




Auriculotherapy and auricular acupuncture are techniques that involve stimulating specific points on the ear to treat a variety of physical and psychological conditions. This technique is based on the principle that the ear is a microsystem of the body, with each point corresponding to a specific organ or system. The history of conditions being treated through the auricle can be traced back to ancient civilizations, with evidence of its use found in Chinese, Egyptian, Greek, and Roman cultures. However, it was not until the 20th century that modern auriculotherapy was developed. Since then, auriculotherapy has been the subject of extensive research, and there is now a growing body of evidence to support its effectiveness. In this article, we discuss the historical context, possible mechanisms, clinical implications for treatment and diagnosis, and conclude by presenting a simple observation case.
The use of the auricle reflex system for treatment and diagnosis seems to be a promising complementary method with potential value for healthcare providers. It may provide a wider understanding of a patient's health and guide the selection of appropriate treatment options. It may also provide a cost-effective preventive diagnosis assessment tool that can be employed in areas without access to top-of-the-line healthcare technologies. More research is needed to fully understand the mechanisms of action of the auricle microsystem and to further validate its effectiveness.
La auriculoterapia y la acupuntura auricular son técnicas que consisten en estimular puntos específicos de la oreja para tratar diversas afecciones físicas y psicológicas. Esta técnica se basa en el principio de que la oreja es un microsistema del cuerpo, en el que cada punto corresponde a un órgano o sistema específico. La historia del tratamiento de afecciones a través del pabellón auricular se remonta a las civilizaciones antiguas, con testimonios de su uso en las culturas china, egipcia, griega y romana. Sin embargo, la auriculoterapia moderna no se desarrolló hasta el siglo XX. Desde entonces, la auriculoterapia ha sido objeto de numerosas investigaciones y cada vez hay más pruebas de su eficacia. En este artículo analizamos el contexto histórico, los posibles mecanismos, las implicaciones clínicas para el tratamiento y el diagnóstico, y concluimos presentando un sencillo caso de observación.
El uso del sistema reflejo del pabellón auricular para el tratamiento y el diagnóstico parece ser un método complementario prometedor con un valor potencial para los profesionales sanitarios. Puede proporcionar una comprensión más amplia de la salud de un paciente y orientar la selección de las opciones de tratamiento adecuadas. También puede constituir una herramienta rentable de evaluación diagnóstica preventiva que puede emplearse en zonas sin acceso a tecnologías sanitarias de vanguardia. Es necesario seguir investigando para comprender plenamente los mecanismos de acción del microsistema auricular y seguir validando su eficacia.
The auricle microsystem is usually associated with auriculotherapy and auriculoacupuncture as a diagnosis and treatment system. Besides the Chinese, in the ancient world, the use of the auricle in disease treatment has seen application by several other civilizations such as the Egyptians, Greeks, and Romans.5 However, it was only in 1634 AD that the topic resurfaced in Europe by the hand of the Portuguese doctor Manuel Álvares de Távora (Zacutus Lusitanus) who reported the use of the ear to treat sciatic pain in his “Praxis medica admiranda”6 (pp. 356–357). It was recently, around 1956, that modern auriculotherapy saw its birth as doctor Paul Nogier introduced his observations about the somatotopic correspondences of the ear.7
Later in the 80s, these auricle microsystem theories were subjected to an important scientific trial to establish its validity. In the study by Oleson et al.,8 physicians blinded to patients' conditions examined the patient's ear for areas of elevated skin conductivity or tenderness. 75.2% of the auricle diagnoses were confirmed by established medical diagnosis, supporting the hypothesis of somatic organization of the human body in the auricle.
The use of auriculotherapy and auriculoacupuncture still relies on different notions according to diverse theoretical basis. However, efforts have been carried out in the last decades to develop common tools for education and research, as is the example of the “Universal Auriculotherapy Nomenclature”,9 doctor Romoli's auricular sectogram,10 as well as Széchenyi Orientation ear map.11
Main theoriesAccording to Neves et al.,12 effective stimulation at appropriate doses on both central and peripheral regions of the auricular pavilion has demonstrated the potential to induce behavioral inhibition effects, mitigate inflammatory responses, suppress appetite, and enhance various physiological functions, including cardiac performance. Additionally, positive outcomes have been observed in addressing conditions such as depressive symptoms, epilepsy, and pain.
