




Osteoarthritis is characterized by loss or loss of joint cartilage. It clinically presents with pain, rigidity, deformity, different degrees of functional disability, and a decreased perception in the quality of life of patients that suffer from it.
ObjectiveTo determine the perceived quality of life related to health in patients with osteoarthritis, and to correlate it with their functional capacity.
Materials and methodsA descriptive study including 2787 patients. A Coop/Wonca questionnaire was completed to determine perceived quality of life. Cronbach's alpha determined the internal validity and reliability of the questionnaire. Pearson correlation between quality of life and functional capacity was determined. The sociodemographic and clinical characteristics of the patients included in the study were recorded.
ResultsThe mean age was 65 years, with the majority being between 60 and 69 years, and included 65.69% females. The knees were the most affected joint group (37.82%), with 72.37% of the patients having associated comorbidity, including arterial hypertension, diabetes, and obesity. The score of the Coop/Wonca questionnaire was 21.29, with higher scores in men. The most affected dimensions were pain (3.37), physical form (3.11), and daily activities (2.98). Moderate disability predominated.
ConclusionsOsteoarthritis is associated with a large number of comorbidities. There was a correlation between functional capacity and quality of life. The Coop/Wonca chart is a very useful tool in primary health care.
La osteoartritis se caracteriza por disminución o pérdida del cartílago articular. Clínicamente presenta dolor, rigidez, deformidad, distintos grados de discapacidad funcional y disminución de la percepción de la calidad de vida de los pacientes que la padecen.
ObjetivoDeterminar la percepción de la calidad de vida relacionada con la salud en pacientes con osteoartritis y correlacionarla con la capacidad funcional de los mismos.
Materiales y métodosEstudio descriptivo en 2.787 pacientes. Se aplicó cuestionario de láminas Coop/Wonca para determinar percepción de la calidad de vida. El alfa de Cronbach determinó la validez interna y la fiabilidad del cuestionario. Se determinó la correlación de Pearson entre calidad de vida y capacidad funcional. Se describieron las características sociodemográficas y clínicas de los pacientes incluidos en la investigación.
ResultadosPromedio de edad de 65 años, predominio de edades entre 60 y 69 años y del sexo femenino (65,69%). El grupo articular más afectado fue el de las rodillas (37,82%). El 72,37% de los pacientes presentaron comorbilidad asociada con hipertensión arterial, diabetes y obesidad. La puntuación del cuestionario Coop/Wonca fue de 21,29 con puntuaciones más elevadas en los hombres. Las dimensiones más afectadas fueron el dolor (3,37), la forma física (3,11) y las actividades cotidianas (2,98). Predominó la discapacidad moderada.
ConclusionesLa osteoartritis se asocia a un gran número de comorbilidades. Existió correlación entre capacidad funcional y calidad de vida. Las láminas Coop/Wonca constituyen un instrumento de gran utilidad para ser aplicado en la atención primaria de salud.
