


Autoimmune/autoinflammatory syndrome induced by adjuvants (ASIA) suggests that contact with different adjuvants such as silicones or aluminium used as excipient in some vaccines can cause the appearance of different symptomatology.
Materials and methodsA retrospective analysis of the clinical manifestations, laboratory parameters, treatment, and evolution of a case series of 13 patients with ASIA syndrome related to silicone implants and vaccines was performed.
ResultsIn 10 (77%) of the patients there was a history of silicone implants, in the rest of the patients there was a history of vaccination. The most frequent symptom in patients with silicone prostheses was Raynaud's phenomenon (72%), while in patients with a history of vaccination, arthralgias and myalgias were the most frequent symptoms. One patient met the criteria for primary Sjögren's syndrome while another patient had limited systemic sclerosis and associated Sjögren's syndrome. Most of the patients had elevated acute phase reactants (61%), while in the group of patients with a history of silicone prosthesis 60% presented positivity for antinuclear antibodies.
ConclusionRaynaud's phenomenon and skeletal muscle symptoms were the most common manifestations in patients with breast prosthesis and vaccination history, respectively.
el síndrome autoinmune/autoinflamatorio inducido por adyuvantes (ASIA) sugiere que el contacto con diferentes adyuvantes, tales como las siliconas o el aluminio utilizado como excipiente en algunas vacunas, puede ocasionar la aparición de diferente sintomatología.
Materiales y métodosse realizó un análisis retrospectivo de las manifestaciones clínicas, los parámetros de laboratorio, el tratamiento y la evolución de una serie de casos de 13 pacientes con síndrome ASIA relacionado con implantes de siliconas y vacunas.
Resultadosen 10 (77%) de los pacientes existía el antecedente de implantes de siliconas, mientras que en el resto había antecedente de vacunación. El síntoma más frecuente en las pacientes con prótesis de siliconas fue el fenómeno de Raynaud (72%), en tanto que en los pacientes con antecedentes de vacunación, las artralgias y las mialgias fueron los síntomas más frecuentes. Una paciente cumplía criterios para síndrome de Sjögren primario, mientras que otra paciente presentaba esclerosis sistémica limitada y síndrome de Sjögren asociado. La mayoría de los pacientes tuvieron reactantes de fase aguda elevados (61%), mientras que en el grupo de pacientes con antecedentes de prótesis de siliconas, el 60% presento positividad a anticuerpos antinucleares.
Conclusiónel fenómeno de Raynaud y los síntomas musculoesqueléticos fueron las manifestaciones más comunes en pacientes con prótesis mamarias y antecedentes de vacunación, respectivamente.
In 2011, Schoenfeld and Agmon-Levin introduced a new syndrome known as adjuvant-induced autoimmune/autoinflammatory syndrome (ASIA). This syndrome encompasses four conditions: Gulf War syndrome, macrophagic myofasciitis, siliconosis, and post-vaccination adverse effects. It suggests that in genetically predisposed individuals, exposure to various adjuvants, such as silicones or aluminum used as excipients in some vaccines, can lead to a range of clinical manifestations, including myalgia, arthralgia, fatigue, or neurological symptoms.1
Since its introduction, numerous publications have reported patients with diverse symptoms linked to an expanding array of adjuvants.
This brief study describes the clinical and laboratory manifestations of 13 patients with ASIA syndrome related to silicone implants and vaccines.
Materials and methodsBetween January 2014 and July 2020, 13 subjects exhibiting clinical manifestations indicative of ASIA syndrome were treated at the Rheumatology Section of JB Iturraspe Hospital and the Rheumatology Section of Garay Sanatorium, both located in Santa Fe, Argentina.
A retrospective analysis was conducted, reviewing clinical manifestations, laboratory parameters, treatments, and outcomes for patients with a history of vaccination and silicone prostheses.
The study involved reviewing medical records, which posed no risk to patients and did not require informed consent. The protocol was approved by the hospital’s Teaching and Research Committee.
