



Medializing calcaneal osteotomy forms part of the treatment options for adult acquired flat foot. The structural correction that is achieved is widely known. However, the effect of this procedure on the soft tissues that support the plantar arch has been little studied, since it is not possible to quantify experimentally the tension and deformation variations generated. Therefore, the objective of this study was to evaluate the effect of medializing calcaneal osteotomy on the soft tissue that supports the plantar arch, using a computational model of the human foot designed with a clinical approach. The proposed finite element model was reconstructed from computerised tomography images of a healthy patient. All the bones of the foot, the plantar fascia, cartilages, plantar ligaments and the calcaneus-navicular ligament were included, respecting their anatomical distribution and biomechanical properties. Simulations were performed emulating the monopodal support phase of the human walk of an adult. The effect on each tissue was evaluated according to clinical and biomechanical criteria. The results show that calcaneal osteotomy reduces the tension normally generated on the evaluated tissues, with the effect on the calcaneus-navicular ligament and the plantar fascia being the most notable. The deformation results obtained are consistent with experimental tests and clinical knowledge. The versatility of this model allows the objective assessment of different conditions and supports decision making for the treatment of adult acquired flat foot in middle and advanced stages.
La osteotomía medializante de calcáneo forma parte del elenco de opciones de tratamiento en el pie plano adquirido en adultos. La corrección estructural que se consigue es ampliamente conocida. Sin embargo, el efecto de este procedimiento sobre los tejidos blandos que soportan el arco plantar ha sido poco estudiado, pues experimentalmente no es posible cuantificar las variaciones de tensión y deformación generadas. Por lo tanto, el objetivo de este estudio fue evaluar el efecto que tiene la osteotomía medializante de calcáneo sobre el tejido blando que soporta el arco plantar, usando un modelo computacional de pie humano diseñado con un enfoque clínico. El modelo por elementos finitos propuesto fue reconstruido a partir de imágenes de tomografías computarizadas de un paciente sano. Se incluyeron todos los huesos del pie, la fascia plantar, cartílagos, ligamentos plantares y el ligamento calcáneo-navicular, respetando su distribución anatómica y propiedades biomecánicas. Las simulaciones fueron realizadas emulando la fase de apoyo monopodal de la marcha humana de un adulto. El efecto sobre cada tejido fue evaluado siguiendo criterios clínicos y biomecánicos. Los resultados muestran que la osteotomía de calcáneo reduce la tensión generada normalmente sobre los tejidos evaluados, siendo el efecto sobre el ligamento calcáneo-navicular y la fascia plantar los más notables. Los resultados de deformación obtenidos son consistentes con ensayos experimentales y el conocimiento clínico. La versatilidad de este modelo permite la valoración objetiva de diferentes condiciones y apoya la toma de decisión para el tratamiento del pie plano adquirido en adultos en estadios medio y avanzado.
Adult-acquired flat foot has been an object of clinical research in recent years due to an increase in the condition and the great variability of treatment alternatives currently available. The treatment options range from orthesis, for the initial stages, to mid-and hindfoot athrodesis for the more advanced stages of the condition.1–3 Calcaneal medializing osteotomy is one of the most commonly used techniques to correct the pronation characteristic of flatfoot. In some cases, this correction of the bone structure is not sufficient and tissue stress persists at greater or less intensity for specific tissues.1 The clinical experience of the surgeon will determine the need to combine other described techniques on soft tissues or other bone.
This highly subjective component regarding this procedure is caused, in part, by the still latent lack of knowledge of biomechanical variables that have not been appropriately assessed from an experimental perspective. The high biomechanical complexity of the foot, both static and dynamic, the difficulty of segmenting and treating the tissue appropriately during tests, and the limitations of the measurement tools themselves are the main problems.4,5
One way of improving diagnostic objectivity and decision-making is to quantify the effect created by calcaneal osteotomy on the structure of the foot and the soft tissues that support the plantar arch. In recent years, various models have been proposed to describe and evaluate the biomechanics of the normal and the pathological foot.6–8 However, to date, there is no agreed research model to study adult-acquired flatfoot following calcaneal osteotomy.9 Experimental studies have been performed on cadavers, subjecting bodies to progressive loads, evaluating the deformation of the foot structure generated.10–12 However, these experimental models require major financial investment on equipment and better control of study specimens to ensure that the biomechanical characteristics of the tissue remain unaltered.13
Recently, technological advances have considerably increased the processing capacity of computers. This has lead to the design of complex numerical models for studying the biomechanics of the human foot.14 These models are considered a valid alternative, because the researcher can subject the model to loads on “virtual” structures without the need for physical material, with the advantage of being able to alter the structural parameters that most affect the foot–ankle complex. Thus, it is possible to evaluate the response on soft tissues, joints, tendinous complex and muscle tissue.13,15–17 Of course, its validity is supported by appropriate design of the physiological structures and realistic modelling of the mechanical properties of the tissue and its physionomy.18
These models, principally based on finite element modelling, base their study on variables and parameters taken from general experimental papers, ignoring some tissues and characteristics that relate directly to the development of adult-acquired flatfoot.19 In clinical practice, some tissues with passive action have been identified, such as the plantar fascia,20,21 the plantar ligaments and calcaneonavicular ligament or spring ligament,21,22 which participate significantly in the development of this condition. The current published models simulate these tissues without considering their geometry or characteristic hyperelastic behaviour.15,17 Therefore, their approach is not realistic, and therefore reduces the clinical value of these proposals.
