o negativa, obteniendo 6 posibles grupos diferentes. Se exploran las posibles áreas de mejora, tras una ecografía negativa o indeterminada. En algunos pacientes se realiza un 18F-FDG-PET/TC. Analizamos los resultados y la aplicación de un algoritmo diagnóstico, confirmando su eficiencia y su aplicabilidad en según si hay una alta o baja sospecha clínica.
ResultadosSesenta y nueve pacientes (41 en el grupo de alta sospecha y 28 en el de baja sospecha clínica). Hubo un total de 41 diagnósticos nuevos de ACG, 35 en el grupo de alta sospecha y 6 en el de baja sospecha. El algoritmo inicial tiene una eficiencia global de diagnóstico de 72,5%, si solamente se utiliza la ecografía, que al incluir al 18F_FDG-PET/TC, mejora a 80,5%. El valor predictivo negativo de la ecografía en los pacientes que presentan una baja sospecha clínica es del 84,6% y el valor predictivo positivo de la ecografía en los pacientes con una sospecha alta es del 100%, mejorando en este escenario la sensibilidad del 57,1% a 80,8% si hacemos un 18F-FDG-PET/TC. La BAT, se realizó a todos los pacientes, sin encontrar diferencias en la sensiblidad o especificidad respecto a la ecografía. En el caso de tener las tres pruebas realizadas, ecografía, biopsia y 18F-FDG-PET/TC, la sensibilidad aumenta a 92,3% en los pacientes que presentan una alta sospecha clínica.
ConclusiónEn situaciones de alta sospecha clínica, el algoritmo proporciona suficiente información para el diagnóstico de ACG si la ecografía es positiva. En el contexto de baja sospecha clínica, una ecografía negativa es suficiente para descartar el diagnóstico. El 18-FDG-PET-TC puede ser de utilidad en aquellos pacientes con alta sospecha y ecografía negativa o indeterminada.

