





Gastric emptying scintigraphy is used to assess patients with symptoms of dyspepsia or gastroparesis. An alteration of fundus accommodation may explain these symptoms. The aim of this study was to determine the accommodation in gastric emptying scintigraphy studies performed in our institution.
Material and methods50 patients (43 children) referred for gastric emptying assessment were evaluated. After fasting for 8 h, and following international guidelines, egg labeling was performed with 37 mBq of [99mTc]Tc-DTPA and administration of standardized food. Areas of interest were defined in the stomach at different times, and the corresponding retention percentages were calculated. Considering the image at time zero, gastric accommodation was qualitatively and quantitatively assessed, calculating the ratio between proximal stomach counts and total counts.
ResultsOf the 50 patients studied, 32 had normal emptying, 10 had slowed emptying and 8 had accelerated emptying. Within the group of patients with normal emptying, 8 had altered accommodation (25%) and another 8 in the group with abnormal emptying (44%). Applying the ROC curve analysis to quantitative values, the most appropriate cut-off value was 0.785 with p < 0.001, sensitivity 82.4% and specificity 100%.
ConclusionGastric emptying scintigraphy in addition to determining motility, made it possible to assess both qualitatively and quantitatively the distribution of the radiotracer in the stomach and thus, indirectly, the accommodation in the fundus. It provided added diagnostic information in a simple manner, without protocol changes and allowing more specific treatments to be assessed.
La gammagrafía de vaciamiento gástrico se utiliza para valorar pacientes con síntomas de dispepsia o gastroparesia. Una alteración de la acomodación del fundus puede explicar estos síntomas. El objetivo del estudio fue determinar la acomodación en los estudios gammagráficos de vaciamiento gástrico realizados en nuestra institución.
Material y métodosSe valoraron 50 pacientes (43 niños) remitidos para la valoración del vaciamiento gástrico. Tras ayuno de 8 horas, y siguiendo guías internacionales, se realizó el marcaje del huevo con 37 mBq de [99mTc]Tc-DTPA y administración de comida estandarizada. Se definieron áreas de interés en estómago a diferentes horas, calculándose los porcentajes de retención correspondientes. Considerando la imagen a tiempo cero, se valoró cualitativa y cuantitativamente la acomodación gástrica, calculándose el cociente entre las cuentas en estómago proximal y las cuentas totales.
ResultadosDe los 50 pacientes estudiados, 32 presentaban vaciamiento normal, 10 enlentecido y 8 acelerado. Dentro de grupo de pacientes con vaciamiento normal, 8 presentaban alteración en la acomodación (25%) y otros 8 dentro del grupo con vaciamiento anormal (44%). Aplicando el análisis de la curva ROC a los valores cuantitativos, el valor de corte más adecuado fue 0.785 con p < 0.001, sensibilidad 82.4% y especificidad 100%.
ConclusiónEl estudio gammagráfico de vaciamiento gástrico, además de determinar la motilidad, permitió valorar tanto cualitativa como cuantitativamente la distribución del radiotrazador en el estómago y, con ello, de manera indirecta la acomodación en fundus. Proporcionó información diagnóstica añadida de manera sencilla, sin cambios de protocolo y permitiendo valorar tratamientos más específicos.
Digestive disorders such as dyspepsia or gastroparesis are frequent in clinical practice and constitute an important healthcare problem that carries significant resource consumption. Gastric emptying scintigraphy is routinely used to assess these disorders. However, many symptomatic patients present a normal isotopic study.1 Therefore, there is increasing interest in obtaining greater information on the role of fundic accommodation in the origin of the symptoms of dyspepsia.
Gastric accommodation was first described by Cannon and Lieb in 1911 and consists in a postprandial reflex that produces a reduction in gastric tone. In this way, the fundus becomes a food reservoir without a significant increase in intragastric pressure. It has been reported that evaluation of gastric accommodation contributes to explaining the symptoms of dyspepsia not clarified by conventional scintigraphy.2
At present, the gastric barostat test is considered the most adequate method for studying gastric accommodation. Nevertheless, it is an invasive procedure, which can alter gastric physiology and is not always available.3 Intragastric food distribution (IFD) is defined as a measure of the quantity of food found in the proximal stomach compared with that found throughout the viscera. Scintigraphic determination of IFD immediately after food intake is an indirect method to evaluate fundic accommodation.4
The aim of this study was to determine both the qualitative and quantitative clinical utility of fundic accommodation in gastric emptying scintigraphy studies performed at our institution.