In this article we propose a new computational model that enables the clinical and biomechanical assessment of calcaneal medializing osteotomy used to correct flatfoot, and the objective evaluation of its effect on each of the tissues that passively support the plantar arch, with results comparable to those of experimental clinical trials. This model includes the geometry of the tissues and biomechanical characteristics close to those of the real human foot. The study evaluates both the collapse and flattening of the plantar arch and talocalcaneal divergence. These are clinical signs that are commonly measured by the internal Moreau-Costa-Bertani angle and Kite's angle. The simulations were performed in the absence of the tissue assessed and only with it present on a normal model and one with the calcaneal osteotomy, in order to evaluate the effect of this surgical procedure on each tissue objectively.
Material and methodFinite element control modelThis study took as its base the model proposed by Morales-Orcajo, et al.,23,24 designed by an Applied Mechanics and Bioengineering research group from the University of Saragossa (Spain). This model starts from the reconstruction of a human foot of a patient with neuropathic metatarsalgia using a conventional SIEMENS SOMATON clinical scanner. The study resolution was .44 on the transversal plane, and 1.0mm in a longitudinal direction. Materialise MIMICS V10 software was used for the segmentation, and reconstruction of the tissue was performed using MIMICS v software. This model maintains the morphology of the cartilage and the plantar fascia, and the differentiation of cortical and trabecular bone, which is generally ignored by other authors despite the importance of considering this differentiation in modelling bone mechanics.24,25 The spring ligaments (SL), the short plantar ligament (SPL) and the long plantar ligament (LPL) were also included, which are essential for appropriately analysing the development of adult-acquired flatfoot. The geometry of each tissue was designed taking the anatomical atlas and cadaver images as the basis, under the advice of doctors and specialists. The mesh of the model was created using ANSYS V.15 software, generating 57453 tetrahedral elements. The model generated is shown in Fig. 1.
Finite element model of medializing osteotomy
The mesh of the control model was modified to replicate a 45° oblique calcaneal osteotomy from proximal to distal and from dorsal to plantar. Medial sliding 1cm of the most proximal segment of the calcaneal osteotomy was performed and this position was considered fixed, thus simulating the effect of osteosynthesis fixation without the need to be added as an external element to the model.
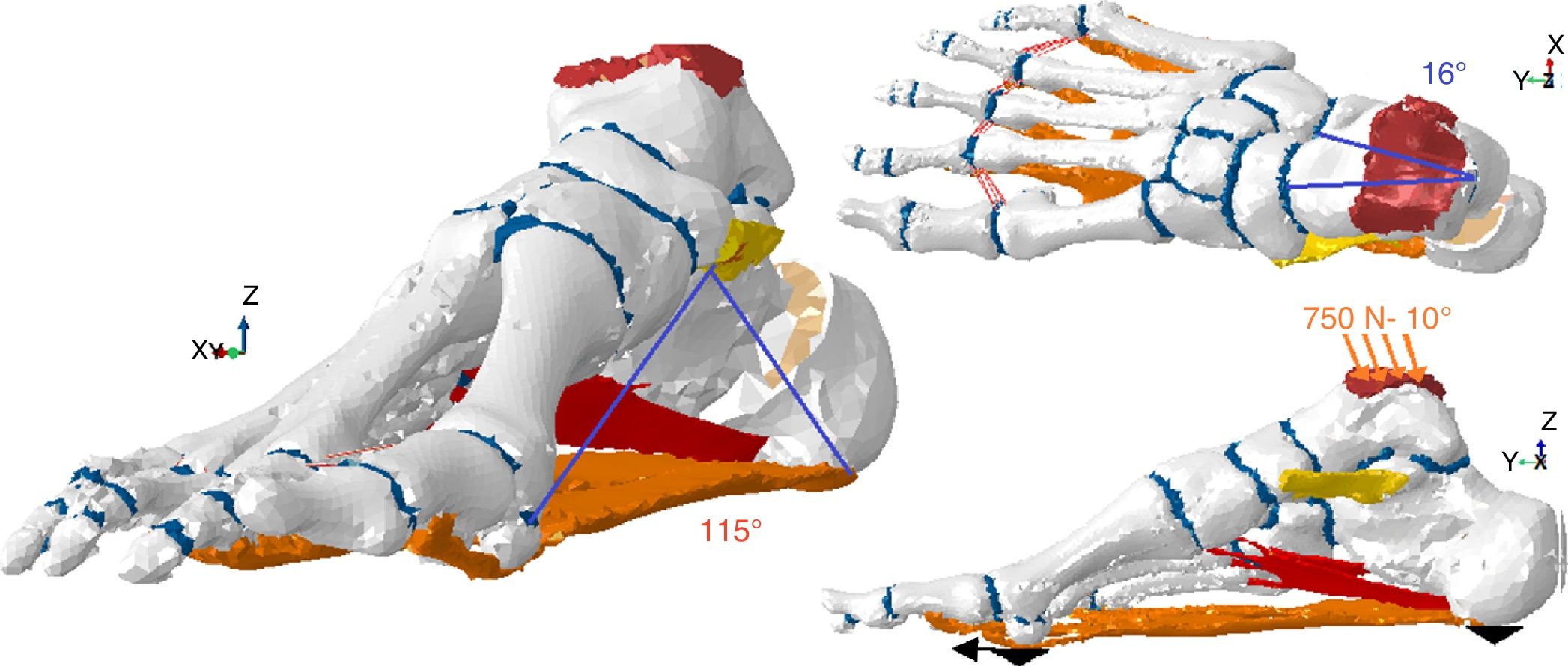
Load conditionsThe model was designed from tomographic images of a resting foot (with no load) (Fig. 1). To deform this initial geometry until a position of load and during the second rocker, the model was simulated with all the passive tissues that support the plantar arch using a load of 750N. This load represents the full weight of a 75kg adult, borne by the foot assessed.
