



The differences between the two main types of fracture of proximal end of the femur, trochanteric and cervical fractures, are still a subject of study, and could be the key to a better understanding of its pathophysiology and prevention. The aim of this study is to determine whether epidemiological differences in the distribution of risk factors associated with hip fracture exist between these two entities.
Patients and methodA descriptive cross-sectional study of 428 patients over the age of 65 admitted for trochanteric or cervical fractures in 2015, in which gender, age, previous diagnosis, external causes associated with fracture and place of the event were recorded.
ResultsThere were 220 patients with a cervical fracture (51.4%) and 208 patients with a trochanteric fracture (48.6%). The average age was higher in the trochanteric fracture, observing a constant increase with age only in women with trochanteric fractures. Cervical fracture showed a significant association with cerebrovascular disease (p=0.039) and trochanteric fracture with accidental falls (p=0.047) and presence of 5–9 previous diseases (p=0.014). A regression analysis maintained this association in the case of a cerebrovascular disease (OR 2.6, 95% CI 1.1–6.4) and the presence of 5–9 diseases (OR 1.5, 95% CI 1.1–2.3).
ConclusionsTrochanteric fractures are associated with women patients of more advanced ages, 5–9 previous diseases and accidental falls. Cerebrovascular disease shows a higher prevalence in cervical fractures.
Las diferencias entre los dos tipos principales de fractura de la extremidad proximal del fémur, trocantérica y cervical, siguen siendo un tema de estudio, pudiendo ser clave para un mejor conocimiento de su fisiopatología y prevención. El objetivo de este trabajo es determinar si existen diferencias epidemiológicas en la distribución de factores de riesgo asociados a la fractura de cadera entre estas dos entidades.
Pacientes y métodoEstudio descriptivo transversal que incluyó 428 pacientes mayores de 65 años ingresados por fractura trocantérica o cervical durante 2015, de los cuales se registraron el sexo, edad, diagnósticos previos, causas externas asociadas a la fractura y lugar del suceso.
ResultadosPresentaron fractura cervical 220 (51,4%) y trocantérica 208 (48,6%) pacientes. La edad media fue superior en la fractura trocantérica, viéndose un aumento constante con la edad únicamente en dicha fractura y en mujeres. La fractura cervical presentó asociación significativa con la enfermedad cerebrovascular (p=0,039) y la fractura trocantérica con la caída accidental (p=0,047) y presencia de 5-9 patologías previas (p=0,014). El análisis de regresión logística mantuvo esta asociación en el caso de enfermedad cerebrovascular (OR 2,6, IC95% 1,1-6,4) y presencia de 5-9 patologías (OR 1,5, IC95% 1,1-2,3).
ConclusionesLa fractura trocantérica se asocia a edades más avanzadas en mujeres, 5-9 patologías previas y caída accidental. La enfermedad cerebrovascular muestra mayor prevalencia en fracturas cervicales.
Hip fracture has a great impact on survival, morbidity and quality of life for those people who suffer from it. It leads to considerable health and social costs and is on the increase in developed countries such as Spain,1 due to the progressive ageing of the population and the close link between these fractures and age. Greater knowledge of these fractures is essential, including its pathophysiology and risk factors, so that effective preventative measures to control this trend maybe put into place.
Proximal femoral fracture (PFF) is a complex pathology the aetiology of which has been associated with multiple risk factors such as advanced age, female gender, Caucasian, physical inactivity, alcohol and tobacco consumption, benzodiazepines, anticonvulsant drugs, cerebrovascular accident, diabetes, osteoporosis, hyperthyroidism and other chronic illnesses.2 However, most studies consider patients with a hip fracture as a homogeneous population without discriminating between the two main types of fracture depending on its anatomical location, trochanteric fractures (extracapsular) and cervical fractures (intracapsular), with increasing proof as to the important differences in risk factors which have an impact on the aetiopathogenesis of these two entities.
