



To estimate the prevalence and describe the main demographic characteristics of rheumatoid arthritis in adults in Colombia.
Material and methodsA descriptive cross-sectional study was conducted using the data taken from the Integral Information System of Social Protection of the Ministry of Health during the years 2012–2016.
ResultsA total of 248,995 cases were identified, which gave an estimated prevalence of 0.52% in those older than 18 years of age. The large majority (80.7% were women, with a female:male ratio of 4.2:1, and there was a higher prevalence in the 70–74 years age group. The departments with the highest number of cases were Bogota DC (64,121), followed by Antioquia (43,771), but the departments with the highest prevalence were Cesar (1.13%), Casanare (0.96%), and Risaralda (0.93%).
ConclusionsDemographic and epidemiological information on rheumatoid arthritis in Colombia is presented. A similar prevalence is reported in other studies from the region, like Brazil (0.46%), Venezuela (0.4%), or Peru (0.55%), but lower than Argentina (0.94%) or Mexico (1.6%).
Calcular la prevalencia y describir las principales características demográficas de la artritis reumatoide en adultos en Colombia.
Materiales y métodosEstudio descriptivo de corte transversal en el que se tomaron los datos del Sistema Integral de Información de la Protección Social del Ministerio de Salud, durante los años 2012-2016.
ResultadosSe identificaron 248.995 casos, lo que permite calcular una prevalencia en mayores de 18 años del 0,52%, de los cuales el 80,7% son mujeres, con una relación mujer:hombre de 4,2:1, con mayor prevalencia entre el grupo etario de 70 a 74 años. Los departamentos con mayor número de casos son Bogotá D.C. (64.121), seguido de Antioquia (43.771); sin embargo, los departamentos con mayor prevalencia fueron Cesar (1,13%), Casanare (0,96%) y Risaralda (0,93%).
ConclusionesSe presenta información demográfica y epidemiológica de artritis reumatoide en Colombia. Se documentó una prevalencia concordante con datos de la región, similar a Brasil (0,46%), Venezuela (0,4%) y Perú (0,55%), menor que Argentina (0,94%) y México (1,6%).
Rheumatoid arthritis (RA), the most frequent of the inflammatory arthropathies, is a systemic disease of unknown etiology, affecting around 1% or the adult population.1 Its manifestations are the result of a complex interrelation between genetic and environmental factors, leading to an alteration of immune tolerance and synovial inflammation with a characteristically symmetrical pattern.2 Epidemiological studies in RA represent the liaison between the clinical practice of rheumatology and society, which allows for the identification of the frequency and clinical and demographic characteristics of the disease, in order to deploy preventive, therapeutic, or rehabilitation efforts. This paper is intended to establish the prevalence of RA in Colombia and to describe the basic demographic characteristics of patients affected by the disease, based on the official clinical – administrative records.
Materials and methodsThis is a descriptive, cross-sectional study based on the information collected from the Integral System of Information on Social Protection of the Ministry of Health of Colombia. The demographic information available in the Individual Registry of Services Delivered to patients diagnosed with RA and juvenile idiopathic arthritis (codes CIE 10:M050. M051, M052, M053, M058, M059, M06, M060, M063, M068, M080), between 2012 and 2016 was used. To calculate the prevalence in Colombia, a five-year group analysis was conducted, as well as an analysis of each of the 32 departments during the 5-year period analyzed, using as the denominator the estimated population according to the forecasts of the National Administrative Department of Statistics, based on the information from the last national census in 2005.3 Subsequently, a description of the data obtained in frequencies and percentage for qualitative variables was submitted. The paper was approved by the Committee of Clinical Research and Ethics of the Poncificia Universidad Javeriana and the San Ignacio University Hospital in Bogotá (Colombia).
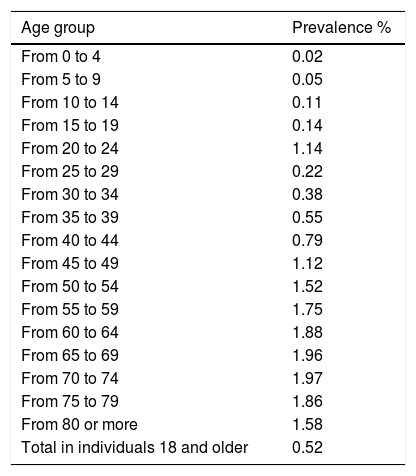
ResultsDuring the period from January 1st, 2012 and December 31st, 2016, 248.995 cases of RA were identified, representing a prevalence of 0.52% in individuals over 18 years old. The prevalence among males was 0.29% and among females was 1.21%. Of the total number of cases, 200.407 were females (80.7%9 for a female:male ratio of 4.2:1 and a higher prevalence among the age group 70–74 years old (Table 1). Because of the characteristics of the registry, it is impossible to determine the incidence rate, nor the time of evolution of the disease, which could be valuable information. The geographical regions with the highest number of cases are Bogotá D.C. (64.121 cases) followed by Antioquia (43.771 cases). However, when adjusting for the number of inhabitants per department, the departments with the highest prevalence were Cesar (1.13%), Casanare (0.96%), Risaralda (0.93%), Boyacá (0.82%), Meta (0.81%), Caldas (0.70%), Nariño (0.69%), Santander (0.68%), Huila (0.65%) and Atlántico (0.63%). The departments with a lower prevalence of the disease were Córdoba (0.15%), Valle del Cauca (0.11%), Vaupés (0.11%), Guainía (0.10%) and the archipelago of San Andrés & Providencia (0.09%). The prevalence of RA for Bogotá city was 0.33%, Cundinamarca 0.58%, and Antioquia 0.49%.