Material and methodsPatients studiedWe performed a retrospective study including patients referred to our department from October 2018 to October 2022 for evaluation of dyspepsia by gastric emptying scintigraphy. The study was approved by the Bioethical Commission of the university to which our center belongs. The symptomatology of the patients included some or part of the following symptoms: abdominal pain, nausea, vomiting, diarrhea, constipation, weight loss, failure to thrive, regurgitation, excessive eructation, pyrosis and early satiety. Data collection on the evolution of the patients finished in October 2023.
Of a total of 64 studies, 14 were ruled out for presenting tracer activity outside the stomach in the basal image. Thus, the study group was made up of 50 patients.
Scintigraphic studyThe gastric emptying scintigraphy study was performed following the consensus guidelines published by the Society of Nuclear Medicine and the American Neurogastroenterology and Motility Society.5 For study preparation, the patients were requested to fast for 8 h, discontinue medication that could interfere with the study (prokinetics, analgesics, opiates) during the three days prior to the study and not smoke the day of the study. In diabetic patients, the level of glycemia was determined and should be less than 200 mg/dL.
Egg labeling was performed with 37 mBq de [99mTc]Tc-DTPA, administering a standard meal (egg omelette, two slices of bread, 30 g of jam, a slice of York ham, and 120 mL of water). Patients were asked to eat the meal within a maximum period of 10 min. Planar images centered on the abdomen were acquired (matrix 128 × 128, anterior and posterior, of 2 min) immediately after the meal and at 30 min and at 1, 2, and 3 h. The images were acquired using three dual head gamma cameras Millennium VG® and NM/CT 870 DR (both from GE Healthcare, Milwaukee, USA) and one Symbia T2® (Siemens, Erlangen, Germany), with low energy collimators and a window of 20% centered on a photopeak of 140 keV. The study was well tolerated by all the patients.
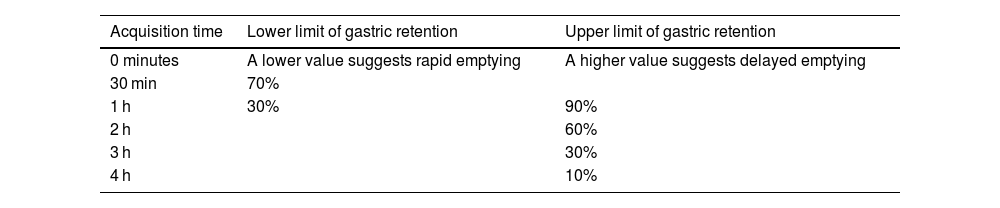
Image processing and evaluationWe manually defined areas of interest in the stomach for each acquisition time according to the previously mentioned international guidelines and using a Xeleris® (GE Healthcare) processing station. The values of normality used for gastric emptying were those described in the guidelines (Table 1).
Gastric accommodation was qualitatively and quantitatively evaluated considering the image at time zero. The first was performed according to that used in previous publications and based on 5 grades.4 Grade 1 corresponded to clearly altered accommodation, grade 2 was probably altered accommodation, grade 3 was possibly altered, grade 4 was probably normal and grade 5 was clearly normal. Posteriorly, these grades were grouped into two groups: altered accommodation (grades 1, 2 and 3) and normal accommodation (grade 4 and 5). Quantitative evaluation by IFD determination was performed generating areas of interest for the proximal portion of the stomach and for all the viscera and calculating the quotient between the two areas. For the latter localization, the stomach was divided into two equal parts using the middle point of the longitudinal axis of the viscera (Fig. 1).