Rheumatic diseases are considered a group of around 250 illnesses mostly affecting the musculoskeletal system. Because of the involvement of other organs and systems, rheumatic diseases are considered systemic conditions. Clinically, these pathologies are characterized by the presence of pain, inflammation, stiffness, deformity, and varying levels of disability that reduces the perceived health-related quality of life (HRQOL).1–5
Osteoarthritis (OA) is reported as the most frequently observed pathology among the adult population around the world. According to the American College of Rheumatology this disease is considered a heterogeneous group of conditions involving a broad range of symptoms and joint signs, which in combination with defective articular cartilage integrity and structural changes in the subchondral bone and in the joint margins, account for the key clinical–anatomopathological characteristics of the disease.1,2,6
It has been reported that OA affects around 30% of the population over 60 years old. Approximately 40% of the patients over the age of 50 present early imaging signs that could be related to the disease. This condition is irrefutably associated with aging, increasing the functional disability of elderly patients. Overall, it is considered the fourth cause of disability.7,8
The morbidity from rheumatic diseases in Cuba is considered to be high. OA ranks among the first 10 causes of hospital care. Moreover, considering that the incidence and the prevalence of OA increases in patients over the age of 50, and in view of the growing aging trend of the Cuban population, we may then conclude that we are facing a significant public health issue.4,5,8–11
Mechanical pain associated with stiffness is reported as the primary clinical manifestations of the disease. The pattern of joint disorder is somewhat related to gender, with a high prevalence of hands involvement among females, whilst the coxofemoral joint is more frequently affected joint in males. Spinal and knee involvement are equally described among males and females.4,6,11–13
The progressive decline of the articular function and osteo-articular pain are the main reasons why patients with OA visit the doctor. The are multiple factors in the pathology that have a negative impact on the patients’ perceived HRQOL; these are mainly pain, stiffness, subsequent deformities, and high care and treatment costs.11,14
HRQOL is defined by the World Health Organization as the personal perception of the individual about his/her life situation. This concept comprises both the cultural aspect, as well as the individual's values and their relationship with his/her objectives, expectations, and interests. This overarching concept is one of the factors currently used to measure treatment effectiveness and progress of the disease.8,11
It is however startling that despite the high frequency of OA, there are very few research reports on the topic. There are some papers in Cuba such as the publications by Góngora et al., Prada et al. and Solis-Cartas et al., focusing on HRQOL in patients with OA. However, these studies are based on small sample sizes and hence may be misleading in terms of the actual perception of patients with OA.2,4,5,11,13,15
So, considering the growing trend towards aging of the Cuban population, the high prevalence of OA among patients over 50 years old, the modest information available on the topic, and the impact of the disease on HRQOL, the decision was made to conduct this research, with a view to identify the perceived HRQOF and its relationship with functional capacity, in patients cared for at the National Center of Rheumatology, between January 2012 and May 2017.
Materials and methodsDescriptive, observational, cross-sectional study conducted in 2787 patients with a diagnosis of OA who visited the outpatient clinic at the National Center of Rheumatology between January 2012 and May 2017. Patients were included in the study based on the diagnosis of OA, pursuant to the criteria of the American College of Rheumatology.11,13 This research is the result of a 5-year study that was supplemented with previous partial reports.
A survey was designed for the research, which was evaluated by experts of the National Center of rheumatology and by rheumatologists from other hospitals in the country. The questionnaire was approved based on clinical and methodological aspects, with cross-matching for identification, interpretation and administration; additionally, a correlation test was conducted that gave a positive result. Upon approval, the questionnaire was administered to each patient, hence contributing with the collection of the variables included in the study.
The Coop/Wonca charts were selected to establish the HRQOL perception. This tool is validated in Spanish and is easy to administer and interpret. This is a generic instrument that perfectly integrates clinical and visual elements, facilitating the patient's interpretation, and delivering a rapid and adequate answer. Initially the tool comprised 9 charts that were then reduced to 7. A short version is also available using only 5 charts; however, for the purpose of our research, 7 charts were used, including: physical fitness, emotional, activities of daily life, social activities, mental status, changes in health status and pain. After presenting the pictures to the patient, he/she indicates which one depicts best his/her health condition over the last 2 weeks.11,14,16
The scale of this questionnaire ranges from 7 to 35 points. The higher the score, the poorer the patient's perceived HRQOL. Since the questionnaire is simple and easy to interpret, it can be administered in 5min. Cronbach's alpha coefficient was calculated to establish the internal validity and the reliability of the Coop/Wonca charts questionnaire.11,14
The Cuban version of the Health Assessment Questionnaire (HAQ-CU) was used to determine the functional capacity of the patients. This particular questionnaire is also validated in Spanish and tries to identify the patient's functional capacity to fulfill daily life chores. Depending on the level of disability, patients are graded from 0 points (fulfilling the chore without any limitation) to 3 points (totally dependent to do the task). The scores for each activity are added and the average is calculated, with the following final ranges: no disability (less than 0.5 points), mild disability (between 0.5 and 1 point), moderate disability (>1 point and <2 points), and severe disability in patients with scores above 2 points.11,13,14
The socio-demographic and clinical characteristics of the patients included in the research were described, comparing the results against those from other national and international studies. Pearson's coefficient was used to establish the association between the HRQOF and the functional capacity of patients with OA in the study.