The load was introduced vertically in a downward direction, with a 10-degree incline as suggested by some authors,13,25 distributed over the tibio-talar (90%) and fibular-talar (10%) contact area. The simulations were performed keeping the nodes of the most plantar end of the calcaneus fixed and blocking the most plantar nodes of the first and fifth metatarsals sliding over the Z axis (vertical), simulating the effect of the ground on the model of the foot during the second rocker of gait.
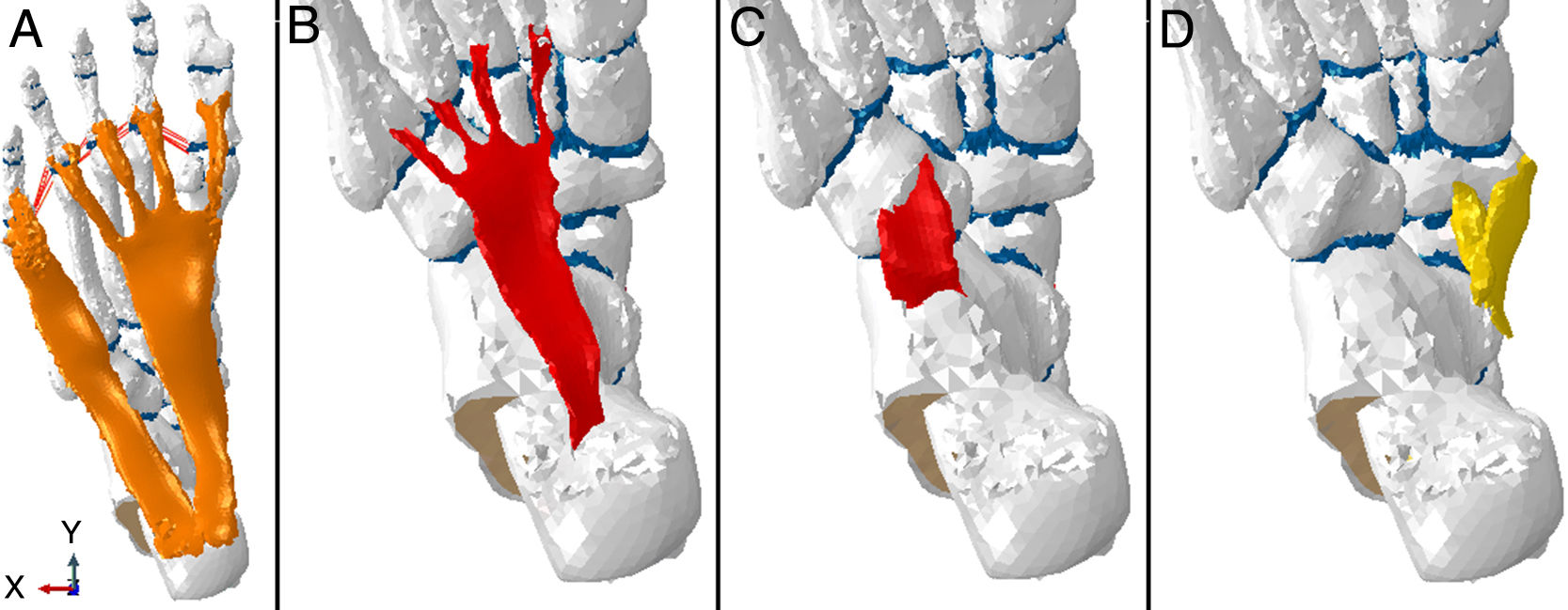
Anatomical elementsThe model maintains the bone structure of the base model, differentiating the properties of the cortical and trabecular component of the bone,24 and is complemented with ligaments, cartilage and planar fascia in the appropriate anatomical positions (Fig. 2).
, long plantar ligament (B), short plantar ligament (C) and spring ligament (D), included in the model.")
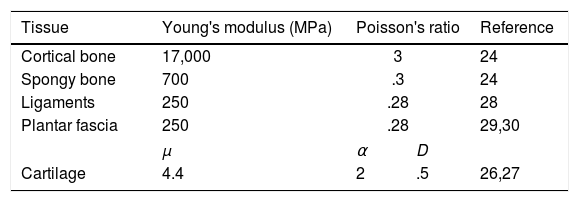
The tissue models were considered elastic linear elements, using previously published biomechanical properties (Table 1). A non-linear and hyperelastic model, which better represents the tissue mechanics, was considered appropriate to model the cartilage, characterised by displacement of fluid in the presence of compression. This dynamic behaviour is represented using Ogden's model, following the suggestions published by Mansour and Wu.26,27 The parameters used for each tissue are summarised in Table 1.
Study variablesThe structural changes of the plantar arch were quantified by determining the Internal Moreau-Costa-Bartani (IMCB) angle and talocalcaneal divergence through Kite's angle. The Ruler application was used for this measurement, developed by Ergonauts and the Polytechnical University of Valencia.31 This assessment was made on a control foot model and on the calcaneal medialising osteotomy model. Both models were evaluated under the same conditions of load.
To determine the collapse and pronation of the foot model, and the effect of calcaneal osteotomy (medialized calcaneus) on each of the tissues evaluated, we calculated the difference of the results of each simulation with the results of the model without calcaneal osteotomy (anatomical calcaneus), estimating the relative difference of each evaluation. For each case (anatomical and medialized), we took as the basis the difference between the deformation of the complete model and the maximum deformation generated on simulation maintaining only the bone structure.
In order to determine the biomechanical effect of calcaneal osteotomy on each tissue, the simulations were developed in the absence of and the presence alone of the specific tissue model being evaluated, taking the simulation of the initial complete model as the reference model. Subsequently, and sequentially, the isolated effects were simulated on the plantar fascia, short plantar ligament, long plantar ligament and spring ligament maintaining the same load conditions28 in the computing environment. Analysis of each tissue on pronation of the foot was based on the Kite's angle measurement.