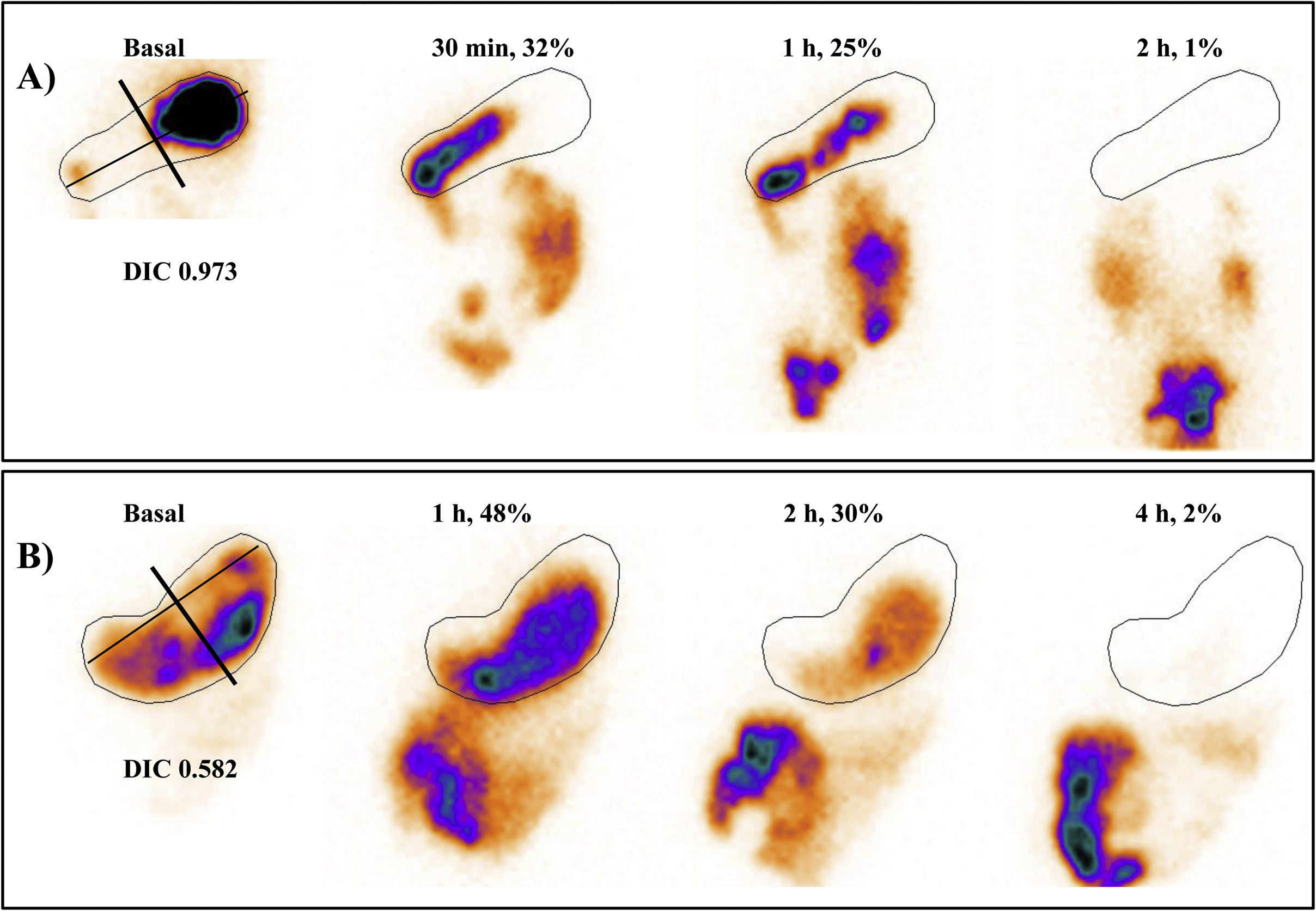
Scintigraphic evaluation of accommodation in the basal image as well as gastric emptying.
A. Study of a 14-year-old girl with a definitive diagnosis of functional dyspepsia. Both the qualitative and the quantitative evaluation were compatible with fundic accommodation within normality. Gastric emptying showed values compatible with rapid emptying.
B. Study of a 12-year-old boy diagnosed with food intolerance, with a scintigraphic result of altered accommodation and normal emptying.
Only the images acquired in anterior projection at different hours, the IFD value and the percentage of retention are shown.
Two nuclear medicine physicians with experience in gastrointestinal studies jointly carried out the processing and interpretation of the studies.