To bolster the scientific foundation for the clinical application of auricular acupuncture, it is crucial to delve into the mechanisms of its functioning and assess its clinical efficacy through rigorous investigation, including basic experimental research and preliminary pre-clinical experiments. This comprehensive understanding can significantly contribute to refining and optimizing therapeutic approaches.
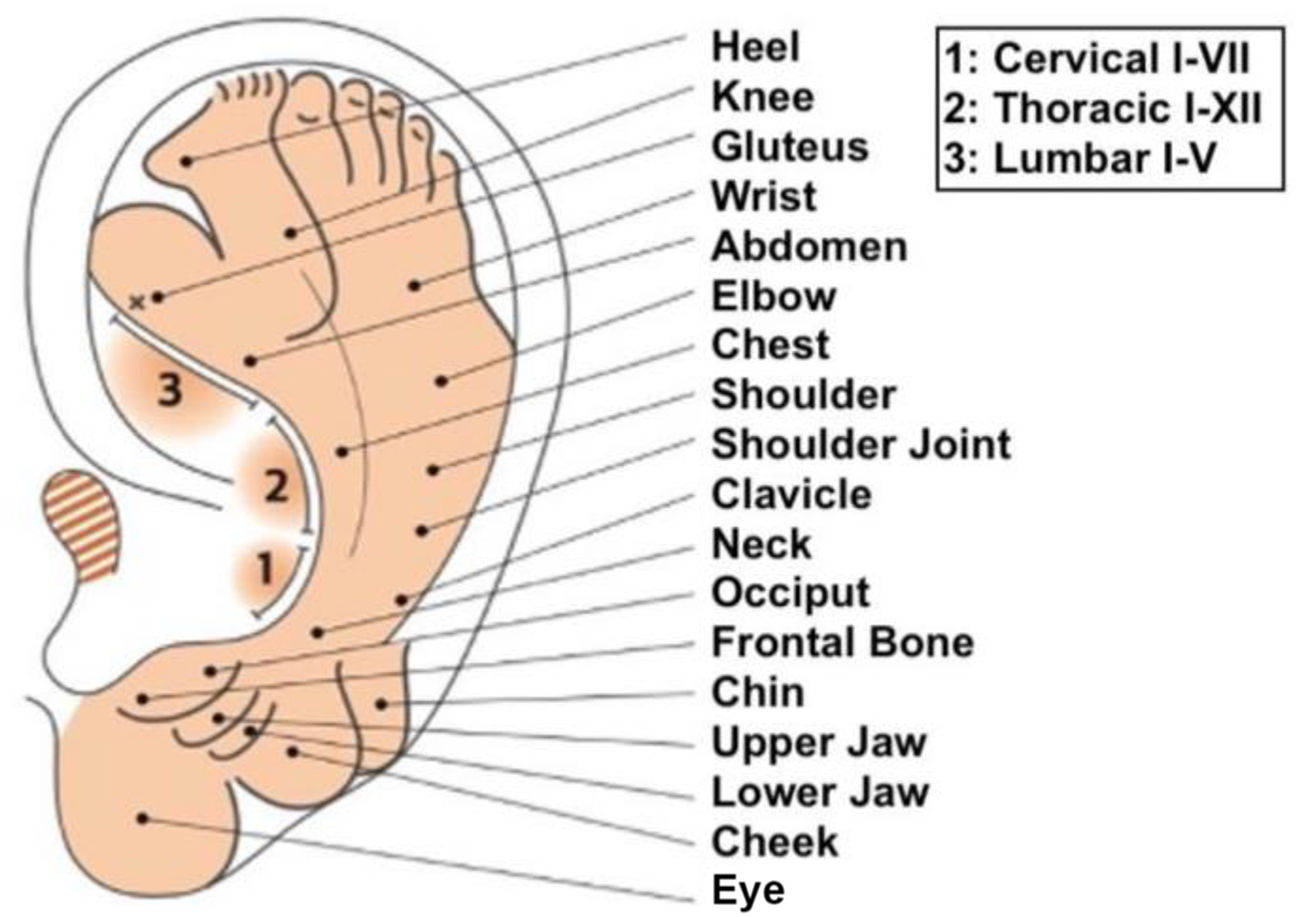
Somatotopic arrangement and embryological regionsNogier's groundbreaking work introduced the concept of a somatotopic arrangement, often referred to as the Homuncular Theory, by mapping an inverted fetus onto the ear (Fig. 1), highlighting its resemblance.5,13,14 Widely adopted for diagnosing and treating auricular diseases, this map serves as a key reference point in the field.15 According to this arrangement, the earlobe corresponds to the head and brain, the antihelix reflects the spine, the scaphoid fossa relates to the upper extremities, while the superior and inferior crus targets the lower extremities. The concha is associated with internal organs.

