



We present a 55-year-old male patient with a follicular lymphoma (stage III-S) diagnosed in 2014. CHOP chemotherapy and Rituximab ended in 2016 with a good response. In 2020 a soft palate mass appeared. This lesion was biopsied and a lymphoid B neoplasm with a nodular pattern was found. Staging [18F]FDG PET/CT found several hypermetabolic lymphatic nodes at cervical, pectoral and iliac regions, with a hard palate mass and other retroperitoneal lesion; so the conclusion was a lymphoma recurrence. The patient started new line treatment with ESHAP chemotherapy (Figs. 1 and 2).
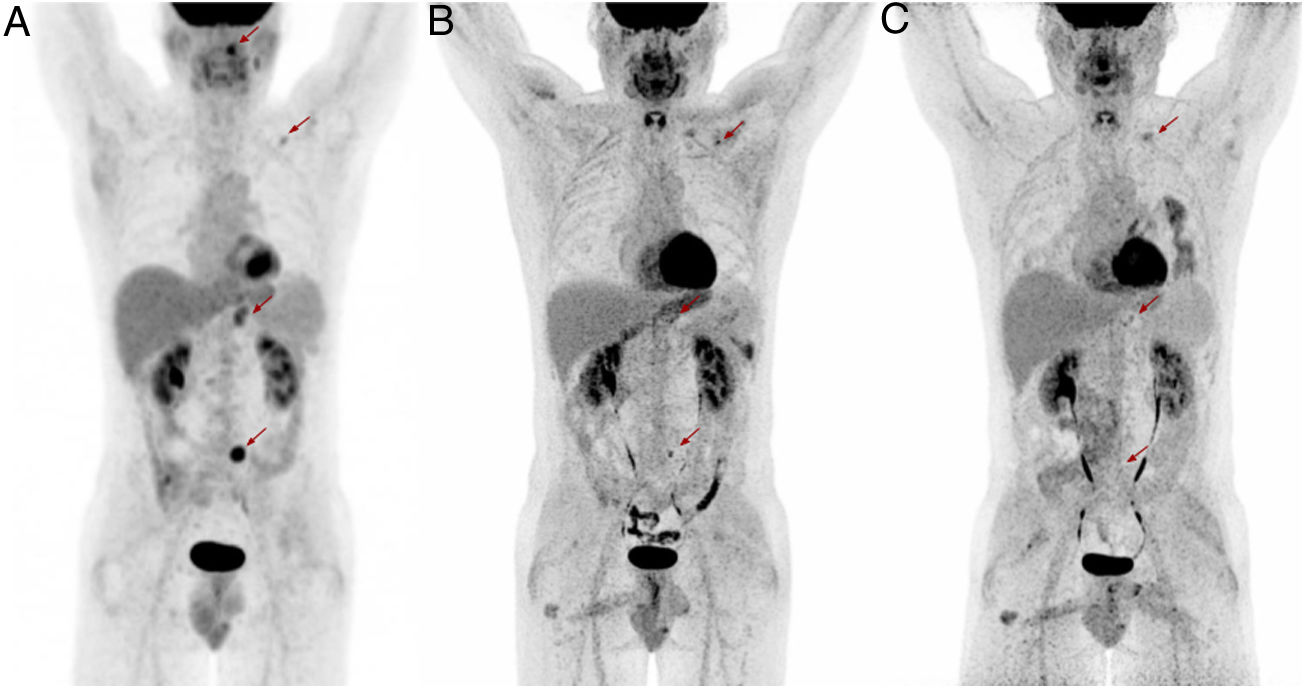
![MIP PET images. Evolution of lymphoma studied by [18F]FDG PET/CT. (A) Relapse [18F]FDG PET/CT: June 2020. (B) After chemotherapy [18F]FDG PET/CT: September 2020. (C) After SARS-COV-2 infection: December 2020. Arrows signal the pectoral lymph node (upper arrow), retropancreatic mass (middle arrow) and iliac lymph node (lower arrow) in each image.](https://static.elsevier.es/multimedia/22538089/0000004200000001/v1_202301120623/S2253808922000477/v1_202301120623/en/main.assets/gr1.jpeg?xkr=ue/ImdikoIMrsJoerZ+w997EogCnBdOOD93cPFbanNdV4B9vwZQjgKcZv3MP4CdsNwQlWjMJVGmnQkWYSILi5LeY9sQyce9iSqg1H5Z+1uLtuRLt22gt+UqqkopavpOlGAFYCi/mMmacznp5ahklGKyqhjr4xu17G9ffPnIoUXiXP6IM/b9gmzq4EQwCNxhJ2vb3/d3/eNgiw0N10WGhrzuVSWRev65rCo6nLuIjqD5UdBMaLF6t0tEeHMhCmHXCmqN7kcEY8rs+xBbjIpKu7KY9Tt+U1eJCUFU6NX5SzjSI+foYdWbxSW3K5R/qUvFJ "MIP PET images. Evolution of lymphoma studied by [18F]FDG PET/CT. (A) Relapse [18F]FDG PET/CT: June 2020. (B) After chemotherapy [18F]FDG PET/CT: September 2020. (C) After SARS-COV-2 infection: December 2020. Arrows signal the pectoral lymph node (upper arrow), retropancreatic mass (middle arrow) and iliac lymph node (lower arrow) in each image.")