For the analysis and interpretation of the information, an O/S Windows Excel 2016 database was developed. Data processing was automated using the Windows SPSS-PC version 24.5 software. The information was summarized via absolute frequencies and percentages for the qualitative variables and central tendency, and scatter measures were used for the quantitative variables. 95% confidence intervals were estimated to complete the specific calculation of the above-mentioned measurements. The calculation of Cronbach's alpha coefficient determined the internal validity and reliability of the HRQOL questionnaire. The results were illustrated in tables and graphs to make the information easier to understand.
ResultsThe analysis of the data collected is as follows:
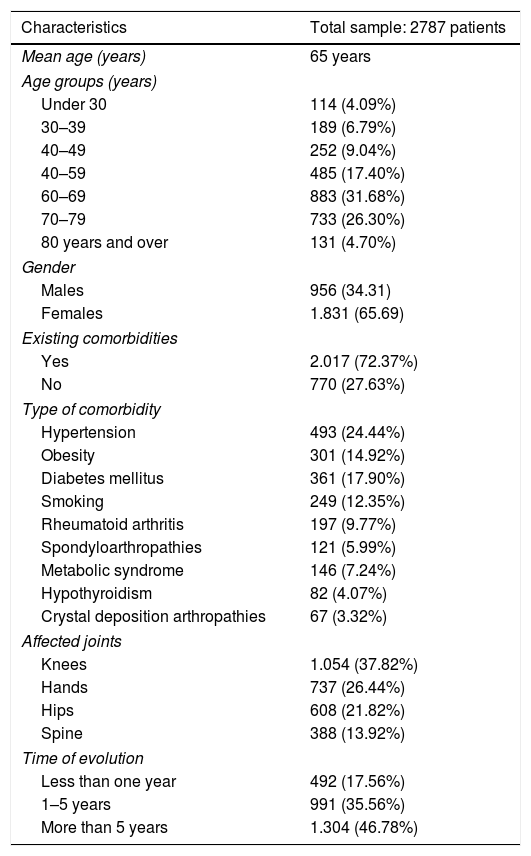
The analysis of the socio-demographic variables (Table 1) resulted in an average age of 65.7 years; most patients (31.68%) were within the 60–69 age range, followed by 26.30% between 70 and 79 years, and 17.40% between 50 and 59 years. In terms of gender, there was a prevalence of females with 1831 patients (65.69%).
Patient distribution based on socio-demographic variables.
| Characteristics | Total sample: 2787 patients |
|---|---|
| Mean age (years) | 65 years |
| Age groups (years) | |
| Under 30 | 114 (4.09%) |
| 30–39 | 189 (6.79%) |
| 40–49 | 252 (9.04%) |
| 40–59 | 485 (17.40%) |
| 60–69 | 883 (31.68%) |
| 70–79 | 733 (26.30%) |
| 80 years and over | 131 (4.70%) |
| Gender | |
| Males | 956 (34.31) |
| Females | 1.831 (65.69) |
| Existing comorbidities | |
| Yes | 2.017 (72.37%) |
| No | 770 (27.63%) |
| Type of comorbidity | |
| Hypertension | 493 (24.44%) |
| Obesity | 301 (14.92%) |
| Diabetes mellitus | 361 (17.90%) |
| Smoking | 249 (12.35%) |
| Rheumatoid arthritis | 197 (9.77%) |
| Spondyloarthropathies | 121 (5.99%) |
| Metabolic syndrome | 146 (7.24%) |
| Hypothyroidism | 82 (4.07%) |
| Crystal deposition arthropathies | 67 (3.32%) |
| Affected joints | |
| Knees | 1.054 (37.82%) |
| Hands | 737 (26.44%) |
| Hips | 608 (21.82%) |
| Spine | 388 (13.92%) |
| Time of evolution | |
| Less than one year | 492 (17.56%) |
| 1–5 years | 991 (35.56%) |
| More than 5 years | 1.304 (46.78%) |
Source: Questionnaire designed for this research project.