Patient follow-upThe electronic clinical histories allowed consulting the definitive diagnosis of each patient in the study. Data collection on the evolution of the patients finished in October 2023.
Statistical analysisThe data collected were analyzed with the SPSS® version 22 statistical program (IBM, New York, USA). The Kolmogorov-Smirnov test was used to assess the normality of distribution of the parameters.
Comparison of variables was performed with the Mann-Whitney U and Kruskal-Wallis tests in the case of quantitative variables and with the Chi-square test for categorical variables. The Spearman test was used to study correlations among parameters. The most appropriate cut-off and area under the curve (AUC) of the IFD were determined by analysis of the receiver operating characteristic (ROC) curve and the application of the Youden index.
The values found were expressed as median and range for numerical variables and as frequency and percentage in the case of categorical variables. A result was considered statistically significant with a p value < 0.05.
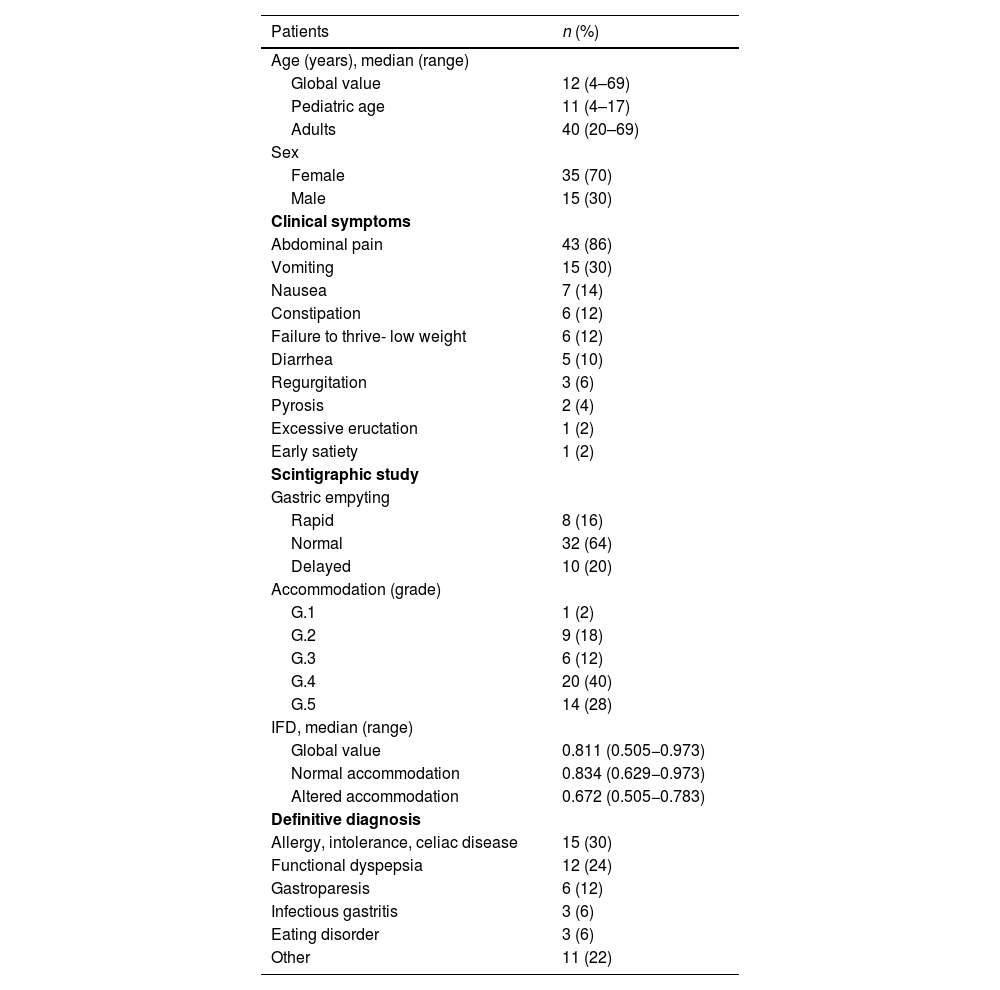
ResultsPatients studiedTable 2 shows the characteristics of the patients studied as well as the clinical symptoms reported. According to age, 43 patients were children (4–17 years old) and 7 were adults (20–69 years of age). Most were females. The most frequent symptom reported by the patients was abdominal pain (86% of the cases), followed by vomiting and nausea. The definitive diagnoses in more than half of the cases were related to allergies, intolerances and celiac disease and functional dyspepsia. In the other group of patients the diagnoses included eosinophilic esophagitis, gastroesophageal reflux, dumping, abdominal migraine, colon disease, functional constipation and functional diarrhea, with each diagnosis being made in a scarce number of patients.
