



Osteoarticular infections due to anaerobes are very rare in children, with the Fusobacterium genus being the most frequently isolated. The course is usually subacute and, although there are predisposing factors described, most patients do not present with them. Generally, joint fluid cultures are sterile since these microorganisms are very sensitive to contact with oxygen, so they require specific culture media. All of the above causes the diagnosis to be delayed, increasing the risk of long-term sequelae. However, the prognosis improves when treatment is started early. The case is presented of a 10-year-old patient who was admitted for 30 days due septic arthritis of the right hip caused by Fusobacterium nucleatum During the admission, he required three surgical interventions, and completed 6 weeks of effective antibiotic therapy, with a good outcome and remaining asymptomatic at the current time.
Las infecciones osteoarticulares por anaerobios son muy raras en niños, siendo el género Fusobacterium el que se aísla con más frecuencia. El curso suele ser subagudo y, aunque hay factores predisponentes descritos, la mayoría de los pacientes no los presenta. Generalmente, los cultivos de líquido articular son estériles ya que estos microorganismos son muy sensibles al contacto con el oxígeno, por lo que precisan medios de cultivo específicos. Todo lo anterior hace que el diagnóstico se retrase y que el riesgo de secuelas a largo plazo aumente. Sin embargo, el pronóstico mejora cuando el tratamiento se inicia de modo precoz. Por todo ello, presentamos el caso de un paciente de 10 años con una artritis séptica de cadera derecha por Fusobacterium nucleatum que permaneció ingresado 30 días. Durante el ingreso precisó tres intervenciones quirúrgicas y cumplió seis semanas de antibioterapia efectiva, con buena evolución, y permanece asintomático en el momento actual.
Most osteoarticular infections in childhood have an acute course, being S. aureus the most frequent causal germ. In the face of a subacute course in which there is no response to the usual antibiotic treatment, the possibility that it is caused by an anaerobic microorganism should be considered 1; the genus Fusobacterium is the most frequent.2
Clinical caseA 10-year-old healthy boy is brought to the emergency room due to right gonalgia (knee pain) for the last 3 weeks. The patient denies antecedents of trauma and remains afebrile all the time. The articular exploration of the hip and the knee shows no limitation of mobility or inflammatory signs. X-rays of the hip and the knee are performed, without alterations, and the patient is discharged with antiinflammatory treatment.
14 days later (5 weeks of evolution) he comes due to worsening of the pain, antalgic position of the right lower limb and limitation of mobility of the right hip. The patient remains afebrile. Laboratory analyses were requested, showing mild leukocytosis and neutrophilia (13.6 × 109 leukocytes/l, 66.1% neutrophils) and C reactive protein of 15.15 mg/dl. A joint ultrasound scan is performed, which shows joint effusion in the right hip; an ultrasound-guide arthrocentesis is carried out and joint fluid of opaque appearance is extracted with 114,840 cells/mm3 (92.7% PMN) and 0 mg/dl of glucose.
