



High levels of glutamate decarboxylase enzyme (anti-GAD) are frequently detected in stiff person syndrome (SPS), and they have also been reported more recently in a group of patients with cerebellar ataxia.1,2 As these syndromes are probably of autoimmune origin, several immunomodulatory regimens have been employed, and these treatments have yielded variable results.3–5 However, there are no studies describing long-term outcomes for these patients.
We describe the initial clinical response and long-term outcome after immunomodulatory treatment in 2 patients with cerebellar ataxia with anti-GAD antibodies. We also present a third case with long-standing SPS and cerebellar ataxia associated with anti-GAD antibodies and describe how the 2 clinical manifestations responded differently to treatment.
Case 1We present the case of a 75-year-old woman with a history of Graves disease and diabetes mellitus type 1 (DM1). At the age of 60, she began to experience symptoms of instability, dysarthria, and nystagmus which progressed for several months. Brain MRI study showed mild cerebellar atrophy. Anti-GAD antibody titres in serum were measured by radioimmunoassay, which yielded a level of 39500U/mL; CSF analysis revealed positive oligoclonal bands (OCB). The patient was treated with intravenous immunoglobulins (IVIG) dosed at 0.4g/kg/day for 5 days, and symptoms improved slightly. Treatment with IVIG has since been administered every 3-4 months, and the patient's condition remains stable to date. This case report has already been published.6
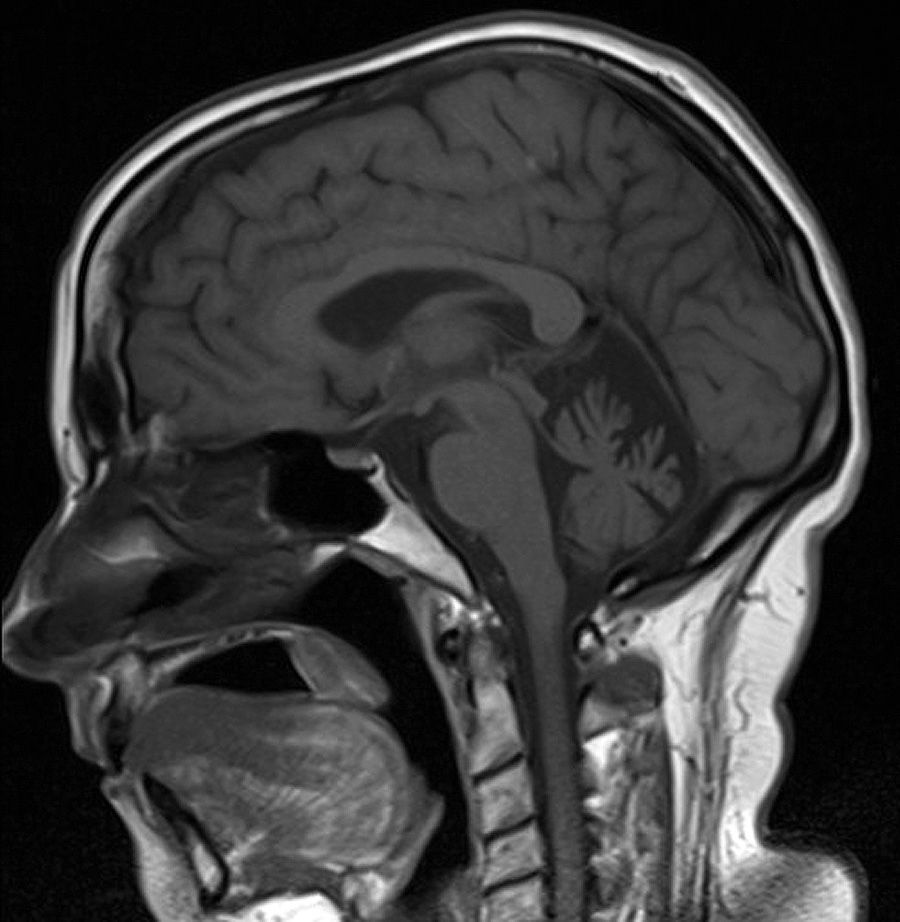
Case 2The second case is a 55-year-old woman with no relevant personal history who developed pancerebellar syndrome at the age of 50. At the same time, she was diagnosed with DM. The brain MRI study revealed atrophy of the cerebellar vermis (Fig. 1). Anti-GAD antibody titres in serum were measured by radioimmunoassay, which yielded a level of 23000U/mL.7 The patient was treated with methylprednisolone (1000mg/day for 5 days), and clinical symptoms improved somewhat. Since that phase, she has been treated with prednisone (2.5mg/day) and azatiopirine (50mg/day) and no symptom progression has been observed.