The historical map of Nogier, by Bachman. Image retrieved from Lovato et al.2
Nogier attributed the relationship between auricular acupuncture and various body areas to the vagus nerve and the autonomic nervous system.5,13,14 As mentioned before, Oleson et al.8 demonstrated a 75.2% accuracy in diagnosing medical conditions using the somatotopic arrangement of the auricle.8
In another study by Romoli et al.,16 it involved 3 diagnostic methods: auricle inspection, pain pressure test, and electrical skin resistance test. When all 3 diagnostic methods were combined, a notable 78.6% success rate was achieved in identifying symptoms and syndromes related to both somatic and mental disorders.
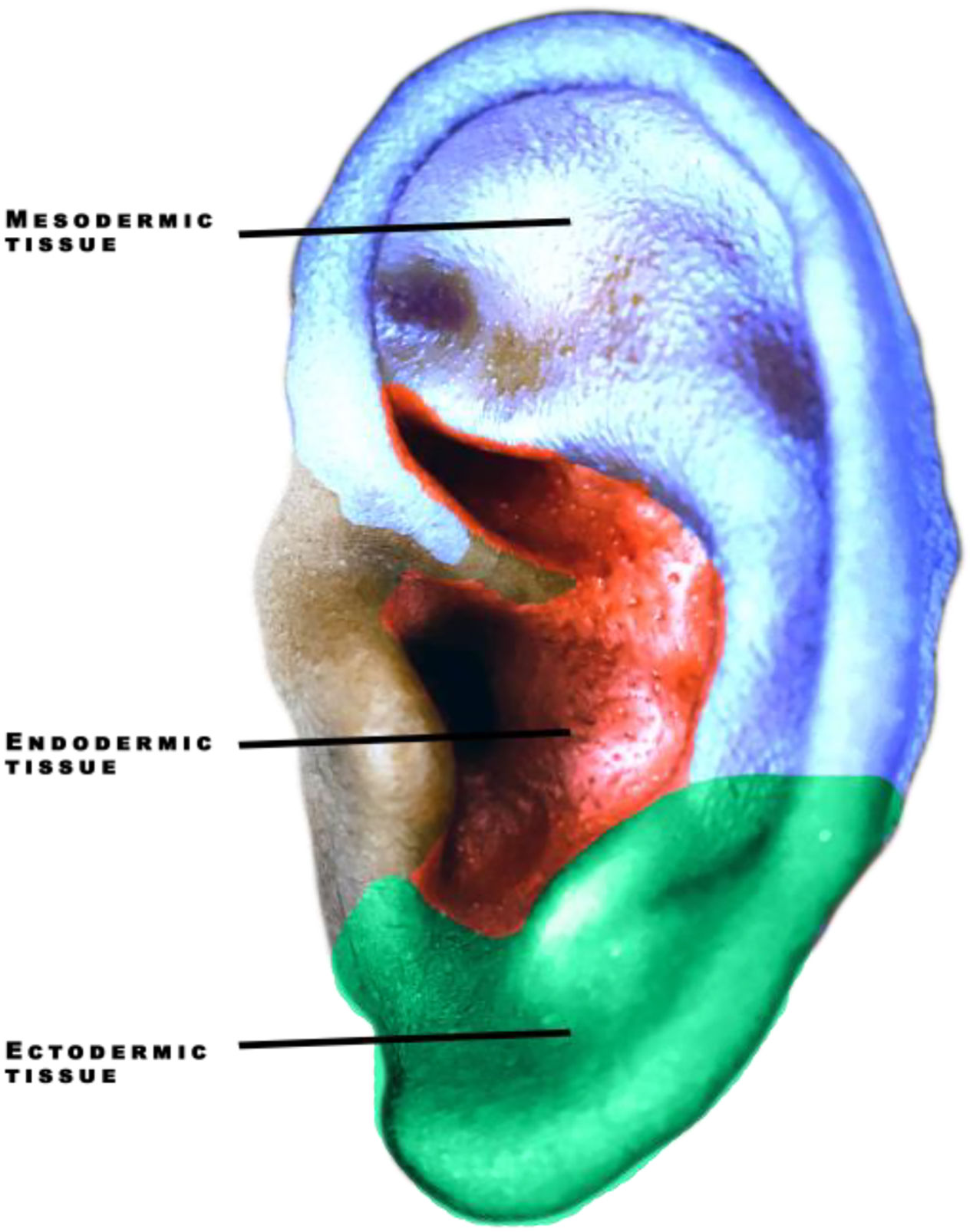
Regarding the concept of embryological regions in auriculotherapy, it aligns closely with somatotopic organization. In this framework, the earlobe and tragus are associated with the ectoderm, while the concha corresponds to the endoderm. The remaining part of the ear is linked to the mesoderm (Fig. 2). This arrangement provides a unique perspective where specific organs associated with the endoderm, for example, can be targeted for treatment or diagnosis through the concha.17

A key principle in this embryological organization is the lower portion of the ear representing the head and brain, while the upper portion corresponds to the extremities of the members.