Trochanteric fractures are usually associated with elderly patients,3 with previous vertebral fractures and with a lower bone density. There is a greater relationship with osteoporosis,4 to a poor health status prior to the fracture,3 low levels of vitamin D, higher levels of PTH in response to hypovitaminosis D,5 previous cerebrovascular accident6 or tobacco habit.7 Furthermore, cervical hip fractures have been associated with taller8 and heavier9 patients, to a lower raising of PTH in response to hypovitaminosis D, Parkinson's disease,5 oestrogenic therapy,3 high blood pressure, antihypertensive therapy6 and to variations in hip morphology4,9 instead of hip bone density.
All of the above data appear to indicate that trochanteric and femoral neck fractures respond to different pathophysiologic processes, which these risk factors may affect in different ways.
Study objectivesThe main objective of this study was to determine whether there were epidemiologic differences in the distribution of risk factors associated with PFF between trochanteric and cervical fractures in patients admitted to Hospital in 2015, so as to gain a better knowledge of the risk of suffering from a trochanteric or cervical hip fracture and exercise the specific and effective means for its prevention.
The secondary objective of this study was to analysis whether demographic variables such as age and gender or certain life style habits associated with PFF differed between these two entities. We observed whether some of the comorbidities played a more relevant role between the PFF risk factors, and the external causes associated with fracture and the location in which they occurred, and resulted in a higher association with the trochanteric or cervical hip fracture.
Patients and methodSample selectionA descriptive cross-sectional study was conducted. The target population were people over 65 with risk factors associated with proximal femur fractures.
The sample population accessible were patients admitted into hospital during the year 2015 for hip fractures. A total of 489 patients who met with these conditions had been admitted into our hospital
The selected sample comprised those patients older than 65 who had been typified through the CIE-9-MC international classification system of illnesses and lesions as femoral fracture. The following trochanteric fractures were included in the group: those classified as closed intertrochanteric line fractures, major and minor trochanteric fractures, and unspecified fractures (CIE-9-MC 820.20 and 820.21). Also femoral cervical fracture classified as closed intracapsular line fractures, femoral neck fractures or cervical region trochanteric fractures, subcapital region fractures and unspecified closed femoral neck fractures (CIE-9-MC 820.00, 820.03, 820.09 and 820.89).
The exclusion criteria applied were: patients who presented with femoral head of sub-trochanteric fracture, fractures caused by high energy trauma, fractures from traffic accidents, multiple fractures and pathological fractures. A total of 61 patients met with these criteria and were excluded from the study with the final sample consisting of 428 patients.
In the selected sample the following data were recorded: number of medical records, age, gender, data of admittance and discharge, procedures executed, external causes associated with the fracture, place where the fracture occurred and diagnoses in their clinical record typified using the CIE-9-MC classification system.
Study variablesThe dependent variables to contrast were the PFF type: trochanteric or cervical. Independent variables analysed were: age and gender, place where the fracture was located and the causes associated with it. In order to compare previous health status, 0–4, 5–9 or >10 comorbidities were grouped together as they presented on admittance. The specific comorbidities analysed were: high blood pressure (HBP), acute myocardial infarction (AMI), heart failure, cerebrovascular disease (CVD), transient ischaemic attack, diabetes mellitus type 2 (DM 2), hyperlipidaemia, osteoporosis, previous vertebral fracture, Alzheimer's disease, Parkinson's disease, depression, organic psychosis, chronic obstructive pulmonary disease (COPD), ashma, chronic kidney failure, problems of vision and hypothyroidism. Lifestyle factors analysed were overweight and obesity, tobacco abuse and a personal tobacco habit, admittance to an old peoples’ home, being bedridden and physical limitation.