Characteristics of the patients, clinical symptoms, scintigraphy results and definitive diagnosis.
| Patients | n (%) |
|---|---|
| Age (years), median (range) | |
| Global value | 12 (4–69) |
| Pediatric age | 11 (4–17) |
| Adults | 40 (20–69) |
| Sex | |
| Female | 35 (70) |
| Male | 15 (30) |
| Clinical symptoms | |
| Abdominal pain | 43 (86) |
| Vomiting | 15 (30) |
| Nausea | 7 (14) |
| Constipation | 6 (12) |
| Failure to thrive- low weight | 6 (12) |
| Diarrhea | 5 (10) |
| Regurgitation | 3 (6) |
| Pyrosis | 2 (4) |
| Excessive eructation | 1 (2) |
| Early satiety | 1 (2) |
| Scintigraphic study | |
| Gastric empyting | |
| Rapid | 8 (16) |
| Normal | 32 (64) |
| Delayed | 10 (20) |
| Accommodation (grade) | |
| G.1 | 1 (2) |
| G.2 | 9 (18) |
| G.3 | 6 (12) |
| G.4 | 20 (40) |
| G.5 | 14 (28) |
| IFD, median (range) | |
| Global value | 0.811 (0.505−0.973) |
| Normal accommodation | 0.834 (0.629−0.973) |
| Altered accommodation | 0.672 (0.505−0.783) |
| Definitive diagnosis | |
| Allergy, intolerance, celiac disease | 15 (30) |
| Functional dyspepsia | 12 (24) |
| Gastroparesis | 6 (12) |
| Infectious gastritis | 3 (6) |
| Eating disorder | 3 (6) |
| Other | 11 (22) |
IFD: intragastric food distribution.
Of the 50 patients studied, 8 presented a scintigraphy compatible with rapid emptying, 32 had studies within normality and 10 showed delayed emptying. For qualitative evaluation of the accommodation, the most frequent grade described was grade 4 (40%) followed by grade 5 (28%). Altered accommodation (grades 1, 2 and 3) made up 32% of the studies. In regard to quantitative evaluation, the IFD values were lower in patients with altered accommodation (Table 2).
Table 3 shows the distribution of the accommodation studies in relation to the gastric emptying scintigraphy. Eight (25%) of the 32 patients with normal emptying presented altered accommodation. Of the 18 patients with abnormal emptying (rapid or delayed), 8 showed equally altered accommodation, constituting 44% of the patients.
Table 4 shows the results of the scintigraphic study and the symptoms most frequently found in the 3 most numerous diagnostic groups. A significant number of patients in each group presented altered accommodation. Delayed emptying was very frequent in gastroparesis and abdominal pain was a major symptom.
Scintigraphic findings and the most frequent symptoms in the three most numerous diagnostic groups. Values expressed as percentage.
| Accommodation | Gastric empyting | Symptoms | ||||||
|---|---|---|---|---|---|---|---|---|
| Definitive diagnosis | Altered | Normal | Delayed | Rapid | Normal | Pain | Vomiting | Nausea |
| Allergies, intolerance, celiac | 47 | 53 | 7 | 27 | 66 | 80 | 50 | 13 |
| Functional dyspepsia | 25 | 75 | 17 | 25 | 58 | 83 | 33 | 17 |
| Gastroparesis | 33 | 67 | 83 | 0 | 17 | 100 | 34 | 17 |
On comparison of the patients with altered versus normal accommodation, significant differences were found in the IFD values (Mann-Whitney U test, p < 0.001). On applying the ROC curve analysis to the IFD values, the most adequate cut-off for differentiating between altered and normal accommodation was 0.785, with an AUC of 0.930 (0.861−0.999), p < 0.001, and values of sensitivity of 82.4% and specificity of 100%.