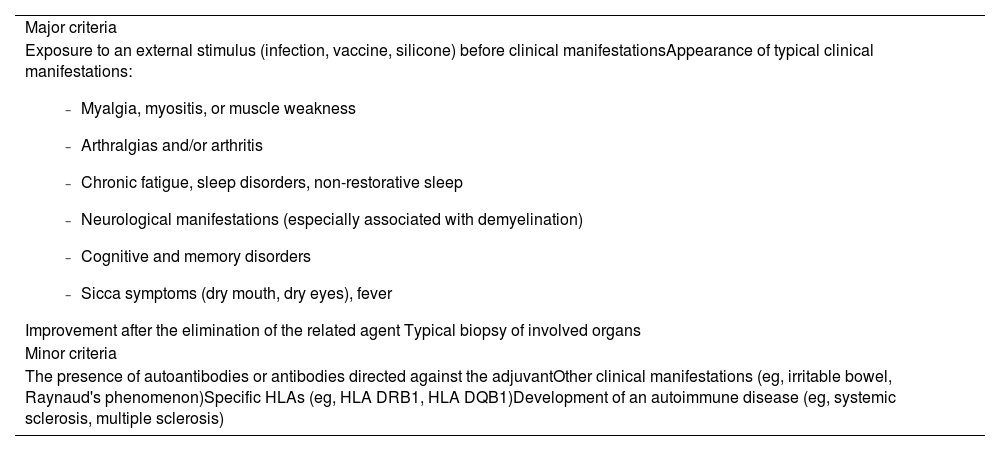
Diagnosis was based on the criteria suggested by Schoenfeld et al., as applied by the treating physician (Table 1).
Diagnostic criteria for ASIA syndrome.
| Major criteria |
Exposure to an external stimulus (infection, vaccine, silicone) before clinical manifestationsAppearance of typical clinical manifestations:
|
| Minor criteria |
| The presence of autoantibodies or antibodies directed against the adjuvantOther clinical manifestations (eg, irritable bowel, Raynaud's phenomenon)Specific HLAs (eg, HLA DRB1, HLA DQB1)Development of an autoimmune disease (eg, systemic sclerosis, multiple sclerosis) |
Two major criteria, or one major and two minor criteria, are necessary for the patient to be diagnosed with ASIA syndrome.
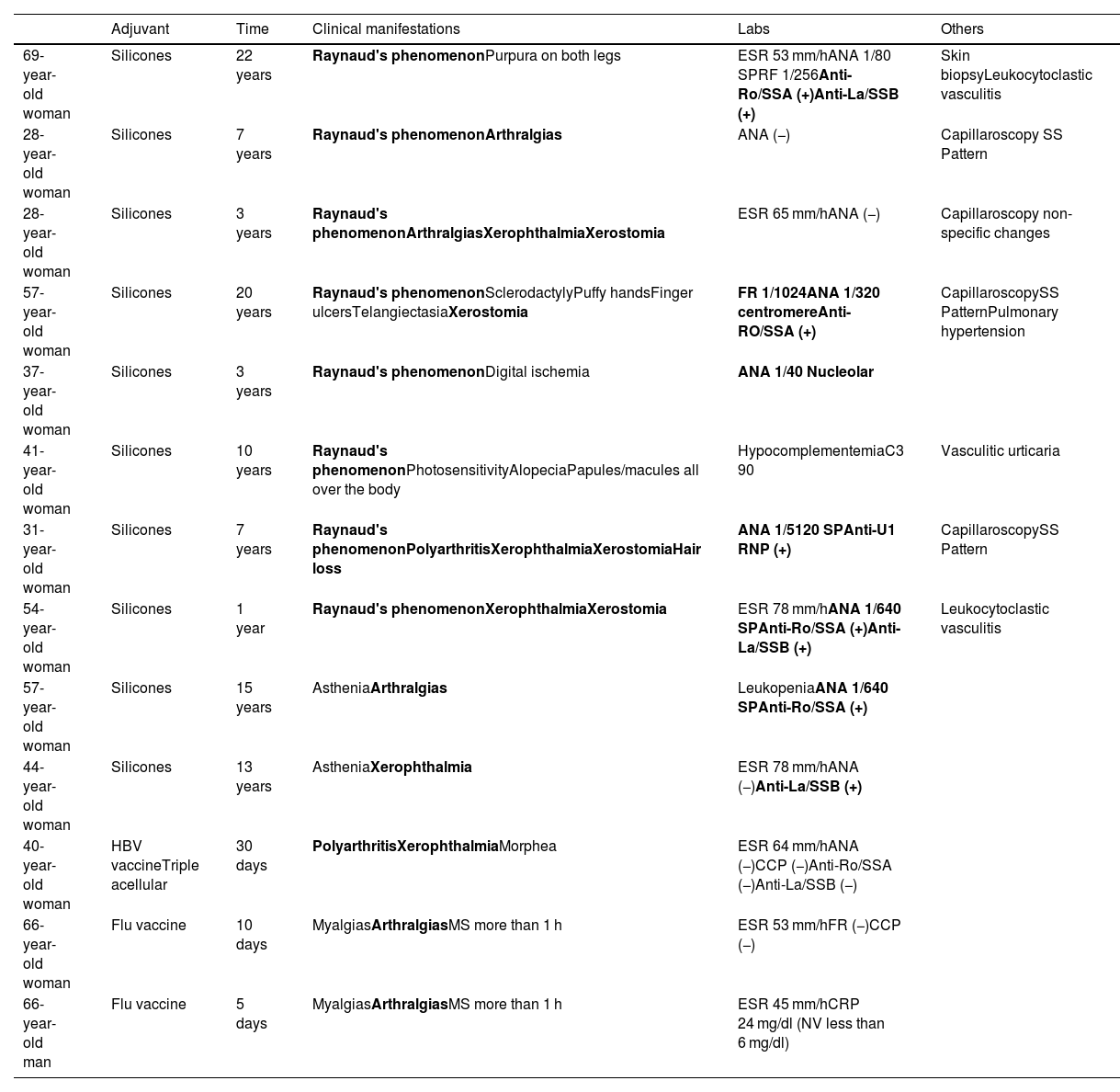
The medical records of 13 patients (12 women and one man) were reviewed, with a median age of 47 ± 14 years (range 28–69) (see Table 2). Among these patients, 10 (77%) had a history of silicone implants, while 3 (23%) had a history of vaccination (2 women and one man).
Main clinical and laboratory manifestations in 13 patients with ASIA syndrome.
| Adjuvant | Time | Clinical manifestations | Labs | Others | |
|---|---|---|---|---|---|
| 69-year- old woman | Silicones | 22 years | Raynaud's phenomenonPurpura on both legs | ESR 53 mm/hANA 1/80 SPRF 1/256Anti-Ro/SSA (+)Anti-La/SSB (+) | Skin biopsyLeukocytoclastic vasculitis |
| 28-year- old woman | Silicones | 7 years | Raynaud's phenomenonArthralgias | ANA (−) | Capillaroscopy SS Pattern |