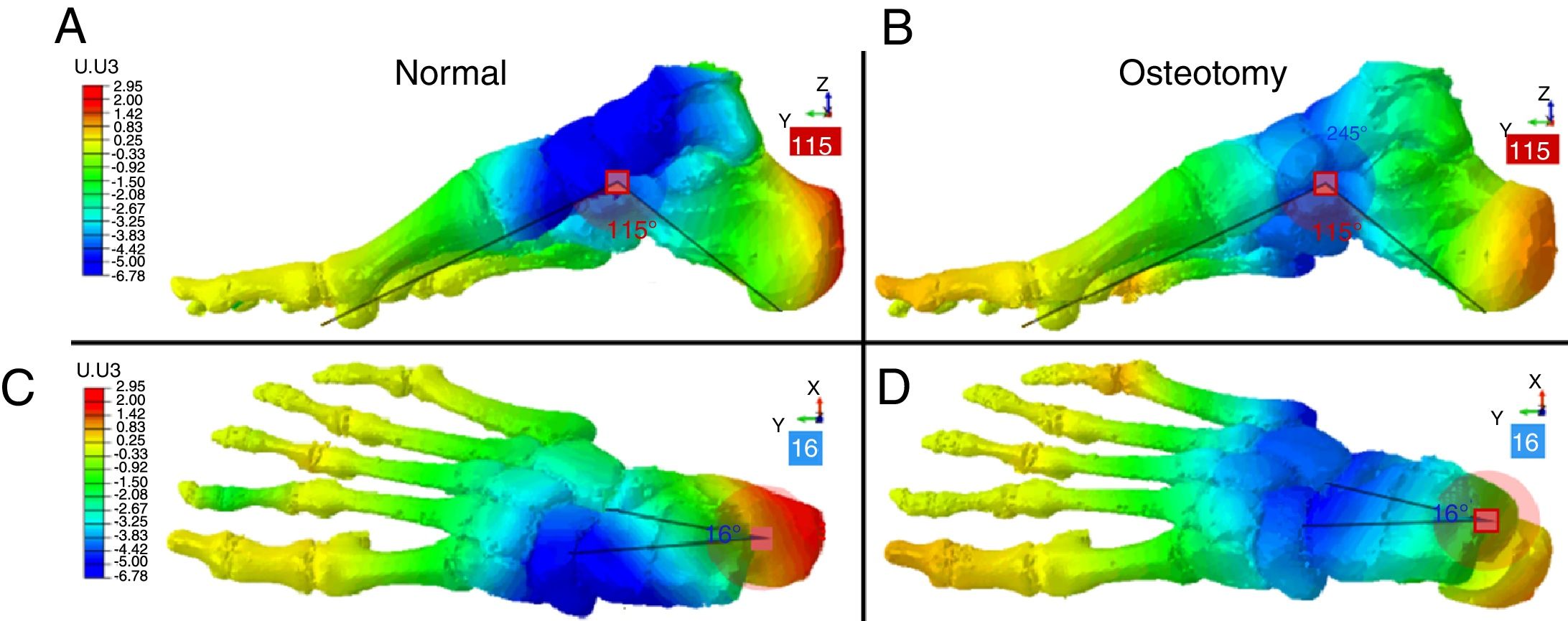
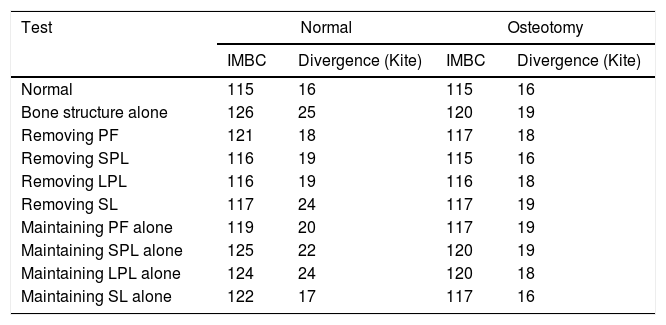
ResultsOf the deformation of the models under loadThe measurements under load conditions of the anatomical and medialised calcaneal model showed deformation in line with the ranges that are considered clinically normal for the IMBC angle (between 115 and 125 degrees), and Kite's angle (between 15 and 20 degrees).