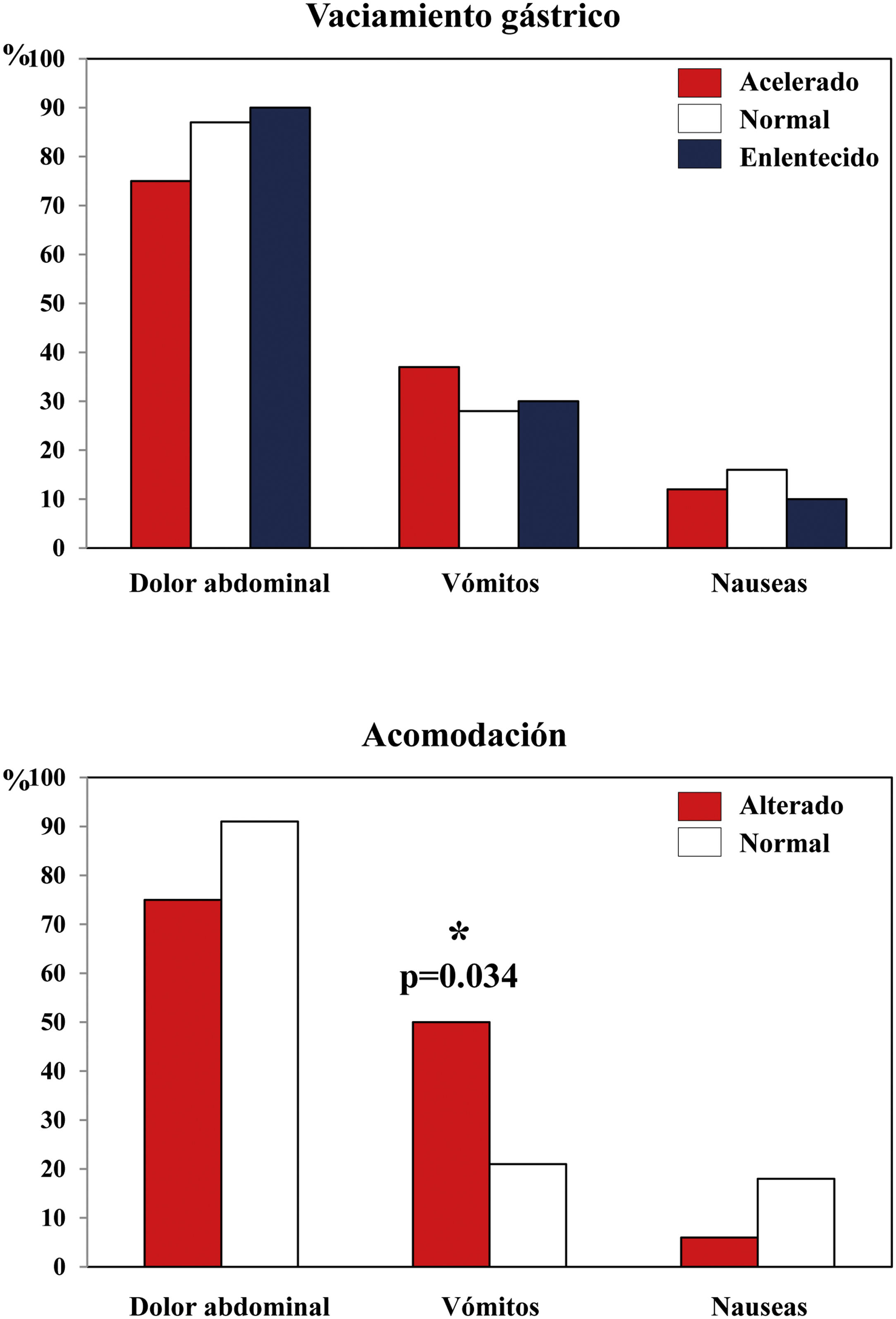
A greater prevalence of clinical symptoms was not observed in either of the two groups, except for vomiting, which was significantly more frequent in the case of altered accommodation (Fig. 2).