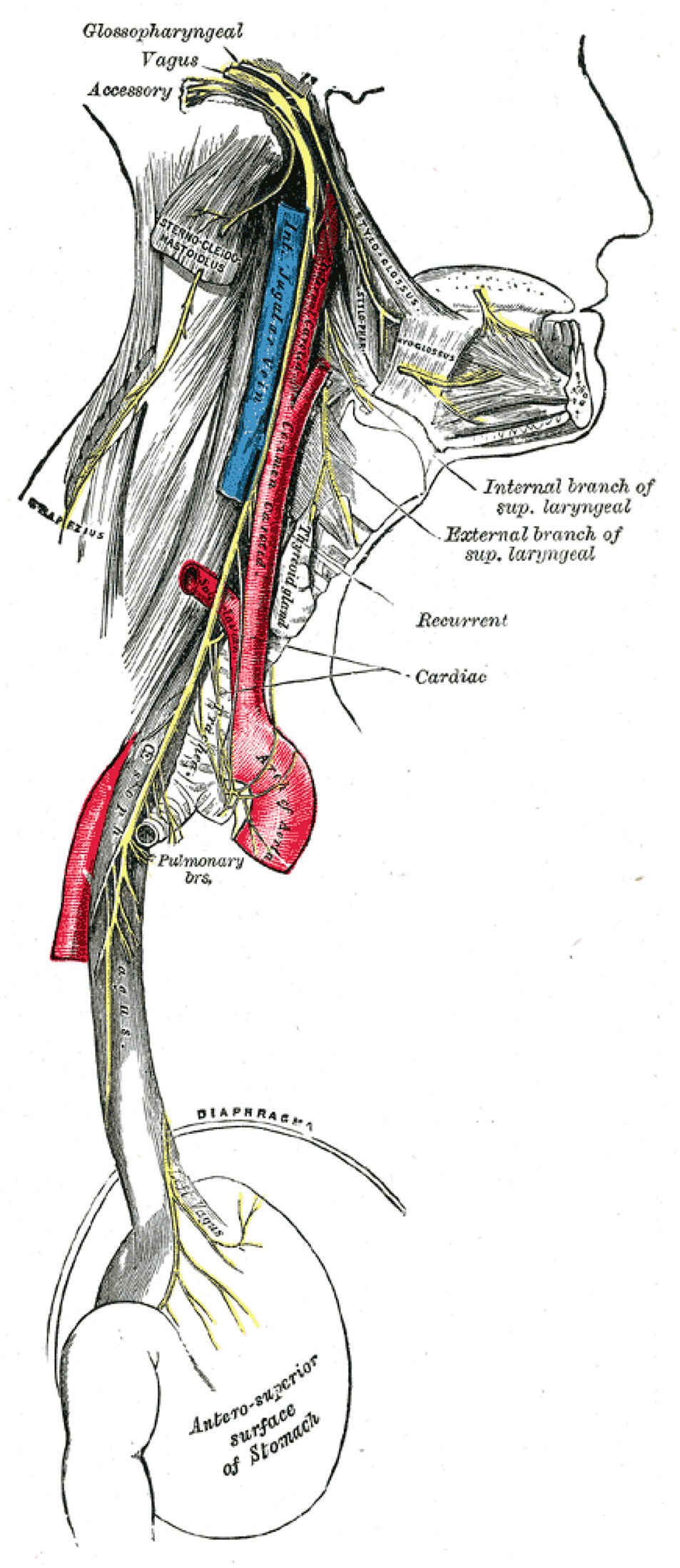
Channel/meridian theoryIn accordance with the channel (or meridian) theory, the auricle establishes direct and indirect connections with the 12 channels of traditional Chinese medicine. In fact, the Huang Di Nei Jing asserts that every channel converges in this area.18,19 The 6 Yang channels run directly into the ear or around the side of the ear (Fig. 3). The 6 Yin channels connect with the ear directly or indirectly through other divergent channels and connect with the Yang channels.18 (See Figs. 4–6.)