MIP PET images. Evolution of lymphoma studied by [18F]FDG PET/CT. (A) Relapse [18F]FDG PET/CT: June 2020. (B) After chemotherapy [18F]FDG PET/CT: September 2020. (C) After SARS-COV-2 infection: December 2020. Arrows signal the pectoral lymph node (upper arrow), retropancreatic mass (middle arrow) and iliac lymph node (lower arrow) in each image.
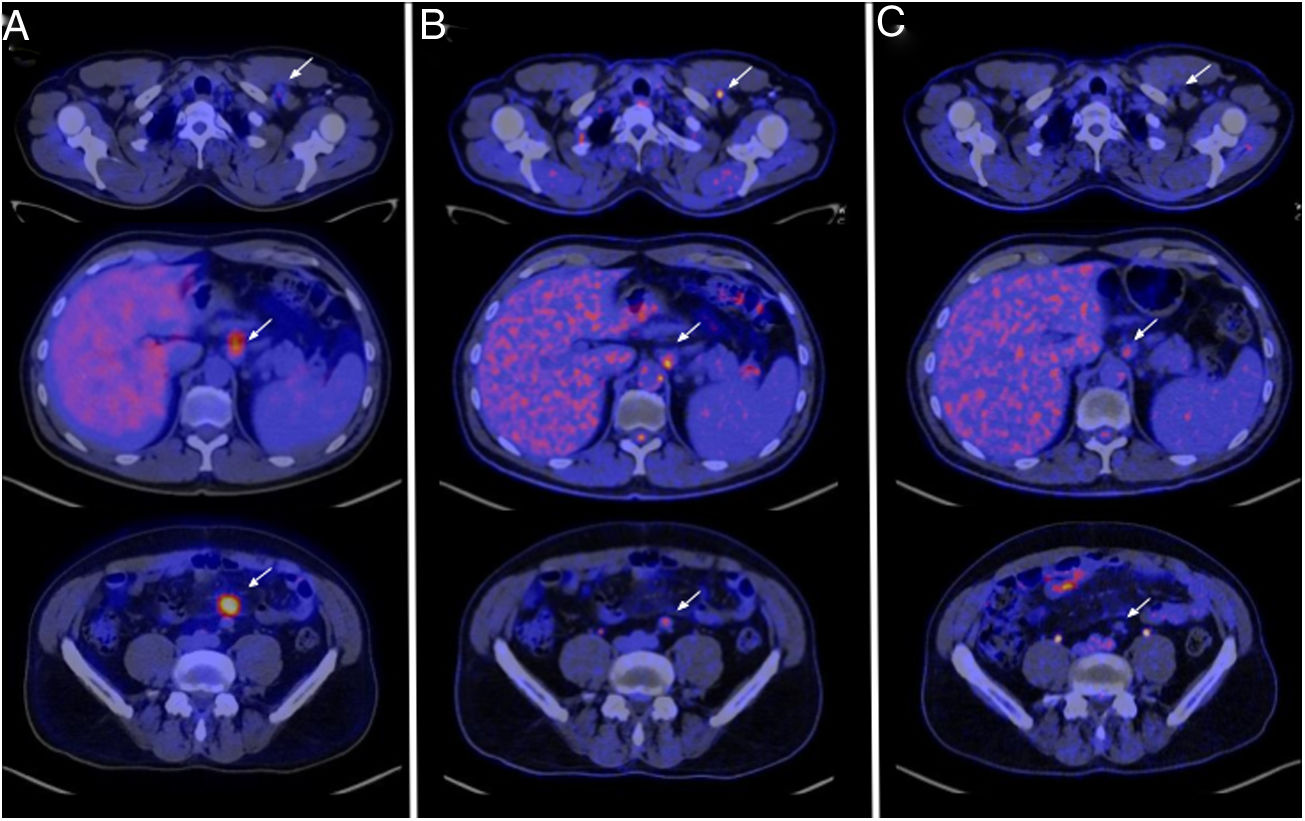
![Transaxial fusion PET/CT images. Evolution of lymphoma, [18F]FDG PET/CT axial cuts. The upper set of arrows points the left retropectoral lymph node (level T2, ), the middle set of arrows points the retropancreatic mass (level T11-T12, hepatic hilum) and the lower set of arrows points the left iliac lymph node (level L4-L5, aortic bifurcation). (A) Relapse [18F]FDG PET/CT: June 30th 2020. (B) After chemotherapy [18F]FDG PET/CT: September 10th 2020. (C) After SARS-COV-2 infection: December 16th 2020.](https://static.elsevier.es/multimedia/22538089/0000004200000001/v1_202301120623/S2253808922000477/v1_202301120623/en/main.assets/gr2.jpeg?xkr=ue/ImdikoIMrsJoerZ+w997EogCnBdOOD93cPFbanNdV4B9vwZQjgKcZv3MP4CdsNwQlWjMJVGmnQkWYSILi5LeY9sQyce9iSqg1H5Z+1uLtuRLt22gt+UqqkopavpOlGAFYCi/mMmacznp5ahklGKyqhjr4xu17G9ffPnIoUXiXP6IM/b9gmzq4EQwCNxhJ2vb3/d3/eNgiw0N10WGhrzuVSWRev65rCo6nLuIjqD5UdBMaLF6t0tEeHMhCmHXCmqN7kcEY8rs+xBbjIpKu7KY9Tt+U1eJCUFU6NX5SzjSI+foYdWbxSW3K5R/qUvFJ "Transaxial fusion PET/CT images. Evolution of lymphoma, [18F]FDG PET/CT axial cuts. The upper set of arrows points the left retropectoral lymph node (level T2, ), the middle set of arrows points the retropancreatic mass (level T11-T12, hepatic hilum) and the lower set of arrows points the left iliac lymph node (level L4-L5, aortic bifurcation). (A) Relapse [18F]FDG PET/CT: June 30th 2020. (B) After chemotherapy [18F]FDG PET/CT: September 10th 2020. (C) After SARS-COV-2 infection: December 16th 2020.")
Transaxial fusion PET/CT images. Evolution of lymphoma, [18F]FDG PET/CT axial cuts. The upper set of arrows points the left retropectoral lymph node (level T2, ), the middle set of arrows points the retropancreatic mass (level T11-T12, hepatic hilum) and the lower set of arrows points the left iliac lymph node (level L4-L5, aortic bifurcation). (A) Relapse [18F]FDG PET/CT: June 30th 2020. (B) After chemotherapy [18F]FDG PET/CT: September 10th 2020. (C) After SARS-COV-2 infection: December 16th 2020.