72.37% of the patients answered yes, when asked about existing comorbidities or harmful habits. The most frequent comorbidities were hypertension (HBP), diabetes mellitus (DM), and obesity with 24.44%, 17.90% and 14.92%, respectively. 12.35% of the patients said they were smokers. The other comorbidities included in the research represented less than 10% of the total number of patients.
The most frequently affected joints were the knees, with 37.82%, followed by the hands, hips, and spine, with 26.44%, 21.82% and 13.92%, respectively. 46.78% of the total number of patients with OA had more that 5 years of evolution of the disease, followed by 991 patients with between 1 and 5 years, and 492 patients were diagnosed with OA within less than one year.
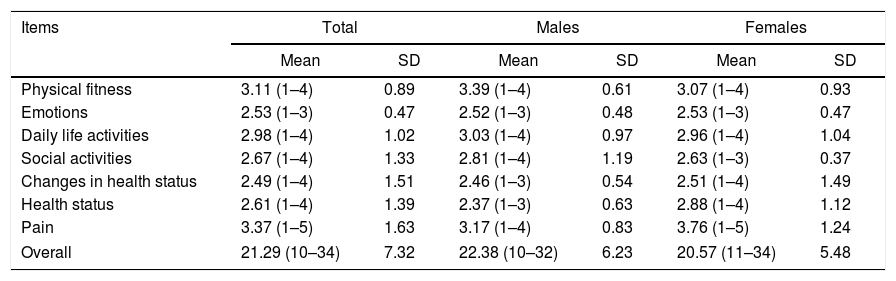
When analyzing the HRQOL based on the specific measurements and sum total (Table 2), the overall score of the study was 21.29 points. The most relevant indicators were pain, physical fitness, and daily life activities, with scores of 3.37, 3.11 and 2.98, respectively. In males, the overall score and the indicators of fitness, daily life activities, and social activities, were above the average for the study, indicating a poorer HRQOL perception in male patients. With regard to females, pain, changes in health status, and health status scored surprisingly high, performing above the study average.
Distribution of patients based on the perceived HRQOL and gender using Coop/Wonca charts.
| Items | Total | Males | Females | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Physical fitness | 3.11 (1–4) | 0.89 | 3.39 (1–4) | 0.61 | 3.07 (1–4) | 0.93 |
| Emotions | 2.53 (1–3) | 0.47 | 2.52 (1–3) | 0.48 | 2.53 (1–3) | 0.47 |
| Daily life activities | 2.98 (1–4) | 1.02 | 3.03 (1–4) | 0.97 | 2.96 (1–4) | 1.04 |
| Social activities | 2.67 (1–4) | 1.33 | 2.81 (1–4) | 1.19 | 2.63 (1–3) | 0.37 |
| Changes in health status | 2.49 (1–4) | 1.51 | 2.46 (1–3) | 0.54 | 2.51 (1–4) | 1.49 |
| Health status | 2.61 (1–4) | 1.39 | 2.37 (1–3) | 0.63 | 2.88 (1–4) | 1.12 |
| Pain | 3.37 (1–5) | 1.63 | 3.17 (1–4) | 0.83 | 3.76 (1–5) | 1.24 |
| Overall | 21.29 (10–34) | 7.32 | 22.38 (10–32) | 6.23 | 20.57 (11–34) | 5.48 |
SD: standard deviation.
Source: Coop/Wonka charts questionnaire.
The internal consistency and reliability of the use of the Coop/Wonca charts was evaluated with Cronbach's alpha (Table 3), which resulted in a coefficient of 0.872.
