



Massive pulmonary thromboembolism is a condition with high morbidity and mortality if not treated early. A case of a young man with a history of knee trauma that was admitted to the emergency department with sudden dyspnea and syncope is discussed. During the clinical evaluation the patient experienced 5 episodes of cardiac arrest that required prolonged cardiopulmonary-cerebral resuscitation. The diagnosis of massive pulmonary thromboembolism was confirmed by echocardiography and thoracic CT angiography. Although prolonged cardiopulmonary-cerebral resuscitation is a relative contraindication for systemic thrombolysis, the patient experienced remarkable clinical improvement with no sequelae upon hospital discharge.
El tromboembolismo pulmonar masivo es una entidad con alta morbilidad y mortalidad si no se trata tempranamente. Se expone el caso de un hombre joven con antecedente de trauma en rodilla quien ingresa al servicio de urgencias por cuadro súbito de disnea y síncope; durante la evaluación clínica presenta 5 episodios de paro cardiaco con requerimiento de reanimación cardiocerebropulmonar prolongada; se confirma el diagnóstico de tromboembolismo pulmonar masivo mediante ecocardiografía y angiotac de tórax. A pesar que la reanimación cardiocerebropulmonar prolongada se considera una contraindicación relativa para trombolisis sistémica, ésta fue administrada, con notoria mejoría clínica, sin ninguna secuela al alta hospitalaria.
Pulmonary thromboembolism (PTE) is defined as a partial or complete obstruction of the pulmonary artery or any of its branches potentially resulting in acute right ventricular insufficiency and cardiogenic shock. Around 90–95% of the emboli originate from the venous system of the lower extremities.1–3
The estimated incidence of PTE is 70–200 cases per 100,000 inhabitants per year,2,4,5 and it has a strong direct correlation with age.6,7
In many cases PTE is asymptomatic or has a non-specific clinical evolution and is only identified in about 60% of the cases.8,9 Some studies suggest that up to 60% of all hospitalized patients may have PTE, representing the primary cause of preventable deaths in this type of patients.1 PTE is the third cause of cardiovascular death, following myocardial infarction and cerebrovascular disease.10 The overall hospital mortality due to PTE in Colombia is approximately 14.8%. Proper management may reduce this rate from 15–30% down to 3–10%.11,12 30% of the patients that survive an acute episode of PTE will experience residual symptoms and 2% develop pulmonary hypertension.13
The clinical guidelines suggest classifying the patient into four categories for the diagnostic and therapeutic approach13,14:
High risk: patients with PTE severity index (PESI) Class III–V (massive PTE), severe right ventricle (RV) dysfunction, elevated cardiac biomarkers, hypotension, cardiogenic shock or respiratory arrest.
Intermediate high risk: patients with PESI Class III–V, RV dysfunction, elevated cardiac biomarkers with no hypotension or shock.
Intermediate low risk: patients with PESI Class III–V, RV dysfunction or elevated cardiac biomarkers or none of the above.
Low risk: patients with PESI Class I–II, minor symptoms such as chest pain and tachycardia produced by small clots in the distal pulmonary circulation, with no signs of RV dysfunction or elevation of cardiac biomarkers.13,14
The therapeutic options for PTE management include systemic anticoagulation, systemic thrombolysis, catheter-directed thrombolysis (CDT) and surgical thrombectomy.15
Systemic thrombolysis reduces the mortality in high-risk patients16,17 and may be considered for intermediate-high risk patients14; its principal benefit is based on the quick recovery of the pulmonary blood flow, but it is associated with major bleeding complications in up to 20% of the cases, and with intracranial hemorrhage with an incidence of 0.9–5%.16,18
In high-risk PTE patients and with absolute or relative contraindications for systemic thrombolysis,14 the guidelines specify that systemic thrombolysis could be considered in the presence of immediate life-threatening risk. Furthermore, alternative therapies have been proposed in the literature, including CDT and surgical thrombectomy that should be performed at specialized institutions.15
Upon approval by the institution's ethics committee and by the patient, a clinical case of a young man admitted to the emergency department with high-risk PTE is discussed. The patient presented with cardiorespiratory arrest on 5 occasions, requiring prolonged CPCR and finally undergoes systemic thrombolysis with satisfactory results and with no pulmonary or neurological sequelae. The article is proprietary of the authors.