Prevalence of Rheumatoid Arthritis per age group in Colombia, from 2012 to 2016.
| Age group | Prevalence % |
|---|---|
| From 0 to 4 | 0.02 |
| From 5 to 9 | 0.05 |
| From 10 to 14 | 0.11 |
| From 15 to 19 | 0.14 |
| From 20 to 24 | 1.14 |
| From 25 to 29 | 0.22 |
| From 30 to 34 | 0.38 |
| From 35 to 39 | 0.55 |
| From 40 to 44 | 0.79 |
| From 45 to 49 | 1.12 |
| From 50 to 54 | 1.52 |
| From 55 to 59 | 1.75 |
| From 60 to 64 | 1.88 |
| From 65 to 69 | 1.96 |
| From 70 to 74 | 1.97 |
| From 75 to 79 | 1.86 |
| From 80 or more | 1.58 |
| Total in individuals 18 and older | 0.52 |
The prevalence is estimated by dividing the total number of patients per age group into the mean population of the period by age group as the denominator×100 inhabitants.
Many factors make it difficult to establish and compare the prevalence of RA, because the data vary not just in terms of the populations studied, but also in terms of the methodology used in each research project.4 Historically, studies reporting the prevalence of RA may be classified into 3 time phases. The first phase corresponds to censuses of the European and US population that provided the statistical data; the second phase used computerized data or hospital records of the populations to make estimates about the occurrence of RA – a method then called “desk epidemiology” since no field studies were conducted. Then came the age of population surveys like the so called COPCORD (Community Oriented Program for the Control of Rheumatic Diseases) methodology. The most reliable incidence, prevalence and mortality estimates in RA are those derived from population studies, but these are characterized by a broad geographical and ethnic variability.5,6
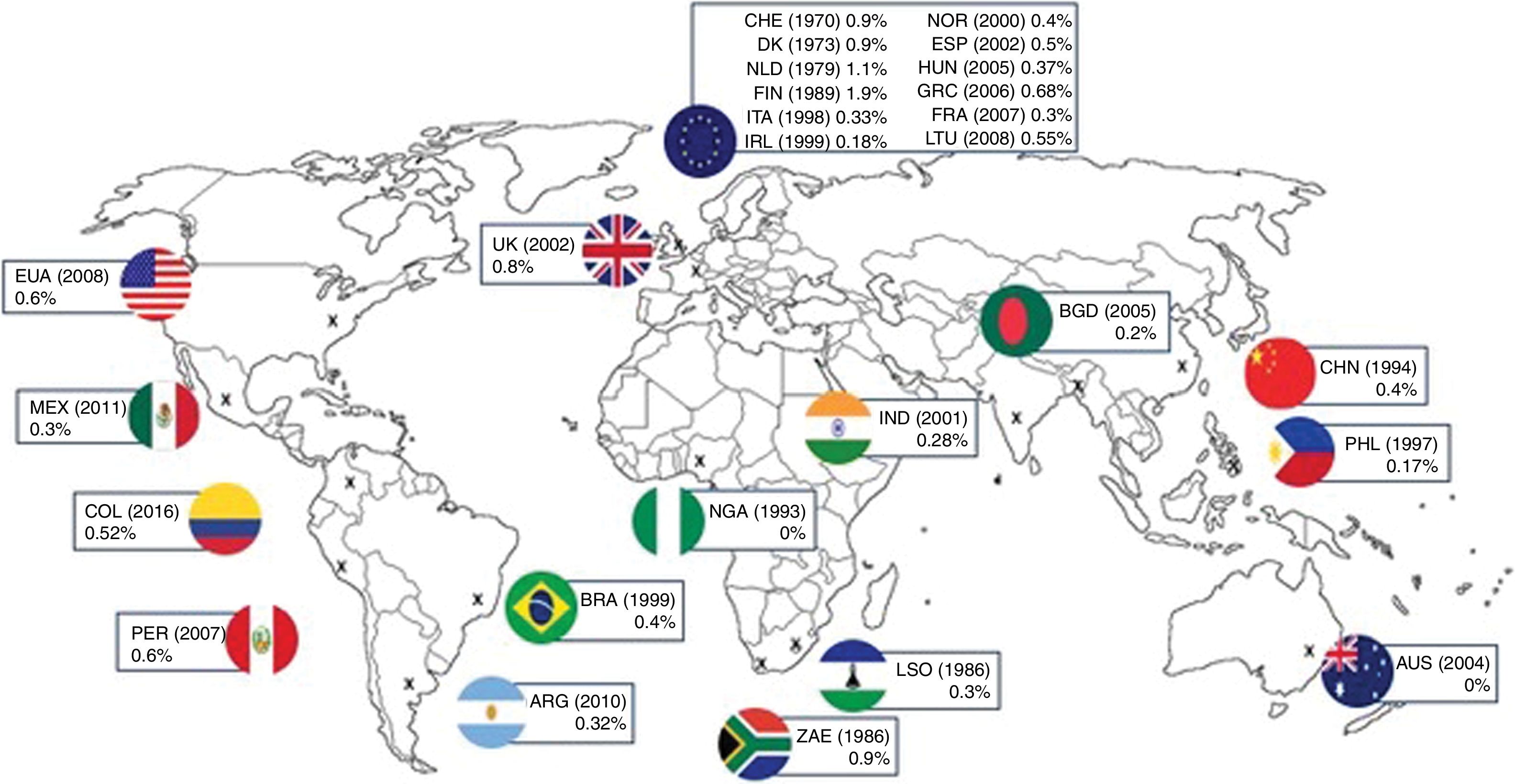
A systematic review on the incidence and prevalence of RA7 shows the huge variability of the results from various studies worldwide, with the highest prevalence documented in women and in developed countries.8 The data with the highest prevalence have been found in indigenous populations in the United States, such as the Yakima Indians (3.4%), Chippewa (5.3%) and Prima (5.3%), while the lowest levels correspond to eastern countries such as for instance a rural community in Kinmen island in China, with a prevalence of 0.3%.9,10Fig. 1 summarizes by regions the prevalence data worldwide.11,12 The prevalence of RA reported for Latin America is of around 0.5%.13 In Colombia, in a study of the Afro-Colombian population, the prevalence was estimated at 0.4%.14 Another descriptive study based on the information from medical records of an institution for rheumatic patients, identified using the keyword “rheumatoid arthritis”, reports a prevalence of 0.15%, with an average age of 53.2±13.9 years, and average onset of symptoms at 41.3±14.0 years, and a predominance of the disease among females (81.9% of the patients). However, when searching using the coeds CIE10, selection and information biases are reported, that may result in an underdiagnosis of the disease.15,16

Prevalence of RA in various countries around the world.