Statistical analysisFor statistical analysis, quantitative variables were expressed as mean±standard deviation and qualitative data as absolute frequencies and percentages. The exact Fisher test was used to contrast the dichotomic variables and the Student's t-test for the continuous variables. To compare the variation of the incidence of both types of fracture with age, the sample was divided into intervals of 65–75, 76–85 and >85 years and the χ2 test was used. For a less biased calculation of the relationship between the dependent variable (fracture type) and independent variables which had shown a statistically significant association, they were included in a multivariate logistic regression study together with other possible factors of confusion such as gender and age. Differences were considered to be statistically significant with a value of p<0.05. The statistical package SPSS 23.0 and the software GraphPad QuickCalcs10 were used to analyse data.
ResultsDistribution of the dependent variableOf the 428 patients admitted for PFF included in the study, 208 (48.6%) presented with a trochanteric fracture, of which 204 were described as closed trochanteric line fractures and 4 as closed intertrochanteric line fractures. Also, 220 patients (51.4%) presented with a transcervical fracture, out of which 154 were described as closed femoral neck fractures, 28 as closed transcervical neck base fractures, 37 as other closed transcervical fractures and 1 as a closed transcervical fracture of unspecified intracapsular line.
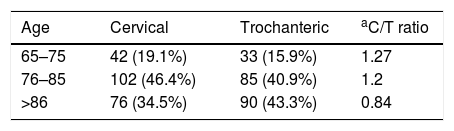
Correlation between the type of fracture and the demographic variables such as age and genderThe mean age of the sample population was 82.74. In the case of the trochanteric fracture the mean age of presentation (83.4±7.2) was higher to that presented by cervical fractures (82.1±7.5), although this difference was not statistically significant (p=0.073). Table 1 shows the distribution of both types of fracture according to age in intervals of 65–75, 76–85 and >85, without showing any significant differences between both fractures. It may be observed that, in the case of the femoral neck fractures, the maximum incidence was present in the age group of 76–85, being less in more advanced ages, whilst in the case of the trochanteric fractures there is a constant increase of the incidence as age increases.