Clinical case description29-year old man, mestizo, biologist, with no relevant personal or family history, healthy life-style, who 15 days prior to admission developed a lesion in the right knee meniscus while practicing sports but did not require surgical management. While receiving physical therapy the patient presented three seizure episodes followed by syncope. The patient was admitted fully conscious to the emergency department complaining of chest pain and dyspnea. During the first hour the patient developed 5 episodes of cardiac arrest, one of them lasted for 20min, documenting pulseless electrical activity (PEA). CPCR maneuvers were implemented and spontaneous circulation in sinus tachycardia was restored.
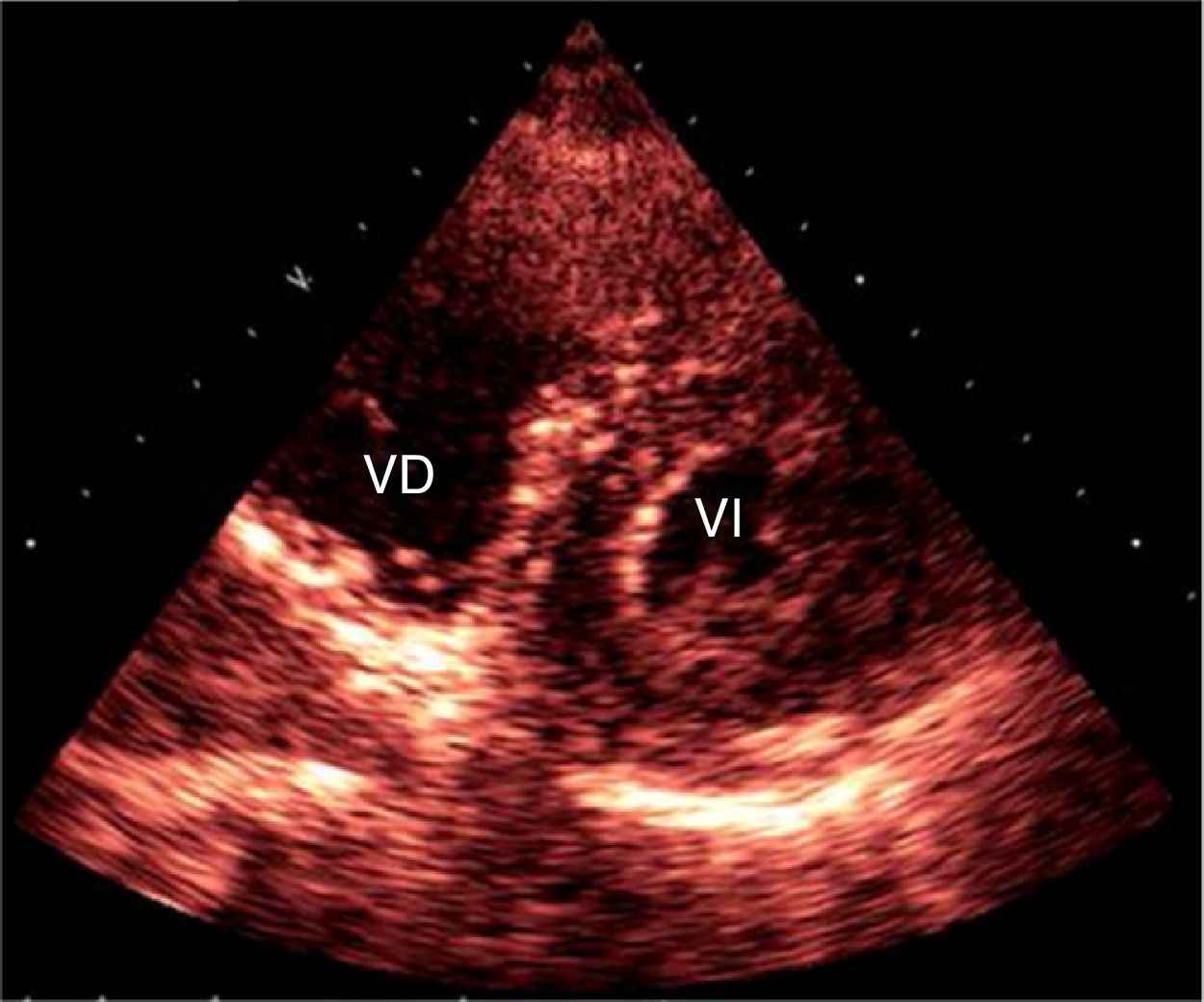
There were no economic, cultural or linguistic barriers for the diagnostic approach. A transthoracic ECG evidenced a moderately dilated right ventricle with free wall hypokinesis (TAPSE 9.2mm), a systolic pulmonary pressure of 55mmHg, moderately dilated pulmonary artery and hyper-dynamic left ventricle (Fig. 1).