. Values shown as percentage. * Chi-square test.")
In regard to the comparison among patients with normal, delayed or rapid emptying, there were no significant differences in the IFD values (Kruskal-Wallis, p = 0.838) and neither was a greater prevalence of clinical symptoms observed in any of these groups (Fig. 2).
Lastly, there were no differences in the levels of IFD among the different definitive diagnoses (Kruskal-Wallis test, p = 0.926).
Correlations among parametersOn applying the Spearman correlation coefficient, a high positive correlation was observed between the IFD parameter and the qualitative evaluation of accommodation, with a correlation coefficient of 0.723 and p < 0.001.
DiscussionDigestive disorders are a frequent pathology in medical consultations. Gastric emptying scintigraphy is a non-invasive and quantitative physiological method and is currently considered the standard study for evaluation of these patients.5 However, it does not show the functionality of the proximal and distal stomach separately. This has led to considering other specific gastric functions, such as accommodation of the fundus or motility of the antrum.1
Gastric accommodation to food consists in the relaxation of the proximal portion of the stomach without an increase in intragastric pressure. This response to ingestion, mediated by the vagus nerve, is constituted by receptive relaxation and other adaptative functions with which the fundus is converted into a reservoir. Maximum accommodation is produced at around 15 min after ingestion.6 Alteration of this accommodation can cause rapid transit of the food to the antrum, which can produce its distension and the appearance of symptoms of dyspepsia. These symptoms include nausea, vomiting, sensation of early satiety, weight loss and abdominal pain.7 The development of new specific treatments for this alteration, such as muscarinic receptor antagonists, has increased interest in its study.8
There are different methods for studying accommodation, with the gastric barostat test is currently considered the most adequate. Nevertheless, this is an invasive and uncomfortable method for patients, that can alter the gastric physiology and is not always available or tolerated.3 Three-dimensional ultrasonography is an inexpensive, available and non-invasive method with results that adequately correlate with other procedures. This technique has limitations due to the presence of air in the proximal stomach and is operator-dependent.9 Magnetic resonance allows determining anatomy, motility and gastric emptying in the same study with greater spatial and temporal resolution. However, its cost, availability and the need for sedation in young patients limits its use.10 Lastly, the satiety test by the administration of caloric fluid is a simple and well tolerated method, although the results lack correlation with other procedures.11
In regard to radioisotope methods, Kuiken et al.12 were the first to develop the single photon emission computed tomography (SPECT) method for evaluation of accommodation. The study requires the injection of pertechnetate for its deposit in the gastric mucosa, and the study is generally done separately with respect to gastric emptying scintigraphy, makings its use difficult.13
Bredenoord et al.14 determined accommodation using SPECT in 214 patients with functional dyspepsia, diabetes mellitus, after fundoplication, and with rumination syndrome. These authors also evaluated accommodation in 173 of the patients by gastric emptying scintigraphy. They found no significant differences between groups in relation to the symptoms. Among the whole group, 43% presented altered accommodation and 35% showed rapid or delayed emptying. The group with diabetes more frequently presented alteration in accommodation than in emptying. Among the patients with normal emptying, 25% presented altered accommodation. In conclusion, the authors considered that evaluation of accommodation could help identify patients for selective and more effective treatment.
Publications on the distribution of food within the stomach by planar scintigraphy began to appear in the last third of the last century, for both the solid and the liquid phase of the food.15 More recently, Tomita et al.16 compared the determination of accommodation by gastric emptying scintigraphy and the gastric barostat test in 20 patients. They divided the stomach into three equal area, and found a significant correlation between the two methods and a high reproducibility in the scintigraphic study. For the authors, the radioisotope study was a useful test for the determination of accommodation.
Orthey et al.4 quantitatively determined IFD in the basal image of the scintigraphic study as an indirect method for evaluating accommodation. According to the authors, the method of dividing the stomach into two halves was more adequate than the division into three parts or than the separation at the base of the angular incisure of the lesser curvature, the localization of which was difficult to determine in the scintigraphic image. Nineteen percent of the patients with normal gastric emptying and 12% with delayed emptying presented altered accommodation. There was a significant correlation between the qualitative and quantitative determination of accommodation as well as a significant difference in the IFD values between the patients with normal and altered accommodation (values of 0.809 and 0.447, respectively).