Anatomy depicting the trajectory of the vagus nerve along the neck and thorax. Figure by Gray et al.3

Inervation of the auricle. Figure by Jiang et al.4
Although some authors state that the origin of the Chinese auricle system lacks a proper theoretical framework,15 others understand the Chinese auricle microsystem as a direct representation of the reflex system of the acupuncture points and channels.20
Reflex mechanismFunctional magnetic imaging studies have been crucial to understand how the auriculotherapy reflex may happen in the human body.
It is the case of the study of Romoli et al.,21 which tested brain activation of 2 auricle points. The stimulation of the thumb auricular acupoint on the left ear produced a bilateral activation in the parietal operculum. As for the stimulation of the brain stem auricular acupoint of the left ear, it resulted in a pattern of regions belonging to the pain matrix, but with local differences in the left amygdala, anterior cingulate cortex, and cerebellum. The authors also highlight the fact that these results are in agreement with the therapeutic indications of this point, which include head pain, dizziness, and vertigo.
These differences in activation patterns between the 2 points suggest the specificity of the 2 acupoints.
In another study,22 the stimulation of the hand auricular acupoint results in specific activation in the somatosensory cortex for the hand of the post-central gyrus. Later, the same authors tested the knee auricular acupoint according to the Chinese and the French–German topographies. The authors concluded that the activation of the brain areas is different with potentially significant neurophysiological and clinical effects also differing. Nevertheless, both approaches may offer therapeutic benefits.
In the case of the study of Zhang et al.23 with stroke patients, auricular acupuncture activated the primary motor cortex (M1) of the brain, which may be a key mechanism of its positive results. Specifically, the results showed that the patients in the auricular acupuncture group had significantly greater increases in motor-evoked potential amplitude and oxyhemoglobin (HbO2) levels in the primary motor cortex M1 region of the brain than the patients in the control group.
However, much earlier in 1832, Friedrich Arnold had already found that stimulating the external ear canal could induce a cough similar to the cough reflex induced by the vagal nerve. Since the stimulation of the auricular branches of the vagus nerve may induce a similar response to that of the vagal nerve, the auricular reflex system may be in part based on this relationship between the auricular branches of the vagus nerve and the autonomic nervous system.13,24 (Fig. 3).
In fact, the auricular branches of the vagus nerve deliver fibers into the nucleus tractus solitaries.15,25 This nucleus serves as a critical relay center in the brainstem, receiving sensory input from the facial nerve (CN VII), glossopharyngeal nerve (CN IX), vagus nerve (CN X), and afferent nerves in the internal organs. This input provides the nucleus tractus solitarius with essential information about the status of the body's internal environment. In turn, the nucleus tractus solitarius sends outputs to various brain regions, including the reticular formation, parasympathetic preganglionic neurons, the paraventricular nucleus of the hypothalamus, the thalamus, and the amygdala. These outputs orchestrate a wide range of visceral reflexes, such as the carotid sinus reflex, the aortic reflex, the gag reflex, and the cough reflex, as well as several respiratory and gastrointestinal reflexes that regulate organ function.26 Therefore, the auricular branch of the vagus nerve plays a unique role in this intricate system. It innervates the concha of the auricle and the external auditory canal, particularly the inner part of the tragus. Stimulation of the auricular branch of the vagus nerve is initiated in the cutaneous concha, travels through the auricular nerve (CN IIX), and terminates in the nucleus tractus solitaries.27 These connections establish a pathway for the auricular branch of the vagus nerve to modulate autonomic nervous system activity.