Distribution of trochanteric and cervical hip fractures by age of the population under study.
| Age | Cervical | Trochanteric | aC/T ratio |
|---|---|---|---|
| 65–75 | 42 (19.1%) | 33 (15.9%) | 1.27 |
| 76–85 | 102 (46.4%) | 85 (40.9%) | 1.2 |
| >86 | 76 (34.5%) | 90 (43.3%) | 0.84 |
The data are expressed as absolute frequencies (of each group).
With regard to patient gender, 112 (26.2%) were male, whilst 315 (73.6%) were female and the gender of one patient was not recorded. The predominance of females was similar in both cervical (74.5%) and trochanteric fractures (72.6%).
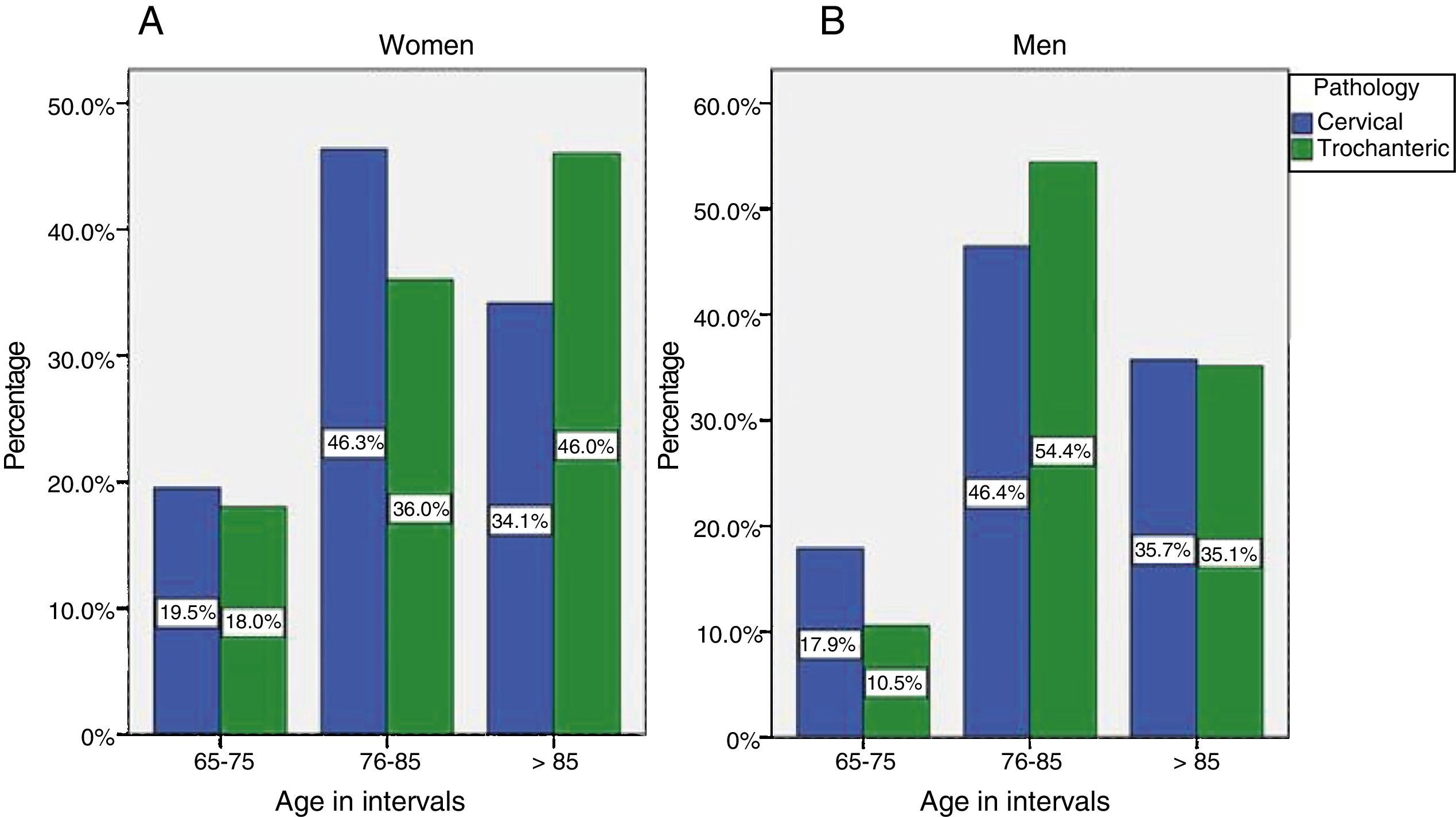
On analysing the distribution of both types of fracture with regards to gender and age, we found there was a tendency towards women (Fig. 1), observing greater incidence of trochanteric fractures as age progressed, with the highest percentage of trochanteric fractures occurring in patients over 85, whilst in the case of femoral neck fractures, the group aged 76–85 years predominated. In the males this progression with age was not observed, in either trochanteric fractures or cervical fractures, with there being a higher incidence of both fractures in the age group between 76 and 85 years.
Analysis of external associated causes and place of fracture occurrence and men (B) within each age interval.")
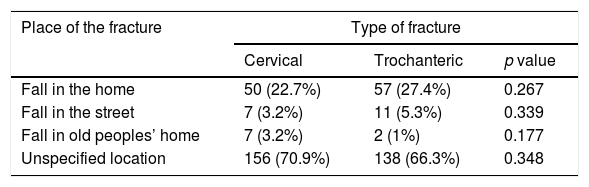
Table 2 contains the associated external causes to the main event, i.e. the type of PFF. No differences were observed between both types of fracture with regard to the place in which they occurred (home, old peoples’ home, street of unspecified location).
place in which the cervical and trochanteric hip fractures took place in the study sample.
| Place of the fracture | Type of fracture | ||
|---|---|---|---|
| Cervical | Trochanteric | p value | |
| Fall in the home | 50 (22.7%) | 57 (27.4%) | 0.267 |
| Fall in the street | 7 (3.2%) | 11 (5.3%) | 0.339 |
| Fall in old peoples’ home | 7 (3.2%) | 2 (1%) | 0.177 |
| Unspecified location | 156 (70.9%) | 138 (66.3%) | 0.348 |
Data are expressed as absolute frequencies (percentage of each group).