| 28-year-old woman | Silicones | 3 years | Raynaud's phenomenonArthralgiasXerophthalmiaXerostomia | ESR 65 mm/hANA (−) | Capillaroscopy non-specific changes |
| 57-year-old woman | Silicones | 20 years | Raynaud's phenomenonSclerodactylyPuffy handsFinger ulcersTelangiectasiaXerostomia | FR 1/1024ANA 1/320 centromereAnti-RO/SSA (+) | CapillaroscopySS PatternPulmonary hypertension |
| 37-year-old woman | Silicones | 3 years | Raynaud's phenomenonDigital ischemia | ANA 1/40 Nucleolar | |
| 41-year-old woman | Silicones | 10 years | Raynaud's phenomenonPhotosensitivityAlopeciaPapules/macules all over the body | HypocomplementemiaC3 90 | Vasculitic urticaria |
| 31-year- old woman | Silicones | 7 years | Raynaud's phenomenonPolyarthritisXerophthalmiaXerostomiaHair loss | ANA 1/5120 SPAnti-U1 RNP (+) | CapillaroscopySS Pattern |
| 54-year-old woman | Silicones | 1 year | Raynaud's phenomenonXerophthalmiaXerostomia | ESR 78 mm/hANA 1/640 SPAnti-Ro/SSA (+)Anti-La/SSB (+) | Leukocytoclastic vasculitis |
| 57-year-old woman | Silicones | 15 years | AstheniaArthralgias | LeukopeniaANA 1/640 SPAnti-Ro/SSA (+) | |
| 44-year- old woman | Silicones | 13 years | AstheniaXerophthalmia | ESR 78 mm/hANA (−)Anti-La/SSB (+) | |
| 40-year- old woman | HBV vaccineTriple acellular | 30 days | PolyarthritisXerophthalmiaMorphea | ESR 64 mm/hANA (−)CCP (−)Anti-Ro/SSA (−)Anti-La/SSB (−) | |
| 66-year- old woman | Flu vaccine | 10 days | MyalgiasArthralgiasMS more than 1 h | ESR 53 mm/hFR (−)CCP (−) | |
| 66-year-old man | Flu vaccine | 5 days | MyalgiasArthralgiasMS more than 1 h | ESR 45 mm/hCRP 24 mg/dl (NV less than 6 mg/dl) |
The criteria that each patient met are highlighted in bold.