After 2 cycles of chemotherapy, an interim [18F]FDG PET/CT was performed. The cervical lymphadenopathy and the hard palate mass disappeared. The rest of the lymphadenopathies decreased their metabolic activity. Even the retropancreatic mass reduced its size. The remanings lesions presented the following SUVmax: retropancreatic mass (3,87), pectoral (4,94) and iliac (4,18). The liver SUVmean was 1,87 and the mediastinal blood pool SUVmean was 1,16. The Metabolic Tumor Volume (MTV) was 3,68 cm3 and the Total Lesion Glycolysis (TLG) was 7,85 SUV-lbm.cm3. The next proposed line of treatment was Rituximab. Before the first cycle, the patient suffered from SARS-COV-2 pneumonia and had a corticosteroid treatment, but no immunochemotherapy. One month after the infection, the patient got a negative result for SARS-COV-2 PCR.
Another restaging [18F]FDG PET/CT was performed and the pectoral and iliac lymphadenopathies significantly decreased their metabolic activity rate and size. Also, the retropancreatic mass reduced its size, but kept its metabolic activity rate. The SUVmax of the lesions was: retropancreatic mass (3,44), pectoral (1,93) and iliac (1,49). The liver SUVmean was 1,56 and the mediastinal blood pool SUVmean was 1,51. The MTV was 3,00 cm3 and the TLG was 4,23 SUV-lbm.cm3. Additionally, a pulmonary infiltrate with an increase of the metabolic activity was described related to the SARS-COV-2 infection. It was interpreted as a partial response without any therapy. Finally, the Rituximab treatment was initiated.
As mentioned in the medical literature, there is evidence that virus antigens could generate an antitumor activity1. There is a low number of reported cases of lymphomas which spontaneously decrease its metabolic activity and size, concurring with a viral infection2. The main hypothesis in this case was that the SARS-COV-2 virus triggered an immune response that brought out a cytokines chain which activated an immune cells reaction against the neoplastic cells3.
Please cite this article as: Rudolphi-Solero T, Rashki M, Fernández-Fernández J, Rivas-Navas D, Ramos-Font C, Rodríguez-Fernández A. El virus SARS-COV-2 desencadena una respuesta inmunitaria antitumoral en un paciente con linfoma. Rev Esp Med Nucl Imagen Mol. 2023;42:59–60.