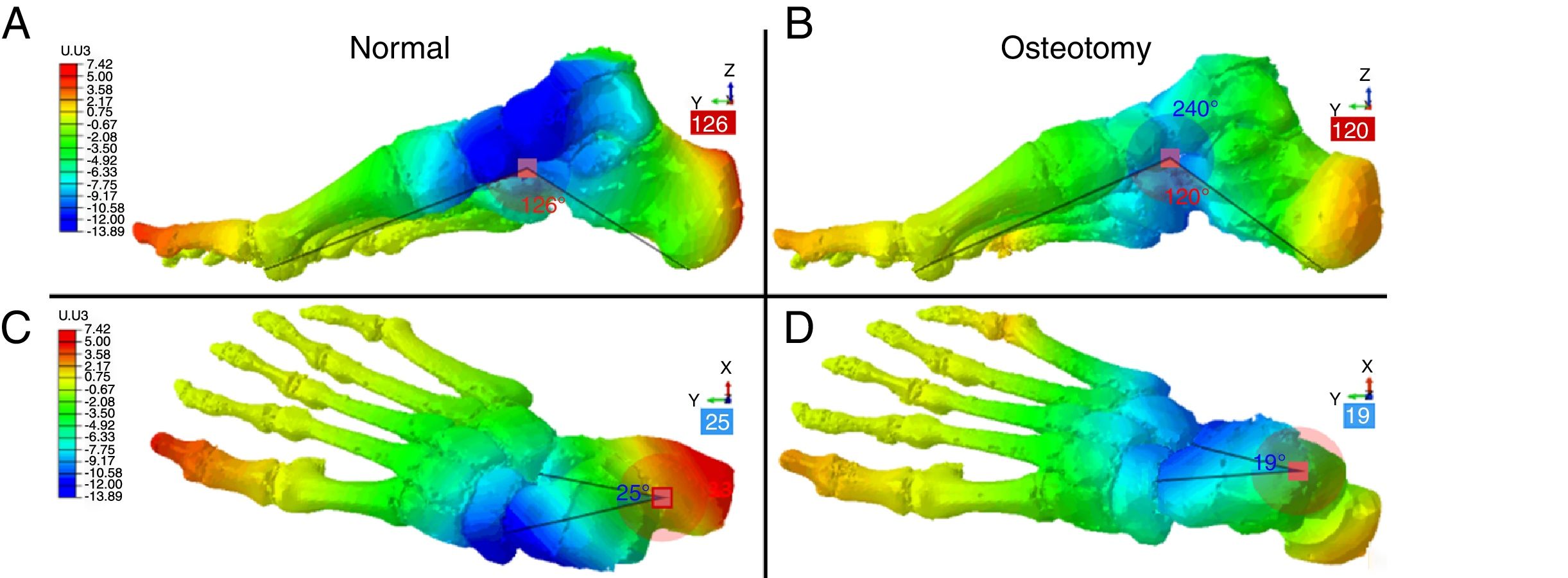
Subtracting all the passive structural support elements of the foot resulted in the maximum deformation values under load of the two models (Fig. 4). For both cases (Figs. 3 and 4), the deformation generated on the vertical axis (Z) was represented, in order to observe the differences in collapse and rotation of the hindfoot inwards (foot in pronation) or outwards (foot in supination).


Maximum deformation obtained on simulating the model maintaining bone structure and cartilage alone. The architecture and geometry of the foot collapses under load in the absence of ligamentous structures. Medialising osteotomy limits this effect and makes the arch more stable. A and B: Costa Bartani angle values; C and D: Kite's angle values.
The IMCB and Kite's angles obtained from each selective stimulation are summarised in Table 2.
Angle values of each selective simulation.
| Test | Normal | Osteotomy | ||
|---|---|---|---|---|
| IMBC | Divergence (Kite) | IMBC | Divergence (Kite) | |
| Normal | 115 | 16 | 115 | 16 |
| Bone structure alone | 126 | 25 | 120 | 19 |
| Removing PF | 121 | 18 | 117 | 18 |
| Removing SPL | 116 | 19 | 115 | 16 |
| Removing LPL | 116 | 19 | 116 | 18 |
| Removing SL | 117 | 24 | 117 | 19 |
| Maintaining PF alone | 119 | 20 | 117 | 19 |
| Maintaining SPL alone | 125 | 22 | 120 | 19 |
| Maintaining LPL alone | 124 | 24 | 120 | 18 |
| Maintaining SL alone | 122 | 17 | 117 | 16 |
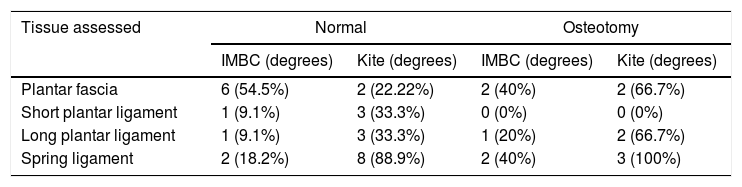
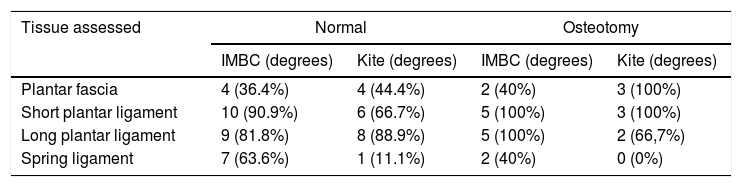
Tables 3 and 4 quantify the effect of each tissue on collapse and flattening of the plantar arch by the numerical difference taking the simulation of the anatomical model under load and the previously obtained maximum deformation values as the benchmark.
Results of the simulations in the absence of each tissue.
| Tissue assessed | Normal | Osteotomy | ||
|---|---|---|---|---|
| IMBC (degrees) | Kite (degrees) | IMBC (degrees) | Kite (degrees) | |
| Plantar fascia | 6 (54.5%) | 2 (22.22%) | 2 (40%) | 2 (66.7%) |
| Short plantar ligament | 1 (9.1%) | 3 (33.3%) | 0 (0%) | 0 (0%) |
| Long plantar ligament | 1 (9.1%) | 3 (33.3%) | 1 (20%) | 2 (66.7%) |
| Spring ligament | 2 (18.2%) | 8 (88.9%) | 2 (40%) | 3 (100%) |
Results of the simulations in the presence of the evaluated tissue alone.