In summary, the nucleus tractus solitarius serves as a pivotal hub for integrating visceral sensory input and orchestrating autonomic responses. The auricular branch of the vagus nerve, with its connections to the nucleus tractus solitarius, provides a direct access point for regulating the autonomic nervous system through stimulation of the auricle.
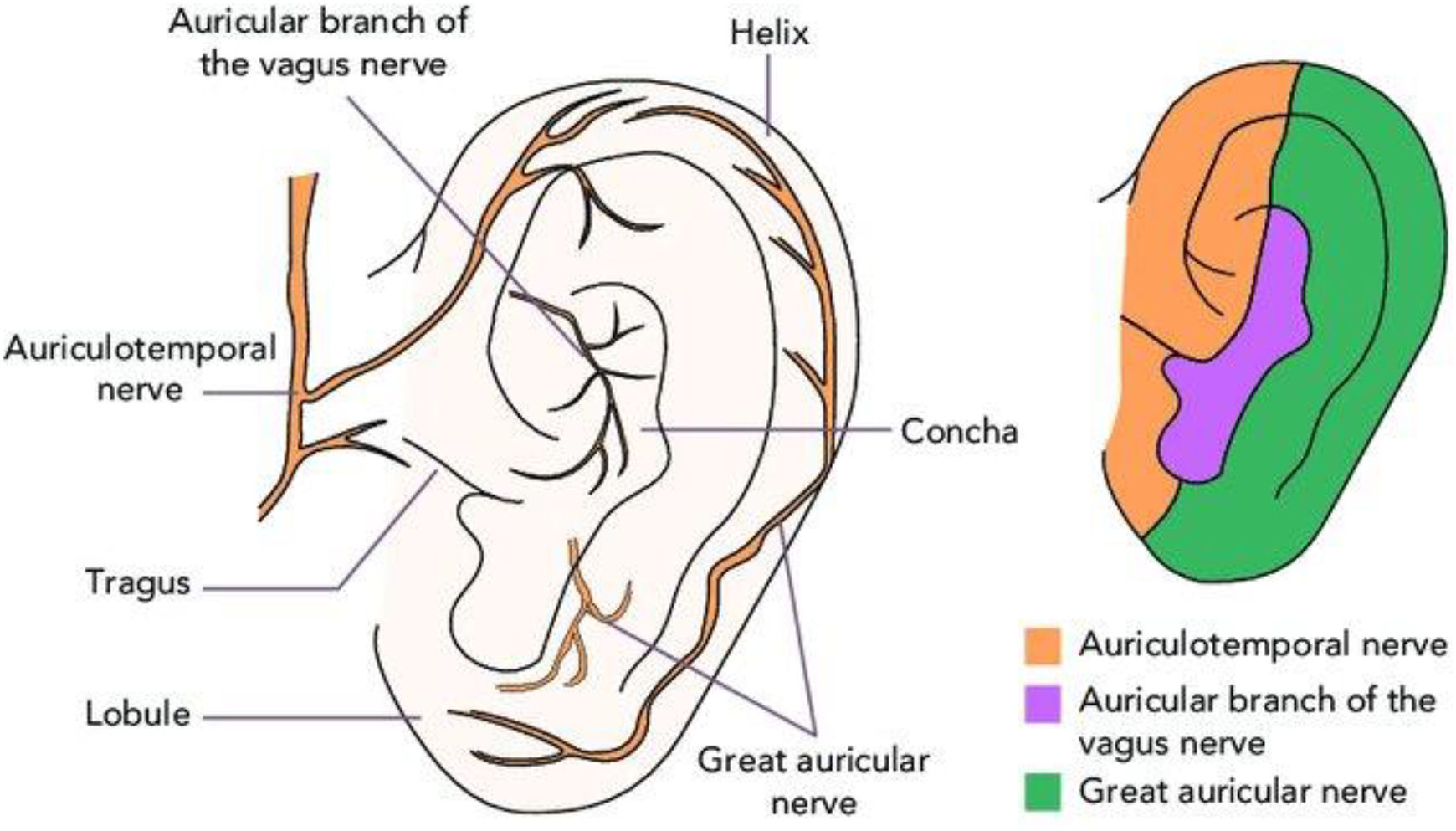
However, it is important to note that the auricle is also innervated by several other branches that may have a role in the reflex system. (Fig. 4).