More recently, the “Key” project using the COPCORD methodology to establish the epidemiology of the main rheumatic diseases in Colombia, in a population over 18 years of age, surveyed 3146 males and 3547 females, and the preliminary results reported a prevalence of RA of 1.49%.17
When comparing against other Latin American countries, we found that our results show a prevalence similar to that of the populations in Brazil (0.46%), Venezuela (0.4%), and Peru (0.55%), and is lower than Argentina (0.94%), and Mexico (1.6%).11 The higher proportion of women affected is similar to the reports in other studies, with a concentration of patients in the elderly group (70–75 years old), which could be due to a longer life expectancy and to the chronicity of the disease. The elderly population warrants a more in-depth analysis in future research projects. The variation in the prevalence outcomes of the various regions in Colombia indicated in our study, may be associated with ancestral population factors in each department, and with the crossbreeding that is characteristic of the Colombian population. It should be noted that the departments with the highest prevalence are those of the Andean region and the Eastern Plains.
This study presents information on the prevalence of RA in Colombia, through the analysis of the data collected in the Individual Registry of Service Delivery to patients with a diagnosis of RA; the registry is based on the classification of CIE10 diseases with the above-mentioned codes. Nevertheless, it fails to mention the criteria used by the practitioners to make the AR diagnosis, and additionally there is the possibility that in the non-specified arthritis code, cases of patients who do not have the disease are included. This comment is relevant because the study may lead to underestimate the prevalence of the disease in our country, and this may be related to the difference found when comparing against the COPCORD Colombia data. Nevertheless, this is the official information recorded in patient care in our country and deserves further analysis, like the one submitted in this study.
Another weakness of our study is that due to the nature of the information available, it is impossible to determine the time of evolution of the disease, the incidence, the severity, the demand for specialized services related to the disease, and the mortality. Our study shows information taken from the database of the Ministry of Health of the Colombian government, which is the information used for demographic and epidemiologic analyses of the population, and forecasts for the delivery of care to patients with RA in our country.
Conflict of interestsThe authors have no conflict of interests to disclose.
To the PhD program in Clinical Epidemiology of the Pontificia Universidad Javeriana (Bogotá, Colombia) in which Dr. Daniel G. Fernández-Ávila is nominated for a PhD degree in Clinical Epidemiology.
Please cite this article as: Fernández-Ávila DG, Rincón-Riaño DN, Bernal-Macías S, Gutiérrez Dávila JM, Rosselli D. Prevalencia de la artritis reumatoide en Colombia según información del Sistema Integral de Información de la Protección Social. Rev Colomb Reumatol. 2019;26:83–87.