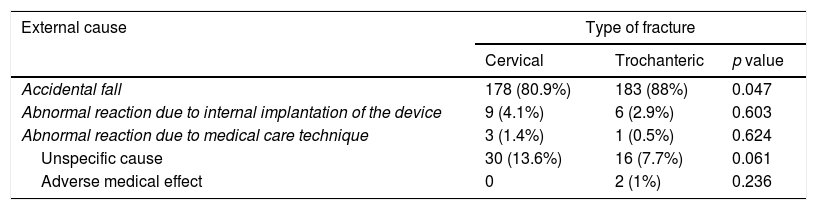
Table 3 contains the causes associated with the fracture. Accidental fall is associated significantly with trochanteric fractures (p=0.047) whilst no differences were observed in those caused by an abnormal reaction from the implantation of an internal device, medical care, adverse effects to drugs or unspecified causes.
External cause associated with cervical and trochanteric hip fractures in study sample.
| External cause | Type of fracture | ||
|---|---|---|---|
| Cervical | Trochanteric | p value | |
| Accidental fall | 178 (80.9%) | 183 (88%) | 0.047 |
| Abnormal reaction due to internal implantation of the device | 9 (4.1%) | 6 (2.9%) | 0.603 |
| Abnormal reaction due to medical care technique | 3 (1.4%) | 1 (0.5%) | 0.624 |
| Unspecific cause | 30 (13.6%) | 16 (7.7%) | 0.061 |
| Adverse medical effect | 0 | 2 (1%) | 0.236 |
The data were expressed as absolute frequencies (percentage of each group).
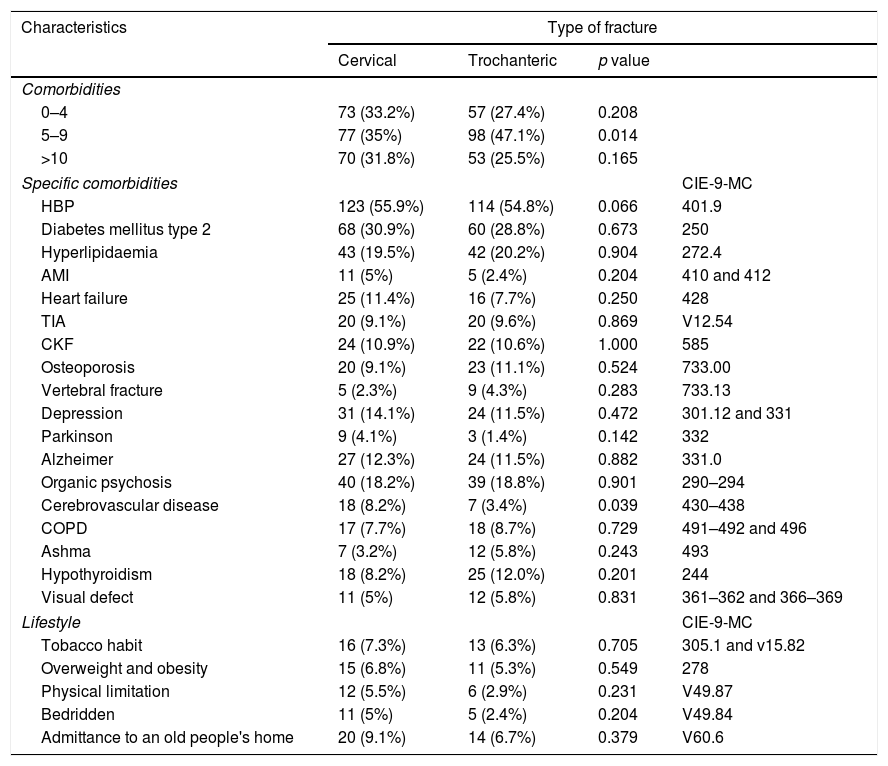
Table 4 presents the analysis of the pathologies and lifestyle associated with PFF, an association was only observed between trochanteric fractures and the group with 5–9 previous comorbidities (p=0.014). Cerebrovascular disease presented with a prevalence which was significantly higher in those patients with femoral neck fracture (p=0.039); the remainder of neurological and psychiatric pathologies analysed were not statistically significant, although almost all of them had greater prevalence in patients with cervical hip fracture, especially in Parkinson's disease. The prevalence of cardiovascular risk factors (HBP, DM and hypolipidaemia) was very similar in both groups, although the cardiovascular pathologies and the AMI or heart failure presented with higher prevalence in patients with cervical hip fractures. In contrast, pathologies such as an osteoporosis, vertebral fractures, asthma or hypothyroidism were more prevalent in the population with trochanteric hip fractures, without there being any significant association there. Neither was there any statistically significant association observed between the type of fracture and a tobacco habit, physical limitation, being bedridden or being admitted to an old peoples’ home.