Chedid et al.17 evaluated IFD in 108 patients with diabetes mellitus by planar scintigraphy and accommodation by SPECT and found a lack of correlation between the two parameters. As a limitation of the study, the authors stated that the SPECT method determines the global content of the stomach, including food, air and gastric secretions, while the planar study only considers the labeled food. They concluded that the IFD method required greater validation before being applied in clinical practice.
Our results are, in part, concordant with those described above in that we found a correlation between the IFD parameter and qualitative evaluation of accommodation as well as a significant difference in this parameter in patients with normal or altered accommodation. Likewise, the rate of patients with scintigraphy showing normal emptying and altered accommodation was similar or close to that reported in some of the above publications. However, the IFD cut-off value found by the ROC analysis in our study was 0.785, which is higher than the 0.568 described by Orthey et al. This difference could likely be explained by the use of a different method for delimiting the proximal and distal stomach and by the group of patients studied, who, in the latter study was made up of patients with symptoms of gastroparesis.
We found a lack of relation between most of the symptoms reported by the patients and the accommodation or the result of gastric emptying study. Only vomiting was more frequent in the case of altered accommodation. In this sense, Pasricha et al.18 developed a multicenter study in which they concluded that patients with normal emptying and symptoms of nauseas and vomiting showed a clinical presentation similar to those with delayed emptying. Other authors have reported a poor relationship between symptoms and alteration in accommodation and an association between delayed emptying and the presence of vomiting.14 There seems to be consensus on the need to carry out more studies on the relationship between the symptoms and motor dysfunction of the stomach.
In relation to the different diagnoses found, we discussed the findings found in the three most numerous groups. The prevalence of allergies, food intolerances and celiac disease is high in the general population, with a symptomatology that, on numerous occasions overlaps with that of gastroduodenal disorders. In these patients, motility disorders along the whole digestive tract have been described at not only the esophageal and gastric levels but also at an intestinal level.19 In our study, a very significant number of cases showed an alteration of accommodation (47%) and emptying (34%), generally being accelerated in the latter case.
Functional dyspepsia makes up part of the functional gastroduodenal disorders defined by the Rome IV criteria published in 2016. This disorder has a high prevalence, considering that 10% of the adult population in English-speaking countries fulfill the diagnostic criteria.20 It has been reported that 25% of the patients with functional dyspepsia present a gastric emptying scintigraphy study within normality, while 40% show an alteration in accommodation.4 In our case, 58% of the patients diagnosed with this disorder presented normal emptying and 25% had problems of accommodation.
Gastroparesis is a chronic disease characterized by a delay in emptying in the absence of mechanical obstruction. The most frequent symptoms are abdominal pain and nausea and vomiting. Fifty percent of these cases are considered of idiopathic origin and around 30% due to diabetic neuropathy.21 Diabetic patients have a high risk of developing problems of gastric motility due to possible neuropathy of the vagus nerve.6 In our study group, 4 patients presented Type 1 diabetes mellitus, with 3 being diagnosed with gastroparesis with delayed emptying and accommodation being within normality. In this group of patients, abdominal pain was a generalized symptom.
Our study has some limitations that should be considered. Since the time allowed for the patients to eat the food before the scintigraphic study was 10 min, some of these patients could not complete the meal. This could be a cause of insufficient accommodation response of the fundus and the presence of bias in the results. To simplify the scintigraphic study, the SPECT method was not used, which might have provided a tridimensional and more accurate assessment of the accommodation. Lastly, previous studies have used evaluation of the contractions of the antrum by acquisition of dynamic scintigraphic studies and Fourier analysis to determine distal motility. This is considered to allow a more physiological division of the stomach than that used in the present study.1
In conclusion, in addition to determining motility, the gastric emptying scintigraphic study allowed qualitative and quantitative evaluation of the distribution of the radiotracer in the stomach, and thus, indirectly assess accommodation in the fundus. It provided additional diagnostic information in a simple way without the need for changes in the acquisition protocol and relevant additional information for patient management.
Conflict of interestThe authors have no conflicts of interest to declare.