Given the suspicion of septic arthritis of the right hip, traumatology indicates arthroscopy for drainage and joint lavage; in addition, intravenous cloxacillin and cefotaxime are started.
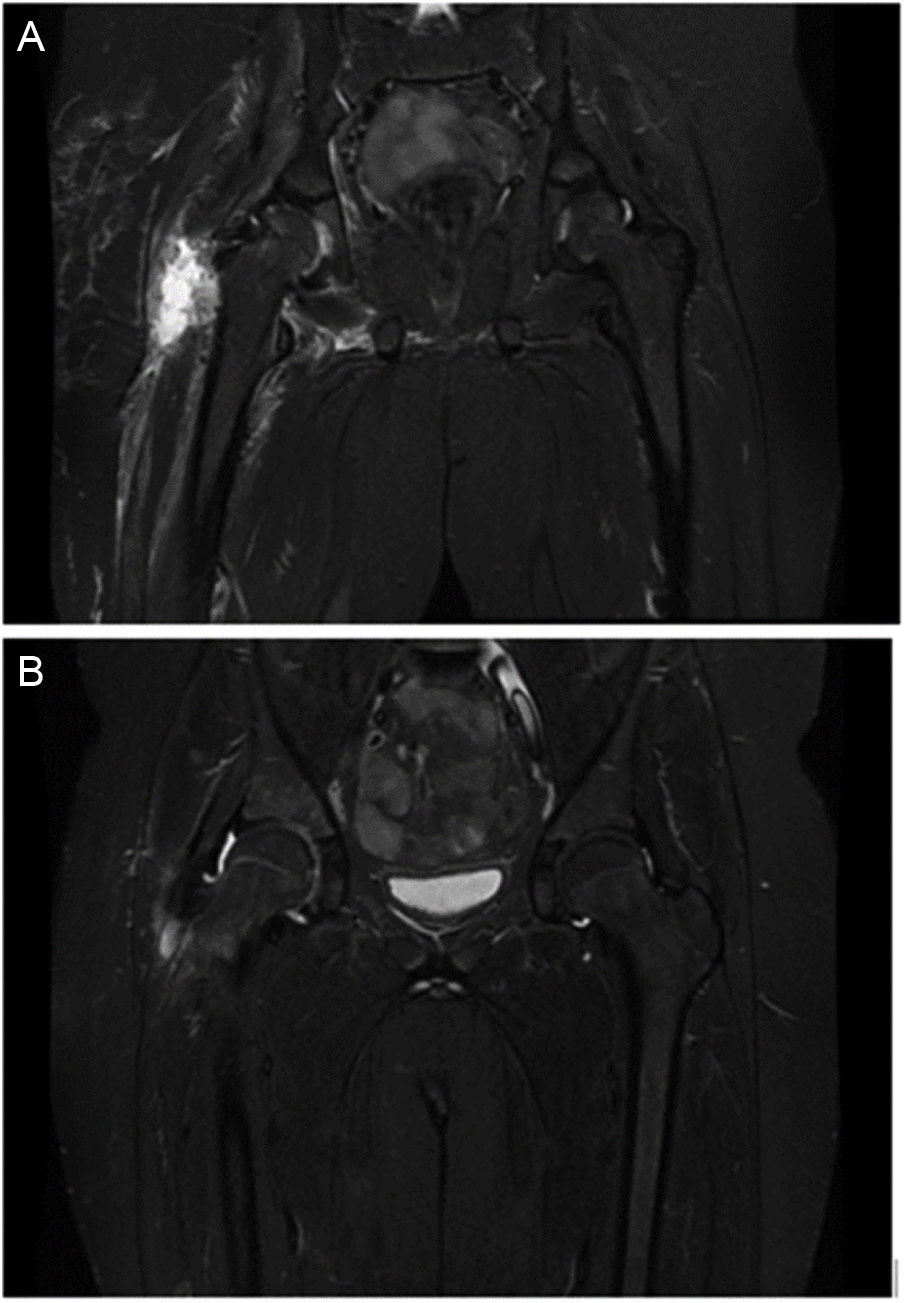
On the second day after admission, a magnetic resonance imaging (MRI) is performed, which reveals osteomyelitis in the acetabulum and myositis of the external obturator muscle and the adductor muscles (Fig. 1).
 Acetabular osteomyelitis and myositis of the external obturator muscle and adductor muscles. B) Significant improvement in acetabular bone edema. Important decrease in muscle edema.")
During the first days after admission, the clinical course was torpid, with onset of fever, worsening of pain and increase in the acute phase reactants (maximum CRP of 26.75 mg/dl and ESR of 99 mm/h), requiring, on the fifth and the seventh day after admission, arthrotomy for drainage and joint lavage.
The PCR for Kingella kingae in the joint fluid is negative and no growth is detected in the cultures thereof until the seventh day, when they notify the isolation of Fusobacterium nucleatum, for which the treatment is changed to ampicillin and metronidazole awaiting the antibiogram. After verifying sensitivity, it is changed to intravenous clindamycin; however, after the appearance of exanthema compatible with toxicodermia (that impresses to be secondary to the administration of clindamycin) the antibiotic therapy is switched back to intravenous metronidazole. After this change there was a favorable evolution, with improvement of mobility and normalization of the acute phase reactants; in addition, improvement in the MRI was observed (Fig. 1).
The patient received 3 weeks of effective intravenous antibiotic therapy; oral amoxicillin-clavulanic acid was prescribed at discharge, and a total of 6 weeks of treatment were completed.
In the subsequent follow-up, more than 2 years after diagnosis, the patient did not have sequelae.
Discussion and conclusionsWith this case we want to highlight that, even though osteoarticular infections due to anaerobic agents are infrequent in childhood,2 there is a need to think about these infections when the clinical course is atypical (subacute condition, absence of fever or poor clinical evolution with the usual antibiotic treatment).1,3 The microbiological identification by conventional methods results difficult, so if there is a high suspicion of bacterial infection and the cultures are sterile, molecular identification by 16S rRNA sequencing could be carried out.3
It is recommended that the initial treatment includes a beta-lactam antibiotic together with clindamycin or metronidazole, since the proportion of beta-lactamase-producing Fusobacterium spp is increasing. A study has also reported up to 9% of clindamycin-resistant Fusobacterium.1 In general, with adequate treatment, the prognosis is very good.2,4,5
Although this clinical picture has been related to oral cavity disease or immunosuppression,3–5 the majority do not present these antecedents,1,2 as in our case.
Conflict of interestThe authors declare that they have no conflict of interest.
Please cite this article as: Alonso de la Hoz J, Galán del Río P, Ballesteros García MM, Mayo Artuch N, Rivero Martín MJ. Osteomielitis por anaerobios. Una entidad poco frecuente en pediatría. Rev Colomb Reumatol. 2021;28:309–311.