Comorbidities and lifestyle of patients with cervical and trochanteric hip fractures in study sample.
| Characteristics | Type of fracture | |||
|---|---|---|---|---|
| Cervical | Trochanteric | p value | ||
| Comorbidities | ||||
| 0–4 | 73 (33.2%) | 57 (27.4%) | 0.208 | |
| 5–9 | 77 (35%) | 98 (47.1%) | 0.014 | |
| >10 | 70 (31.8%) | 53 (25.5%) | 0.165 | |
| Specific comorbidities | CIE-9-MC | |||
| HBP | 123 (55.9%) | 114 (54.8%) | 0.066 | 401.9 |
| Diabetes mellitus type 2 | 68 (30.9%) | 60 (28.8%) | 0.673 | 250 |
| Hyperlipidaemia | 43 (19.5%) | 42 (20.2%) | 0.904 | 272.4 |
| AMI | 11 (5%) | 5 (2.4%) | 0.204 | 410 and 412 |
| Heart failure | 25 (11.4%) | 16 (7.7%) | 0.250 | 428 |
| TIA | 20 (9.1%) | 20 (9.6%) | 0.869 | V12.54 |
| CKF | 24 (10.9%) | 22 (10.6%) | 1.000 | 585 |
| Osteoporosis | 20 (9.1%) | 23 (11.1%) | 0.524 | 733.00 |
| Vertebral fracture | 5 (2.3%) | 9 (4.3%) | 0.283 | 733.13 |
| Depression | 31 (14.1%) | 24 (11.5%) | 0.472 | 301.12 and 331 |
| Parkinson | 9 (4.1%) | 3 (1.4%) | 0.142 | 332 |
| Alzheimer | 27 (12.3%) | 24 (11.5%) | 0.882 | 331.0 |
| Organic psychosis | 40 (18.2%) | 39 (18.8%) | 0.901 | 290–294 |
| Cerebrovascular disease | 18 (8.2%) | 7 (3.4%) | 0.039 | 430–438 |
| COPD | 17 (7.7%) | 18 (8.7%) | 0.729 | 491–492 and 496 |
| Ashma | 7 (3.2%) | 12 (5.8%) | 0.243 | 493 |
| Hypothyroidism | 18 (8.2%) | 25 (12.0%) | 0.201 | 244 |
| Visual defect | 11 (5%) | 12 (5.8%) | 0.831 | 361–362 and 366–369 |
| Lifestyle | CIE-9-MC | |||
| Tobacco habit | 16 (7.3%) | 13 (6.3%) | 0.705 | 305.1 and v15.82 |
| Overweight and obesity | 15 (6.8%) | 11 (5.3%) | 0.549 | 278 |
| Physical limitation | 12 (5.5%) | 6 (2.9%) | 0.231 | V49.87 |
| Bedridden | 11 (5%) | 5 (2.4%) | 0.204 | V49.84 |
| Admittance to an old people's home | 20 (9.1%) | 14 (6.7%) | 0.379 | V60.6 |
HBP: high blood pressure; AMI: acute myocardial infarction; TIA: transient ischaemic attack; CKF: chronic kidney failure; COPD: chronic obstructive pulmonary disease.