Case 3
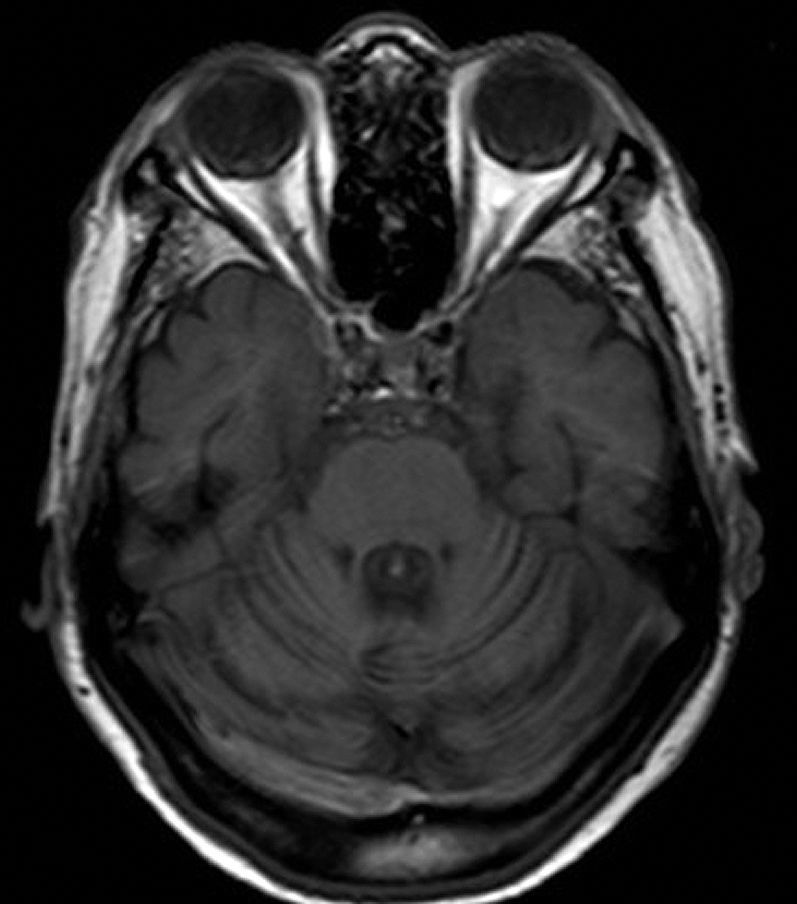
Woman aged 65 years with a history of exophthalmos secondary to prior Graves disease. At the age of 50, she began experiencing symptoms of leg rigidity and spasms. At the age of 52, she underwent an examination in another centre, which revealed scanning dysarthria, limb ataxia, generalised hyperreflexia, and increased tone of the lower limbs. She was attended for the first time at our hospital at the age of 65, and we observed exacerbated symptoms, including inability to remain standing without help. Anti-GAD antibody titres in serum and CSF were 0.99 and 0.97 respectively (in this case we used another technique whose reference value is <0.027); CSF was OCB-negative. At the same time, she was diagnosed with pernicious anaemia, and levels of vitamin B12 were corrected with intramuscular vitamin supplementation. Brain MRI study revealed overall cerebellar atrophy (Fig. 2). The patient was treated with IVIG (0.4g/kg/day for 5 days), which improved leg spasms and rigidity, but the cerebellar syndrome displayed no changes.8 The video provided as additional online material shows the following: pretreatment (0 to 45seconds): (1) upper-limb dysmetria, more severe on the right side, and dysdiadochokinesia, (2) generalised hyperreflexia and increased tone of the lower limbs, especially the right leg, and (3) pronounced rigidity of the legs, and difficulty walking; post-treatment (46 to 90seconds): (1) dysmetria and dysdiadochokinesia, which remains unaltered, (2) decreased tone of the legs, and (3) decreased rigidity of the legs during walking with improved ability to take steps. Cerebellar ataxia, however, remains unchanged.

Nevertheless, other authors have reported a good response to immunological therapy.9 It seems reasonable to think that treatment may be effective when administered early, before irreversible neuronal loss has occurred.10 Therefore, early diagnosis and treatment of patients with cerebellar ataxia with anti-GAD antibodies are essential.
Although it is difficult to make a long-term forecast due to the spontaneous and fluctuating course of the disease, long-term immunomodulatory treatment could help stabilise the patient's condition. Further studies are needed to establish the most appropriate strategies for both initial and long term treatment.
Please cite this article as: Rouco I, Hurtado P, Castaño L, Zarranz JJ. Experiencia en el tratamiento con inmunoterapia en 3 pacientes con ataxia cerebelosa asociada a anticuerpos anticarboxilasa del ácido glutámico. Neurología. 2015;30:247–249.