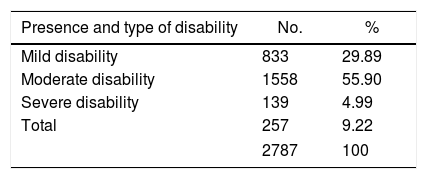
With regard to the functional capacity (Table 4), only 9.22% of the patients had no disabilities at the time of the study, while 55.9% of the participants in the survey had moderate disability.
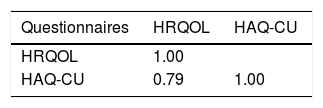
Finally, Pearson's correlation coefficient (Table 5) was analyzed, showing a direct correlation between the perceived HRQOL and functional disability.
DiscussionOA is the eldest of all rheumatic diseases identified. It is reported to affect 10% of the adult population over 60 years old. It may involve any joint, but usually affects the knees and the hips.8
There is an association between OA and ageing. Certainly the incidence of OA increases with age. A probable hypothesis to explain this situation is the cumulative effect of the articular changes that develop with ageing, such as trauma, microtrauma, reduced joint strength, thinning of the cartilage, proprioception disorders, and oxidative stress.17
Several papers report a higher prevalence among patients over 60 years old with OA. In this particular research paper, the average age was above 60 years, with a higher incidence among the patients aged between 60 and 69 years, showing that OA reaches a peak incidence in the elderly.4,11,15,18
In terms of gender, there was a prevalence of females in general. It is reported to be 5-fold more prevalent in women, and several factors may account for this situation. It has been suggested that some situations typical among females, such as higher rates of obesity, lower muscle tone, and more frequent joint hypermobility, result in varying levels of joint instability that favor the occurrence of repetitive microtrauma, leading to irreversible joint damage.19
Another factor to consider in the etiopathogenicity of the disease – which presents more often in females – is quadriceps femoris weakness. The stabilizing role of these muscles on the knee joint is well recognized; muscle weakness results in sensory dysfunction that causes reduced propioception, which favors the development of repetitive trauma and microtrauma in the joint, promoting degenerative changes. Traditionally, quadriceps strengthening has been emphasized as the most important factor in training and conditioning programs designed to protect the knee.19 Another hypothesis is that hormonal factors also play a key role in the development of the disease; this statement is based on the higher frequency of OA during menopause.17,19,20 Some authors such as Cruz García et al.18 also report a higher number of female patients with OA.
The most affected joints were the knees. Other studies, such as the paper by Solis-Cartas et al.11 also report a higher knee joint involvement. A likely explanation of this phenomenon is the presence of multiple foot deformities which are not treated promptly during the first years of life. These foot deformities increase the degree of joint misalignment, promoting the development of trauma and microtrauma, with subsequent damage to the articular cartilage.6
Another hypothesis to try to explain this situation is overweight as a triggering factor of joint damage, since the knees and the hips are the joints that bear 84% of the body weight and when subject to an excessive additional load, results in microtrauma and a subsequent degenerative process of the joint.6 The presence of OA in non-weight-bearing joints suggests that obesity may disrupt the metabolism of cartilages and bones, regardless of the mechanical effect.13,21
In most patients, the time of evolution of the disease was more than 5 years. OA is a chronic disease and ageing of the world population, and specifically of the Cuban population, may play a role in the development of OA. Keeping in mind the chronic condition of the disease and the longevity of the population, it is usual to find patients with a history of several years of evolution of the condition; hence the importance of early identification of the limitations that OA may cause, in order to prevent the impact on the functional capacity of these patients.11
The presence of comorbidities has been reported by other authors as a factor to consider at the onset, during the evolution, and the prognosis of the disease. There are multiple factors influencing the etiology and pathogenesis of OA. Inflammatory processes, metabolic disorders, and mechanical factors have been described as general risk factors in the development of the disease. Arthrosis, despite its association with a large number of comorbidities, may be considered a benign disease. Hypertension, DM, and obesity, as well as inflammatory diseases such as RA and spondyloarthropathies are reported as the comorbidities most frequently associated with OA, in addition to unhealthy lifestyles.18,22