The data are expressed as absolute frequencies (percentage of each group).
Variables which showed a significant association were regarded as independent, i.e. the cerebrovascular disease, present in 5–9 previous pathologies and accidental falls as a cause of fracture, along with other variables which could have conditioned the relationship between these factors and fracture type, such as gender and age. The SCS variable was associated with suffering from a cervical fracture (p=0.046 OR 2.6, 95% CI 1.1–6.4) and the trochanteric fracture present in 5–9 pathologies (p=0.043 OR 1.5, 95% CI 1.1–2.3), i.e. having SCS increase more than double the probability of suffering from a cervical fracture instead of a trochanteric one and presenting with 5–9 pathologies increasing by 1.5 times the probability of suffering from a trochanteric fracture instead of a cervical fracture in the study sample.
DiscussionHip fracture is priority health problem and alone may lead to up to five times an increase in mortality in men and three times in women during the first year, with a significantly higher morality in comparison with the general population of up to 12 years after the fracture.11 Many authors defend the need to analyse the main types of PFF, trochanteric fractures and cervical fractures separately, for better knowledge of their pathophysiology although on occasions the results obtained in these studies differ to one another, thus emphasising the need for new studies to address this issue. For this reason, our objective was to analyse whether differences existed in our population in the factors associated with hip fracture between these two types of fracture, for a better risk assessment and approach to their prevention.
Several recent studies claim that trochanteric fracture is associated with more advanced age than cervical fracture.3,12 However, in our study although the mean age was higher in the group of patients withtrochanteric fracture, this association was not statistically significant and our result was similar to that obtained by Stewart et al.6 in their study. One possible cause of this was the lower sample in our study (n=428) and that previously mentioned (n=310)6 in comparison to the studies of Fox et al.3 (n=923) and Fisher et al.12 (n=761), where this association was established. Despite this, we did find there was relationship between trochanteric fractures and more advanced ages, with the incidence of trochanteric fractures becoming progressively greater in older groups, together with the inversion of the C/T ratio, progressing from 1.27 in the youngest group (65–75 years of age), to 0.85 in those over 85. This relationship may be attributed to the bone loss occurring with age, to which the trochanteric femoral area is more susceptible, due to a greater quantity of trabecular bone (70–90%), compared with the structure of the femoral neck, with a greater quantity of cortical bone. The fracture of this region is associated with other factors less connected with age or bone density, such as greater length or less width of the femoral neck, or a greater angle in the femoral neck axis.4
Analysis of the influence of gender in both types of fracture shows that there is a progressive increase in the incidence of trochanteric fractures with age in women, a phenomenon that was not observed in men, in keeping with previous literature.13 This greater risk of suffering from a trochanteric fracture instead of a cervical fracture in advanced ages in women may be a reflection of the greater loss of the trabecular bone with age in this gender compared to that in men, which may be influenced by greater bone exchange or a turn-over of the trabecular bone, making it more sensitive to hormonal and metabolic factors and therefore to the oestrogen deficit which is associated with ageing in women.9
Trochanteric fractures have been associated with patients who suffer from a previously worse health status. One example of this is the study by Fox et al.3 in which this fractures significantly associated with a greater number of comorbidities (>4). In our study a significant association was observed between trochanteric fractures and the group of patients who presented with 5–9 associated comorbidities (p=0.014), whilst there was no association as was expected in the group of patients with >10 comorbidities. Analysis of specific pathologies present in the three groups establishes according to the number of comorbidities revealed that all had a very similar frequency in both types of fracture save that of osteoporosis, which in the group of 5–9 comorbidities was far higher than in patients withtrochanteric fractures than in those with cervical fractures, and as a result only this group of 5–9 comorbidities was significantly associated with trochanteric fractures and not the group with >10 pathologies, which, a priori, would present with a worse health status and greater fragility.