The patient was transferred to Intensive Care with invasive ventilation support and noradrenalin infusion at 0.1mcg/k/min and vasopressin at 0.01μ/min. A chest CT angiography was positive for massive pulmonary thromboembolism involving both lower lobes and the left upper lobe associated with signs of severe pulmonary hypertension (Fig. 2).

Within the clinical context of a patient with high-risk PTE, prolonged CPCR, and elevated risk for hemorrhagic complications with the administration of systemic thrombolysis, a CDT is initially suggested. However, the Cat-Lab was not available at that time and the patient's conditions were not adequate for transfer. A doctor's meeting was convened and considering the impending life-threatening high risk for the patient, the decision was to administer systemic thrombolysis. Upon obtaining the patient's informed consent, thrombolysis therapy with 100mg of tissue plasminogen activator (Alteplase) was initiated, which was well tolerated, with no evidence of major bleeding. Cerebral hemorrhage was ruled out with neuroimaging and protective hypothermia was initiated. There was a remarkable hemodynamic improvement in the following 12h and vasopressor requirements decreased.
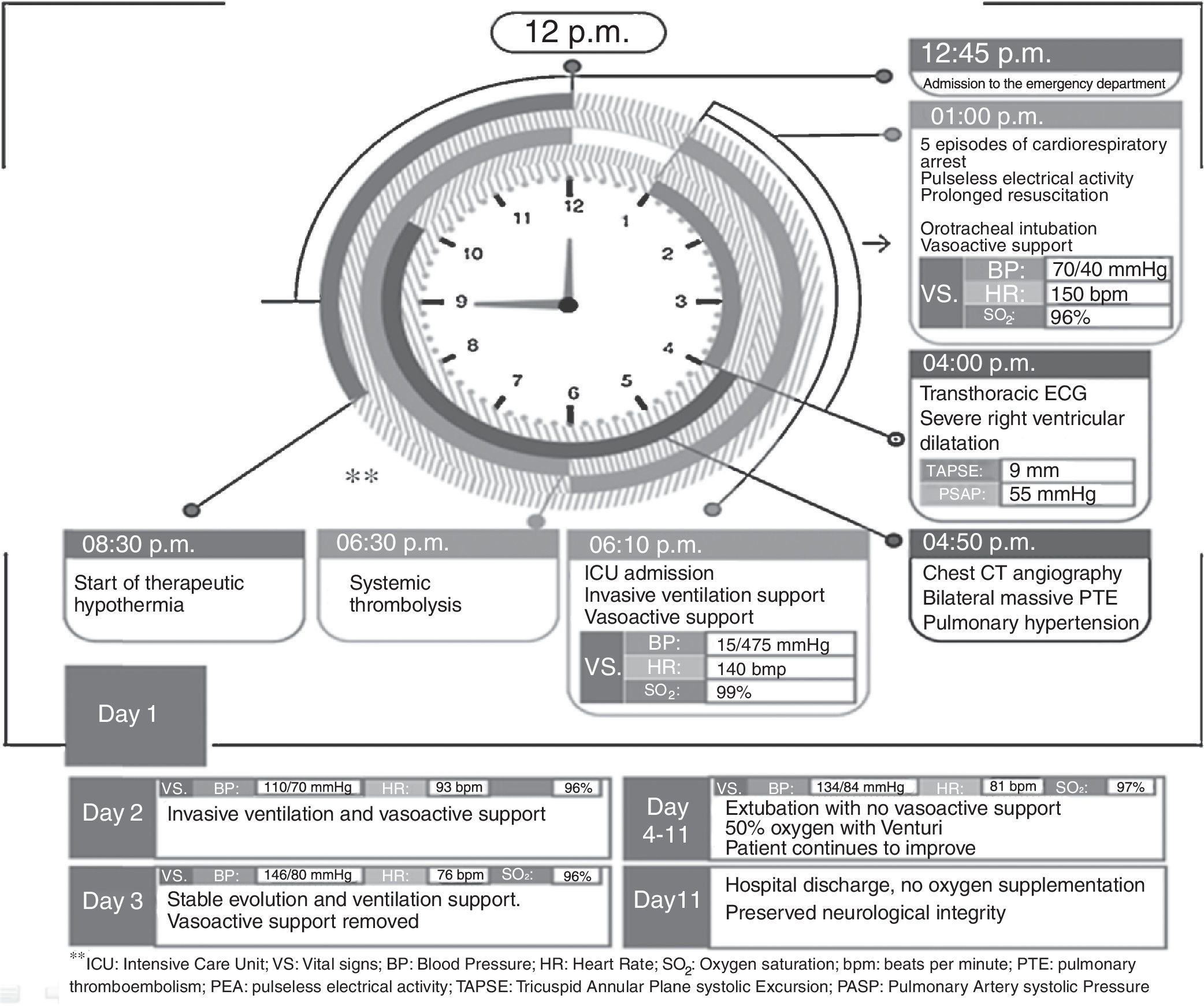
A Doppler study confirmed the presence of deep vein thrombosis of the popliteal and posterior tibial veins, in addition to the soleal venous plexus of the right lower extremity. Ventilation support and vasopressors were removed after 48h. The patient was discharged 10 days later with no neurological sequelae and no supplemental oxygen, with oral anticoagulation and was referred for blood tests to rule out thrombophilia. Fig. 3 illustrates a summary of the patient's key events.
