





Tillaux fracture is known to occur in adolescents once it happens during transition period when the medial and central physis has finished closure, but the lateral physis is still opened. The trauma mechanism is typically external rotation ankle injury resulting in an avulsion fracture of the anterolateral tibial plafond. This fracture has rarely been reported in adults, especially associated with others injuries. We report a case of Tillaux fracture in an adult, associated with a Volkmann fracture and a Maisonneuve fracture, that were surgery treated with open reduction and internal fixation and had an excellent outcome. Recognize and appropriately treat each one of these injuries is the key to prevent further degenerative arthritis and instability.
Evidence Level: IV
Se sabe que la fractura de Tillaux ocurre en adolescentes una vez que ocurre durante el período de transición cuando la fisis medial y central ha finalizado el cierre, pero la fisis lateral todavía está abierta. El mecanismo de traumatismo es típicamente una lesión de tobillo de rotación externa que resulta en una fractura por avulsión del plafón tibial anterolateral. Esta fractura rara vez se ha informado en adultos, especialmente asociada con otras lesiones. Divulgamos un caso de fractura de Tillaux en un adulto, asociado con una fractura de Volkmann y una fractura de Maisonneuve, que se trataron mediante cirugía con reducción abierta y fijación interna y tuvieron un resultado excelente. Reconocer y tratar apropiadamente cada una de estas lesiones es la clave para prevenir artritis e inestabilidad degenerativas.
Nivel de Evidencia: IV
Tillaux fracture is an avulsion fracture of the anterolateral aspect of the tibial plafond owing to the pull of a taut anteroinferior tibiofibular ligament (AITL). In adults, differ from children, the ligament generally gives away before avulsion of its attachment to the anterolateral tibial plafond occurs, leading to relative rarity of this avulsion pattern.1–4 The mechanism of this fracture is typically supination with external rotation.5 In children, the size of the fracture depends on the extent of the fusion medially, because distal tibial epiphyseal closure has an asymmetric pattern. Physeal closure starts from the center and then progresses toward the medial side. Finally, the lateral aspect of distal tibial fusion occurs. The medial closure occurs at approximately 13 to 14 years of age, with lateral closure beginning at 14.5 to 16 years of age. The interval (∼18 months) during which the distal tibial physis completes its closure and gains maturity is referred to as “transition period”. Adolescent Tillaux fracture occurs during transition period when the medial and central physis has finished closure, but the lateral physis still open.6
Volkmann fracture generally occurs in ankle fracture due to either mechanism of pronation or supination with external rotation. External rotation forces make the talus rotate further laterally and the posteroinferior tibiofibular ligament (PITFL) stretch, thus either the PITFL will rupture or an avulsion fracture from the posterolateral tibia occur.
Maisonneuve fracture is an injury caused by a pronation-external rotation force at the ankle that results in rupture along the syndesmosis with its diastasis, lateral talar shift and spiral fracture of the proximal half of the fibula.7
Tillaux fractures have rarely been reported in adults. Of the six published case reports in patients over 18 years old, only one had Tillaux fracture associated with Volkmann fracture, and none of them had association with Maisonneuve fracture.In the present report, we describe the case of a Tillaux fracture in an adult, associates with a Volkmann and a Maisonneuve fractures. To the best of our knowledge, no data are available regarding the association of all of these lesions.