ANA: antinuclear antibodies; ESR: erythrocyte sedimentation rate; RF: rheumatoid factor; SP: speckled; HBV vaccine: hepatitis B vaccine; SS: Systemic sclerosis; CRP: C-reactive protein; NV: Normal velue.
All subjects in this group were women. Of these, 9 had breast implants, while one had an implant in the left calf due to congenital hypotrophy. The time between exposure to the adjuvant and the onset of symptoms ranged from one to 22 years. The most common symptom leading to consultation was Raynaud's phenomenon, observed in 8 individuals (80%). Nailfold capillaroscopy was performed in 4 of these patients, revealing a scleroderma pattern in 3 and non-specific changes in the fourth. Sicca symptoms (xerostomia and xerophthalmia) were the second most frequently reported, occurring in 50% of the cases.
Acute-phase reactants were elevated in 40% of the patients. Antinuclear antibodies were positive in 60% (6/10), and positivity for anti-Ro/SSA and/or anti-La/SSB antibodies was observed in 5 cases (50%). There was an association between sicca symptoms and positivity for anti-Ro/SSA and/or anti-La/SSB antibodies in 3 individuals, one of whom met the criteria for primary Sjögren's syndrome according to the ACR-EULAR criteria.2 Additionally, one patient met the criteria for limited systemic sclerosis, presenting with Raynaud's phenomenon, sclerodactyly, digital ulcers, pulmonary hypertension, and positive anticentromere antibodies, along with associated Sjögren's syndrome.
Although 3 of the subjects did not meet the major criteria for ASIA syndrome, 2 presented symptoms of autoimmune rheumatological disease, such as leukocytoclastic vasculitis, while the third exhibited severe Raynaud's phenomenon with digital necrosis and antinuclear antibodies (ANA) with a nucleolar pattern.
Patients with Raynaud's phenomenon were advised to protect themselves from cold, sometimes with the addition of calcium channel blockers. Two of the 3 individuals with leukocytoclastic vasculitis were treated only with prednisone, while the third patient (with hypocomplementemic leukocytoclastic vasculitis) received hydroxychloroquine (HCQ) in addition to steroids. Patients with xerophthalmia were treated with artificial tears.
Patients with a vaccination historyThe vaccines administered included anti-influenza vaccines for 2 patients, while the third received the hepatitis B vaccine along with the triple acellular vaccine, which contains purified tetanus and diphtheria toxoids and 3 purified Bordetella pertussis antigens. This last patient was the only one with a history of autoimmune disease, having been diagnosed with primary antiphospholipid syndrome with obstetric manifestations (recurrent miscarriages).
In patients with a history of vaccination, symptoms appeared between 5 and 30 days after immunization, with arthralgias and myalgias being the most common. The 2 individuals who received the influenza vaccine exhibited symptoms similar to those seen in polymyalgia rheumatica. All cases were accompanied by elevated acute-phase reactants.
All individuals with a history of vaccination were treated with low doses of corticosteroids with good results. However, the patient who received the hepatitis B and triple acellular vaccines required a combination of HCQ and methotrexate (MTX) due to persistent arthritis.
Patient outcomesBoth groups—those with a history of silicone implants and those with a history of vaccination—generally showed favorable outcomes. The exception was the patient who received the hepatitis B and triple acellular vaccines, developing polyarthritis and a facial lesion compatible with morphea, which required topical treatment.