The analysis of the global HRQOL indicator in this study resulted in an average score of 21.29. When considering the individual items in the questionnaire, pain and physical fitness were the most relevant, with scores above 3 points. This results show that OA has a negative impact on the perceived HRQOL in patients, and certainly pain and physical fitness limitations are the main targets of the disease. Notwithstanding the lack of a cutoff point, it is said that higher scores have a higher impact on the perceived HRQOL and overall scores of over 18 points evidence a decline in HRQOL.23
Comparing this result against other studies, a certain similarity is observed; Solis-Cartas et al.11 and Esteban y Peña et al.23 also report in their studies scores of around 20 points or higher, evidencing the impact on the perceived HRQOL caused by OA. Generally speaking, males had a poorer perception as compared to females. Though ageing is more prevalent among females, its consequences are more visible in men. A probable explanation could be the accumulation of work-related joint trauma or previous sports activities.24 Moreover, hip and knee-associated joint injuries that occur mostly in men, further hinder the activities of daily life, and since these are both weight-bearing joints, any injuries sustained in the hips or knees also have a negative impact on the perceived HRQOL.1,6,13
The internal consistency and reliability of Coop/Wonca charts was once again demonstrated by the higher value achieved as compared to the original version (0.82) for 9 items.16 This value shows a high reliability and ranges between 0.7 and 0.9, pursuant to the recommendation by Nunnally.25 These results are similar to those published by other researchers who achieved Cronbach's alpha values of 0.81 for 7 items and 0.75 for 5 items.26,27
This result has also been reported by Solis-Cartas et al.11 and by Esteban y Peña et al.23 with results above 0.70, which is the reference value to validate the internal consistency and reliability of any HRQOL questionnaire.11
With regard to functional disability, it should be noted that only 9.22% of the patients were not affected in their functional capacity. Moderate disability prevailed and the data show that indeed OA is a frequent source of disability in patients with this condition. Functional disability is a key factor in the symptomatology of OA.28
Pain, stiffness and the presence of deformities are reported as the main culprits of the limitation patients experience to fulfill their daily life activities. So it may be concluded that the higher the disease activity, the stronger the impact of these clinical factors and hence, the more severe the patients’ disability.28
Finally, the resulting coefficient of Pearson's correlation between the Coop/Wonca charts questionnaire and the Cuban version of the Health Assessment Questionnaire was high. This relationship indicates that at a higher level of functional disability, the perception of HRQOL is also higher, with a subsequent decline in the quality of life of patients. There is then an inverse relationship, since the qualitative and quantitative values of both variables are inversely proportional.
This study was conducted at an institution for rheumatic patients which could be a research bias. Consequently, the recommendation is to conduct similar studies in primary care, using both questionnaires as the basis to establish the functional capacity of patients, and their perceived HRQOL.
It is clear then that OA is a disease with a high incidence and a high prevalence, involving a significant number of associated comorbidities leading to high levels of disability in the patients affected by the disease. Learning about the etiology and the pathogenic factors of OA, in addition to having an interventional strategy, are all critical to minimize or delay the potential consequences of the disease on the health status of the population.
ConclusionsOA mainly affects women over 60 years of age, and the knee is the most commonly affected joint. In general, a large number of comorbidities are reported and the disease leads to varying degrees of functional disability and to a decline in the perceived HRQOL, which is more evident in males. A strong correlation was found between the HAQ and the perceived HRQOL; this means that the higher the level of disability, the poorer the perceived HRQOL. The Coop/Wonca charts questionnaire is an extremely valuable tool to determine the perceived HRQOL in patients in primary care.
Conflict of interestThe authors have no conflicts of interest to disclose.
Please cite this article as: Solis Cartas U, Calvopiña Bejarano SJ, Martínez Larrarte JP, Paguay Moreno ÁR, Saquipay Duchitanga GI. Percepción de calidad de vida en pacientes con osteoartritis. Características sociodemográficas y clínicas. Estudio de 5 años. Rev Colomb Reumatol. 2018;25:177–183.