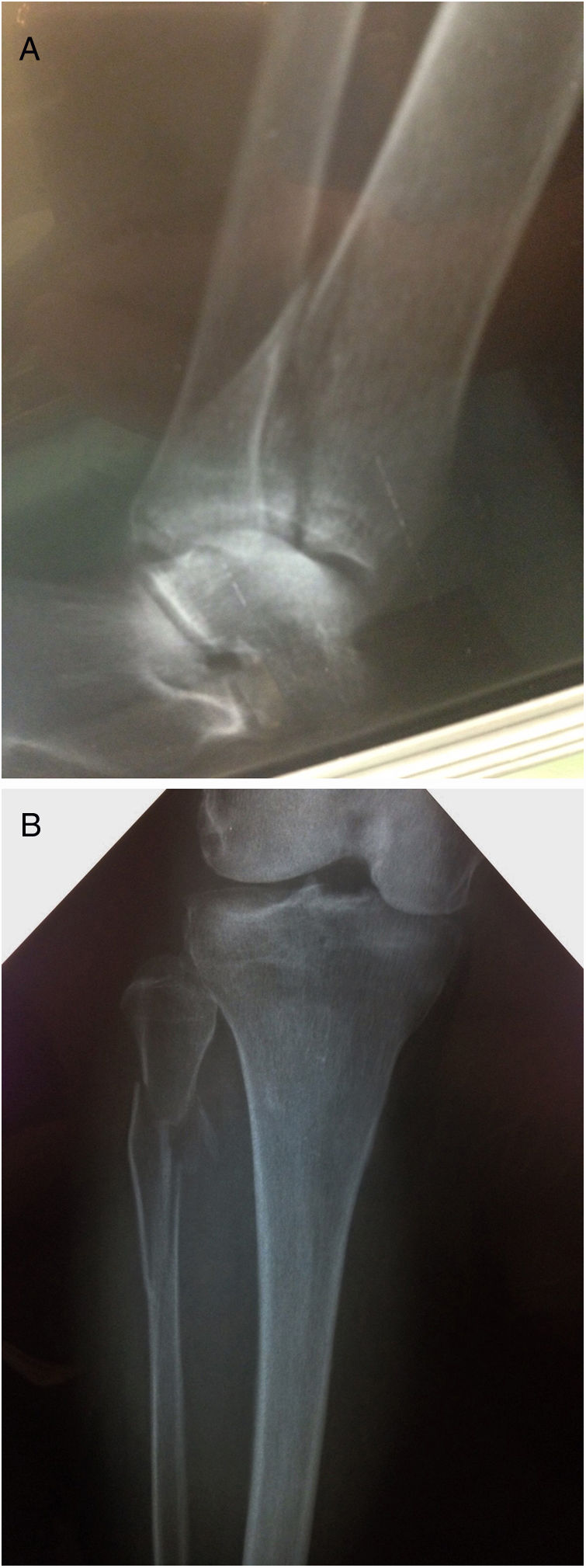
Case ReportA 74-year-old female presented to the emergency room after been hit by a car. The patient was unable to bear weight on her left lower extremity. On clinical examination, swelling and significant tenderness was present over the proximal extremity of her leg until her ankle. The neurovascular examination was normal. Radiographs showed spiral fracture of the proximal half of the fibula (Maisonneuve) (Figure 1A) and posterior malleolus fracture (Volkmann fragment) (Figure 1B). The CT Scan revealed fracture of the anterolateral aspect of the tibial plafond (Tillaux-Chaput) (Figure 2). The patient also had an ischiopubian branch, without displacement.
Surgical Technique

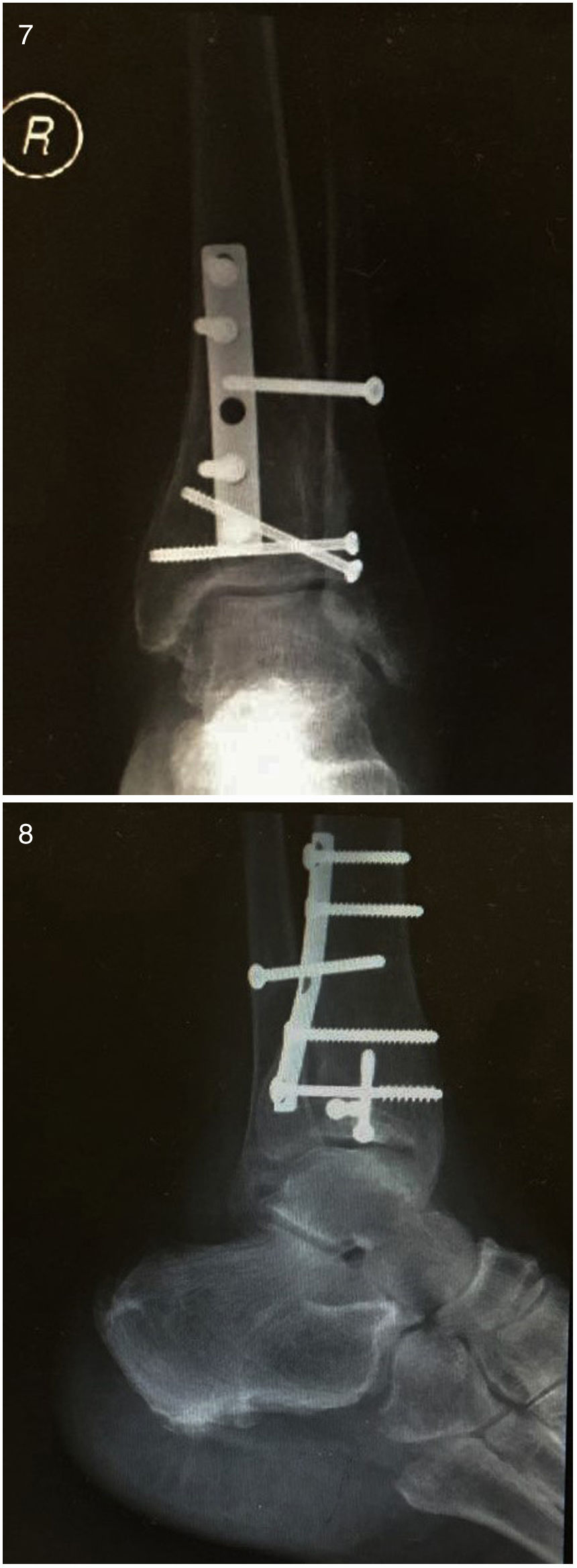
Patient underwent surgery fourteen days following the initial injury. With patient under spinal anesthesia, tourniquet control and right lateral decubitus position, a posterolateral incision was made. The Volkmann fragment was reduced and fixed with a third tubular buttress plate. Thus, the decubitus was changed to dorsal position and the syndesmosis was stabilized using a single 3.5mm fully threaded cortical screw engaging three cortices. Through an anterolateral approach, the Tillaux fracture was reduced and fixed with two cannulated lag-screws (figure 3). The entire procedure was done under fluoroscopic guidance (Figures 4, 5 & 6). Postoperatively, the patient was placed in a below-knee non-weight bearing plaster cast for 6 weeks. Within twelve weeks, clinical and radiographic assessments revealed the fracture to be well consolidated without any complications (Figures 7 & 8). At that time, full weight bearing was allowed. After twelve months of surgery, the patient returned with no symptoms or pain and complete range of motion of the ankle. The AOFAS ankle and hindfoot scale score was 100.
Discussion


Tillaux fracture has rarely been reported in adults. Literature review only presented six others reports with eight cases. This lesion is known to occur in adolescents and is defined as an avulsion fracture of the anterolateral distal tibial epiphysis. Occurs during transition period, between 12-14 years in girls and 15-18 in boys, when the medial and central physis has finished closure but the lateral physis is still open, making it weaker.8,9 The mechanism of this injury is external rotation of ankle that leads to an avulsion fracture owing to the pull of the anteroinferior tibiofibular ligament. Volkmann fracture corresponds to an avulsion-fracture of the posteroinferior tibiofibular ligament from its tibial attachment. Simultaneous Tillaux and Volkmann fractures in the adult patient is extremely rare, with only two cases previously reported. Tillaux fracture has rarely been associated with medial malleolus fracture or deltoid injury10 and the syndesmosis should be carefully evaluated. The presented case shows a unique association: Tillaux and Volkmann fractures associated with a high fibula fracture or Maisonneuve fracture.