| Tissue assessed | Normal | Osteotomy | ||
|---|---|---|---|---|
| IMBC (degrees) | Kite (degrees) | IMBC (degrees) | Kite (degrees) | |
| Plantar fascia | 4 (36.4%) | 4 (44.4%) | 2 (40%) | 3 (100%) |
| Short plantar ligament | 10 (90.9%) | 6 (66.7%) | 5 (100%) | 3 (100%) |
| Long plantar ligament | 9 (81.8%) | 8 (88.9%) | 5 (100%) | 2 (66,7%) |
| Spring ligament | 7 (63.6%) | 1 (11.1%) | 2 (40%) | 0 (0%) |
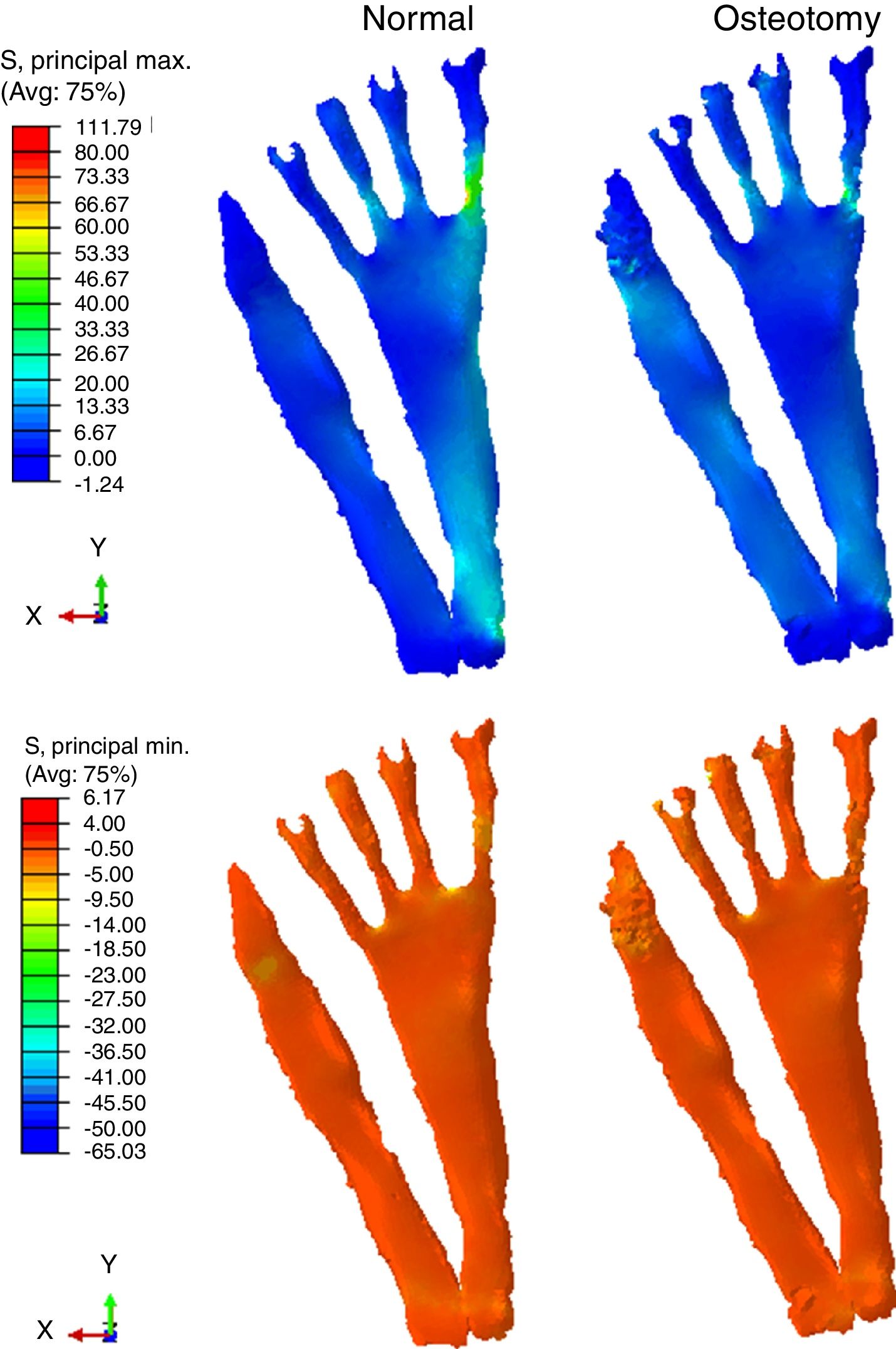
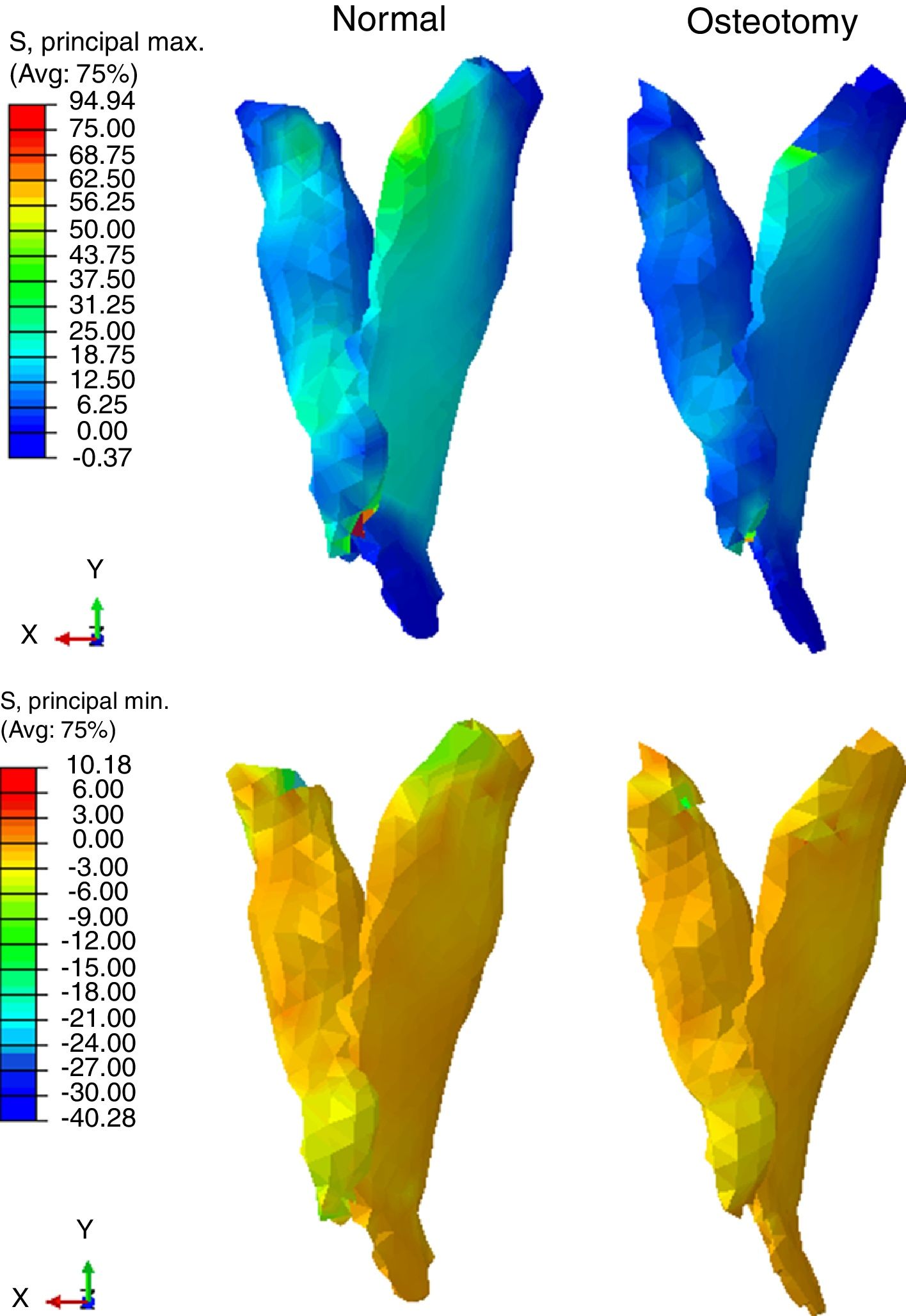
The stress supported by the plantar fascia is shown in Fig. 5 and that supported by the spring ligament in Fig. 6. Each case was assessed using the maximum and minimum principal stresses. These values specific to the engineering of materials are closely linked to the traction stresses (max. principal stress) and compressive stresses (minimum principal stress) supported by the tissues during load. The measurement scale was normalised taking a mean value between both results to correctly observe the differences in each of the cases assessed.
Discussion on the plantar fascia.")
 on the spring ligament complex.")
Our paper's main finding is that the results show a considerable variation in the stress perceived by the plantar fascia and the calcaneonavicular ligament in the foot with the calcaneal medialising osteotomy. We also observed that this procedure on its own reduces and stabilises pronation of the foot.
This article presents the development of a finite element model of a human foot with clear guidance for clinical practice, capable of reproducing the deformation under load of a foot after calcaneal medialising osteotomy, and to simulate different conditions on the soft tissues that passively support the plantar arch, and that are traditionally linked with the development of adult-acquired flatfoot. The versatility of the proposed model enabled assessment of the effect of removing the SPL, LPL, SL and PF, as well as an objective evaluation of the effect of the osteotomy on each of the tissues, and on the anatomical structure of the foot. A clinical approach was used for the evaluation, based on the observation of deformation of the plantar arch and talocalcaneal pronation, the principal signs of adult-acquired flatfoot.
The development of flatfoot affects the plantar arch, which acts to support and buffer human walking, as well as providing the foot a powerful lever that improves gait efficiency.32 From a structural perspective, the plantar arch can be viewed as an architectural truss. These structures enable architects to ensure that roofs can support weight without requiring large support elements. In our model, the plantar fascia