DiscussionAdjuvants are immunological molecules that enhance the specific immune response to antigens and are commonly used in vaccine production. Their use improves immune response, which reduces the frequency and number of vaccines required to achieve sufficient preventive immunity. These molecules affect both adaptive and innate immune responses through various mechanisms, such as the activation of Toll-like (TLRs), NOD-like (NLRs), and type C lectin-like receptors. Proinflammatory cytokines are produced, which promote the chemotaxis of dendritic cells and the activation of antigen-presenting cells, leading to a stronger T-cell response and a more robust adaptive immune response to the antigen. However, in genetically predisposed individuals, adjuvants can induce the production of autoantibodies and the development of autoimmune diseases.3
For decades, there were concerns about the safety of silicone implants, leading the Food and Drug Administration (FDA) to impose a moratorium on silicone gel breast implants in 1992, which was lifted in 2006.4 Although silicone was once considered biologically inert, it is now known that microparticles can migrate and be captured by macrophages in the circulatory system and be detected in various tissues, including the central nervous system. This can lead to immunological abnormalities and potentially cause autoimmune diseases. Silicone has been linked to symptoms such as fatigue, cognitive disorders, arthralgias, myalgias, pyrexia, and sicca symptoms.5 A study involving 24,651 individuals with silicone breast implants found an association with systemic sclerosis, Sjögren syndrome, and sarcoidosis.6 Additionally, a systematic review revealed that patients with silicone implants have a higher risk of rheumatoid arthritis (RA), Sjögren syndrome, and Raynaud's phenomenon.4
Among our patients with silicone implants, Raynaud's phenomenon was prevalent, and 40% also exhibited sicca symptoms. One subject met the criteria for primary Sjögren syndrome, while another met the criteria for limited systemic sclerosis with associated Sjögren syndrome. Although it is debated whether removing the prosthesis alleviates symptoms, Brazilian researchers observed that patients with silicone breast implants who met any major criteria of ASIA syndrome had a 5.6 times greater risk of undergoing prosthesis removal, compared to those with no criteria. Patients with minor criteria had a 4.3 times higher risk.7
Vaccines have undeniably contributed to the eradication and control of numerous infectious diseases, significantly improving global quality of life. However, rare immunological adverse reactions may occur in genetically predisposed individuals. The hepatitis B vaccine has been associated with arthralgia-myalgia, the development of RA, flare-ups of systemic lupus erythematosus, and vasculitic lesions.8 Other studies have reported a high frequency of neuropsychiatric symptoms, often linked to musculoskeletal complaints.9
It has been suggested that undifferentiated connective tissue disease—characterized by clinical manifestations suggestive of autoimmune disease but not fitting a definitive diagnosis—might be part of the ASIA syndrome spectrum, with a stronger association with hepatitis B and tetanus toxoid vaccinations. Specifically, tetanus toxoid was associated with a higher frequency of positivity for anti-β2 glycoprotein 1 antibodies.10 In one case, a patient with antiphospholipid syndrome developed chronic polyarthritis, xerophthalmia, and a localized morphea lesion after receiving the hepatitis B and tetanus toxoid vaccines, both containing aluminum hydroxide or phosphate as an adjuvant.
Additionally, anti-influenza vaccination has been linked to polymyalgia rheumatica and giant cell arteritis,11 as observed in two of our patients, who responded well to low-dose prednisone.
Recently, in Mexico City, 36 individuals who received various COVID-19 vaccines, over seven months, were diagnosed with ASIA syndrome.12 A recent multicenter study of 500 subjects found that the most frequent symptoms of ASIA syndrome were arthralgia and chronic fatigue, affecting nearly three-quarters of patients, while Raynaud's phenomenon and sicca symptoms were observed in about 20%.13
ConclusionsSince its description in 2011, ASIA syndrome has emerged as a condition that highlights the interplay of genetic, hormonal, environmental, and immunological factors in the development of autoimmunity. In our case series, Raynaud's phenomenon and musculoskeletal symptoms were the most common manifestations among patients with breast implants and a history of vaccination, respectively. When assessing these patients, it is important to consider any history of exposure to these adjuvants.
Ethical considerationsThe study involved a review of medical records, which posed no risk to patients, so informed consent was not required. The protocol was approved by the hospital's Teaching and Research Committee.
FinancingThere is nothing to declare.
Conflict of interestThe authors have no conflicts of interest to declare.