The possible mechanism of injury in this case presented was pronation-external rotation, according Lauge-Hansen classification, characterized by, progressively, deltoid ligament rupture or fracture of the medial malleolus; disruption of the anterior syndesmosis and rupture of the interosseous ligament and membrane; spiral fracture of the fibula in its proximal half; and either a rupture of the posterior syndesmosis or a fracture of the posterior tibia.
Tillaux fracture associated with Volkmann fracture are also caused by supination-external rotation. However, in that mechanism the fibula fracture occurs at the level of syndesmosis and in case reported there was a Maisonneuve avulsion-fracture, instead.
Diagnosis is challenging in cases like this. Tillaux and Volkmann fractures can be missed in direct radiographics with anteroposterior and lateral X-ray views of the ankle. Furthermore, Maisonneuve fracture can be neglected if the leg X-ray is not done. Oblique ankle X-ray views can help in the diagnosis and additional CT evaluation is recommended if these lesions are suspected, once it assists the diagnosis and the surgical treatment.
Maisonneuve fracture treatment is surgical, with anatomic reduction and syndesmosis stabilization. Isolated Tillaux and Volkmann fractures can be treated non surgically if there is no dislocation. When displacement is>2mm, reduction and fragment fixation is advised in order to prevent further degenerative arthritis and instability.
In the presented case, there were a unique association of lesions, thus the syndesmosis was disrupted at two points, with sequent ankle instability, requiring fixation.
Tillaux fracture is an unusual injury in adults, and it́s association with Volkmann fracture and Maisonneuve fracture is even rarer. These lesions can be neglected once a careful physical exam is not performed, besides complimentary image exams. They are a serious injuries because can promote a marked ankle instability. Therefore, the surgical treatment is indispensable, beyond open reduction and internal fixation of the posterior malleolus, the Tillaux fragment and the syndesmosis, avoiding the early osteoarthritis.
FundingResearch had been performed with self funding resources by the authors.
Conflict of interestsAuthors does not declare any conflict of interests.