Discussion
In patients with high risk PTE and an extremely critical condition to perform chest CT angiography, the ECG at the patient's bedside may help in identifying any signs suggestive of PTE.19 If PTE is a known or suspected cause of cardiac arrest, thrombolysis may help to recover spontaneous circulation and ensure high survival rates.20 However, in the particular case under discussion, an ultrasound machine was not available to quickly guide the diagnosis; since the administration of thrombolytic agents to patients in cardiac arrest of undifferentiated causes is not associated with a significant benefit in terms of mortality,21 the decision adopted was to stabilize the patient's hemodynamic condition while confirmatory tests could be performed.
Notwithstanding the relative contraindication of prolonged CPCR for the administration of systemic thrombolysis, once PTE is diagnosed in a patient at life-threatening risk, and in the absence of a CatLab for CDT, the decision was to administer Alteplase, with remarkable clinical improvement and no sequelae at discharge.
In conclusion, systemic thrombolytic agents are not considered a contraindication under a life-threatening PTE situation. ECG at the patient's bedside may help to guide the diagnosis and provide quick management response in these cases.
FundingThe authors did not receive sponsorship to undertake this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Chicangana G, Zapata L, Gómez JC, Zuluaga JP. Trombolisis sistémica exitosa en un paciente con tromboembolismo pulmonar masivo, luego de reanimación cardiocerebropulmonar prolongada. Informe de caso. Rev Colomb Anestesiol. 2016;44:245–248.