and calcaneonavicular ligament are the structures that support the arch and, to a lesser extent, the long and short plantar ligaments. The approaches we took in this study have already been published by various authors based on experimental models, but on healthy feet. The model we propose is capable of reproducing these types of studies and, therefore, can be used as a benchmark to analyse different conditions that are very complex to analyse by means of experimental trials. Furthermore, the development of these types of models will enable research to advance towards more relevant clinical aspects including: the evaluation of complementary surgical alternatives, specific implant designs, and individualised risk prediction tools.
The normal foot and calcaneal medialising osteotomy models benchmark the principal geometric structure, and the contour and load conditions of the model proposed by Morales-Orcajo et al.,13 from the Applied Mechanics and Bioengineering group of the University of Saragossa, Spain. However, only the basic bone structure and the plantar fascia were maintained from this model. This new proposal, adds the geometry of tissues necessary to make a full evaluation of changes to the anatomical plantar structure, and the appropriate conditions for cartilage tissue. In addition, it modifies the structure of the calcaneus, emulating simple medialising osteotomy. This model is the result of collaborative work under the ongoing guidance of clinicians who mechanically validated the tissues analysed.24,28
We consider that the deformity observed under load during the second rocker of gait is valid and appropriate. The results of the deformation of the complete foot model, both normal and after calcaneal osteotomy, coincide with normal clinical values, evaluated in terms of IMCB angle and Kite's angle.33 They provide the necessary clinical validity, and the computational prediction correlates with reality.
Some authors have proposed computational models to evaluate the development of flatfoot and the effect of each tissue on the maintenance of the plantar arch. Gefen,34 and later Cheung,8,35 developed models that enabled evaluation of the biomechanical consequences of complete and partial absence of the plantar fascia. However, they considerably simplify the biomechanical characteristics of the tissues, and their geometry, assuming, among other things, the fascia plantar to be a purely deformable element. This same approach was taken by Smith,17 who proposed a computational model to assess Evans osteotomy. However, it maintains the simplification of the anatomy and the biomechanical characteristics of the tissues.