Due to the larger quantity of trabecular bone presenting in the trochanteric region fractures in this area have as standard practice been related to a more osteoporotic bone and with previous vertebral fractures,4,9 due to the similar bony composition of the vertebra, but our findings do not enable us to support or refute this theory. Although both the diagnosis of osteoporosis and vertebral fractures were more frequent in the trochanteric fractures, it was not possible to establish a significant relationship. This could be due to the comparison only being for established diagnoses of osteoporosis in both groups instead of comparing BMD (mineral bone density) levels as was carried out in other studies4,6,9 which did show signficiantly lower levels in patients with trochanteric. fractures
Another pathology associated with greater risk of hip fracture is cerebrovascular accident. However, few articles analysed its specific association with each type of hip fracture and none of the previous studies revealed this association between cerebrovascular disease and cervical hip fracture. In contrast, other studies such as that by Stewart et al.6 established the opposite relationship with the trochanteric fracture, justifying this relationship with a more violent fall, duet the lack of response of defence to the fall associated with stroke.
The findings obtained on analysis of risk factors of hip fracture associated with lifestyle concur with previous studies in that significant differences were found between these factors and both types of fracture.5,12 Other studies such as that of Määttä et al7 did establish an association between tobacco habit and the trochanteric fracture due to the possible interaction of tobacco with bone metabolism, although the study itself refers to the fact that this association was limited by the small number of trochanteric (n=31) and cervical fractures (n=49).
One findings of interest was the clear predominance of the home as the place where both fractures took place. This may be due to the advanced age and greater fragility of the sample studied meant that they spend more time in the home. This could be of interest for future studies when risk factors associated specifically to the home are analysed, although these findings should be cautiously interpreted as the place of fall was not specified in a high percentage of both types of fracture.
The study of external associated causes showed a relationship between accidental fall and trochanteric fracture (p=0.047), which makes sense if we consider that this is a patient group which, as already commented upon above, was elderly and had bone fragility. On absorbing the fall in the trochangeric region (the trochanter mayor is the place which most frequently receives the impact in the elderly) the fracture at this level would be provoked unlike with stronger bones, where the energy of the impact may be transferred to a femoral cervical region,4 although the higher percentage of non specific causes in cervical fractures could be a possible factor to bear in mind when interpreting this study.
Study limitationsOur study has certain limitations. As it is a transversal study, it is not possible to establish causal relations between the comorbidities and fracture type. Variables such as BMI, BMD, and geometry of the treated hip were not included in the study and may affect the type of PFF. The data base used did not collect data on tobacco consumption or the degree of physical limitation. Other factors such as alcoholism, hyperthyroidism or hypovitaminosis D were not able to be included due to their low prevalence in the selected sample. Nor were we able to rule out the possible interaction of other non assessed comorbidities although to reduce this possible error those which are usually associated with risk factors of hip fractures were included and others in previous comparatives studies similar to our own.
ConclusionsTrochanteric fractures present in more advanced ages in women than in men.
In the case of trochanteric fractures there is a higher association with accidental falls as the cause of the fracture.
In the group of trochanteric fractures there is an association with the presence of 5–9 previous comorbidities on admittance.
Cerebrovascular disease is significantly associated with femoral neck hip fractures compared with those located in the trochanteric region.
Level of evidenceLevel of evidence IV.
Ethical liabilitiesHuman and animal protectionThe authors declare that no experiments have been performed on humans or animals for this investigation.
Data confidentialityThe authors declare they have adhered to the protocol of their centre of work on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestThe authors have no conflict of interest to declare.
Please cite this article as: Díaz AR, Navas PZ. Factores de riesgo en fracturas de cadera trocantéricas y de cuello femoral. Rev Esp Cir Ortop Traumatol. 2018;62:134–141.