The proposed model and approach enable evaluation of the relative effect of calcaneal medializing osteotomy on each of the soft tissues that are traditionally linked to the development of adult-acquired flatfoot, respecting the geometry and biomechanical characteristics relevant to each case. The results show that there is a reduction in the stress received by the plantar fascia and the calcaneonavicular ligament on a foot with the calcaneal medialising osteotomy (Figs. 5 and 6). This effect was fundamentally observed on the stresses of traction or stretching generated on the tissue. Furthermore, it was observed that this procedure alone reduces and stabilises pronation of the foot, which could explain the reduction in stress perceived by these tissues. In addition, the model showed that it is precisely these tissues that contribute most to the maintenance of the plantar arch. The results of the simulations show that when the plantar fascia was removed a 40% increase of the IMCB angle was obtained, whereas when the calcaneonavicular or spring ligament was removed, there was an increase of 3 degrees on the talocalcaneal divergence angle (Kite's angle). These results coincide with those of Huang,7 who evaluated the contribution of each tissue experimentally on cadaveric feet. The similarity between this cadaver study and the results obtained by our simulations show the validity of the model's mathematical prediction. On the other hand, a secondary role was observed on maintaining the plantar arch of the short and long plantar ligaments. On simulating the model maintaining only these tissues, results were obtained close to the values generated when maintaining only the bone structure and the cartilages.
Some authors have proposed computational models that seek to evaluate the mechanics of the foot. Wu27 proposed a 2D model that assessed the longitudinal arch of the foot. This model considers a detailed anatomical structure, and a non-linear model for cartilage. This paper was the first approach to evaluate by finite elements the contribution of the plantar ligaments in maintaining the plantar arch. Later, Tao et al.,28 developed a detailed finite element model that assessed the participation of the PF, SL, SPL and LPL in the maintenance of the plantar arch. In contrast to our proposal, these authors do not consider the hyperelastic behaviour of the cartilages, differentiation of cortical and trabecular bone or the appropriate geometry for modelling the tissues assessed. Tao's evaluation is only undertaken in the absence of tissue and complements the evaluation with a study of the pressure differences on the metatarsals. Despite the abovementioned differences in method between the two proposals, the results of the studies coincide in identifying the plantar fascia as the tissue that contributes most in maintenance of the plantar arch, whereas the plantar ligaments play a secondary role.
In this regard it is worth highlighting that the results of our paper show that with an injury or rupture of the SL, there is an increase of 9.1% of plantar arch collapse. This finding places it as the second most important tissue in maintenance of the plantar arch. However, it appears to have a more considerable effect on tarsal pronation of the foot. In the simulation in the absence of the SL, the model showed a variation of 88.9% in Kite's angle, which is reflected in a notable increase in pronation of the foot. These results, therefore, show that the essential contribution of this tissue is the maintenance of the talocalcaneal divergence, rather than on flattening of the foot.
Recently, some authors have considered complex computational models aimed at surgical planning for foot surgery.36,37 However, these proposals maintain morphological and biomechanical considerations of various tissues that are not very close to reality, which notably affects the clinical validity of these proposals. Clinical trials show that the behaviour of both tendons and ligaments is non linear (hyperelastic).13,30 Our model maintains the characterisation of the plant ligaments and SL as elastic-linear elements. However, since this is a static calculation with small displacements and deformations, the error committed is insignificant. The main limitation of our model for clinical use is that it was validated comparing our results with clinical knowledge and with equivalent results in cadaveric experimental models. This limitation is inherent to any experimental numerical model, but at no time invalidates the results obtained. These types of computational representations of biological phenomena enable improved experimentation and understanding in cases where the traditional experimental models are unfeasible or financially unsustainable.
We should also stress the fact that the model is based on a human foot with no mechanical disorder, and therefore we could consider that the results of the stress supported by the soft tissues and the magnitude of the modifying effect of medializing osteotomy can only be correlated in this same circumstance. There is no doubt that with an adult-acquired flatfoot the traction or stretching stresses generated on the tissues could be different, and therefore in order to clinically extrapolate the findings to an adult-acquired flatfoot it would be necessary to provide the numerical model with Young's modulus and Poisson's ratio values under these pathological conditions. Unfortunately there is no published study from which these values can be obtained and this constitutes a suggested future line of research; however we believe that this observation does not qualitatively modify the effect of calcaneal medializing osteotomy on the support structures of the plantar arch.
The computational model that we present in this article contributes new knowledge on the biomechanical representation of the human foot aimed at the evaluation and analysis of the development of adult-acquired flatfoot, as well as the representation of surgical procedures whose effect has not been fully assessed. This model enables the assessment of the effect of calcaneal medializing osteotomy on the structure of the foot and on each soft tissue responsible for supporting the plantar arch and that have traditionally been linked to the development of adult-acquired flatfoot. This inclusion of the geometry of ligaments and tissues, generally ignored by other authors, and the used of biomechanical characteristics based on experimental trials, shows that this proposal is among those closest to reality. The results of this article enable us to conclude, as is guessed in clinical practice, that calcaneal medialising osteotomy reduces stress to the tissues that support the plantar arch, and on its own reduces pronation of the foot. In addition, it confirms the leading role played by the plantar fascia in maintaining the plantar arch, and that of the calcaneonavicular ligament in controlling pronation of the hindfoot.
Level of evidenceLevel of evidence III.
Conflict of interestsThe authors have no conflict of interest to declare.
Please cite this article as: Larrainzar-Garijo R, Cifuentes de la Portilla C, Gutiérrez-Narvarte B, Díez-Nicolás E, Bayod J. Efecto de la osteotomía medializante de calcáneo sobre tejidos blandos de soporte del arco plantar: un estudio computacional. Rev Esp Cir Ortop Traumatol. 2019;63:155–163.