The auriculotemporal nerve (CN V3), for example, is a branch of the mandibular division of the trigeminal nerve (CN V), it carries sensory, vasomotor, and parasympathetic fibers.28 The great auricular nerve (CN II) is a superficial branch of the cervical plexus, originating from fibers of the C2 and C3 spinal nerves.29 The cervical plexus supplies motor innervation to certain neck muscles and the diaphragm, and it provides sensory innervation to various regions of the head, neck, and chest.30 Since the intricacies of the nervous system are complex, future studies should focus on exploring possible mechanisms involving these nerves in the auricular reflex therapy theories.
Finally, the Delta reflex theory also stresses the relationship between parts of the body and auricle regions. This theory was orchestrated in the 1970s upon the observation that stimulating an area of the body with cold or heat resulted in changes in the temperature of the corresponding auricle areas.31
Clinical practice implicationsThe intricate interaction between the auricular branch of the vagus nerve and the nucleus tractus solitaries as a pathway to modulate autonomic nervous system activity may have implications for clinical practice.
In pain management, the stimulation of the auricle can potentially modulate pain signals and reduce pain perception, as some studies already suggest.32,33 This could be particularly beneficial for chronic pain conditions where traditional pain management strategies often fall short.
For gastrointestinal disorders, the modulation of the autonomic nervous system through the auricular branch of the vagus nerve stimulation could be employed to address various gastrointestinal disorders, such as irritable bowel syndrome and irritable bowel syndrome,34 constipation,35 and nausea.36,37 This stimulation may assist in restoring the homeostasis in the microbiota–gut–brain axis.38
As well, in cardiovascular conditions, the auricular branch of the vagus nerve stimulation could potentially regulate heart rate,39,40 blood pressure,41 and vascular tone,42 potentially offering new therapeutic approaches for cardiovascular diseases such as hypertension, arrhythmias, and heart failure.
In the case of neurological disorders, the auricular branch of the vagus nerve stimulation could be explored for the treatment of neurological disorders such as Parkinson's disease,43 epilepsy,44 and migraines.45
Amongst other potential benefits that could be discussed, stress management can also be mentioned. The auricular branch of the vagus nerve stimulation could potentially modulate the autonomic nervous system's “fight-or-flight” response, helping individuals manage stress and anxiety. This could be beneficial for conditions like anxiety disorders and post-traumatic stress disorder.46
These results are supported by several studies specifically using auriculotherapy and auriculoacupuncture.
For example, Aroca et al.47 found that auricular acupuncture applied at the “temporal mandibular joint” ear point was able to bring about significant improvements in patients with temporomandibular disorders, with outcomes similar to those in patients treated with an occlusal splint. The study found that auricular acupuncture was associated with improvements in both physical and emotional aspects of temporomandibular disorders. The study also found that the number of variables exhibiting significantly improved outcomes after treatment was similar between the auricular acupuncture and occlusal splint groups, whereas the sham group showed statistically significant differences when compared with these 2 groups. Similarly, the study of Cândido Dos Reis et al.,48 auricular acupuncture was effective in reducing sleep disorder symptoms and relieving symptoms of anxiety and temporomandibular disorder pain.
However, many other examples stress the practicality and positive effect of the use of auricular acupuncture and auriculotherapy for a myriad of situations such as migraine attacks,49 balance,50 depression,51 chemotherapy side effects,52 fibromyalgia,53 cerebral stroke,23 amongst others.
Implications for clinical diagnosisAs we have seen on the previous topic, many studies confirm that the stimulation of the bodily functions through the auricle is possible. The therapeutic potential of auriculotherapy and auricular acupuncture is therefore plausible and increasingly suggested.
However, as a reflex system, these therapies target the auricle not only for treatment but also as a diagnostic method.
Previously, we have discussed 2 crucial experiments that sustained the diagnostic framework. Firstly, the experiment of Oleson et al.8 showed that the auricle diagnosis does have a significant relation with the patients' conditions. Secondly, the Delta reflex theory is based on the observed reflex response of the auricle areas to stimulation of other body areas.31
However, other studies also contribute to this notion of diagnosis through the auricle. For example, the study of Kwai-Ping Suen et al.19 with 100 participants found out that patients with coronary heart disease were more likely to have a specific earlobe crease, higher electrical conductivity in the “heart” zone of the ear, and more tenderness in the “heart” region than patients without coronary heart disease.
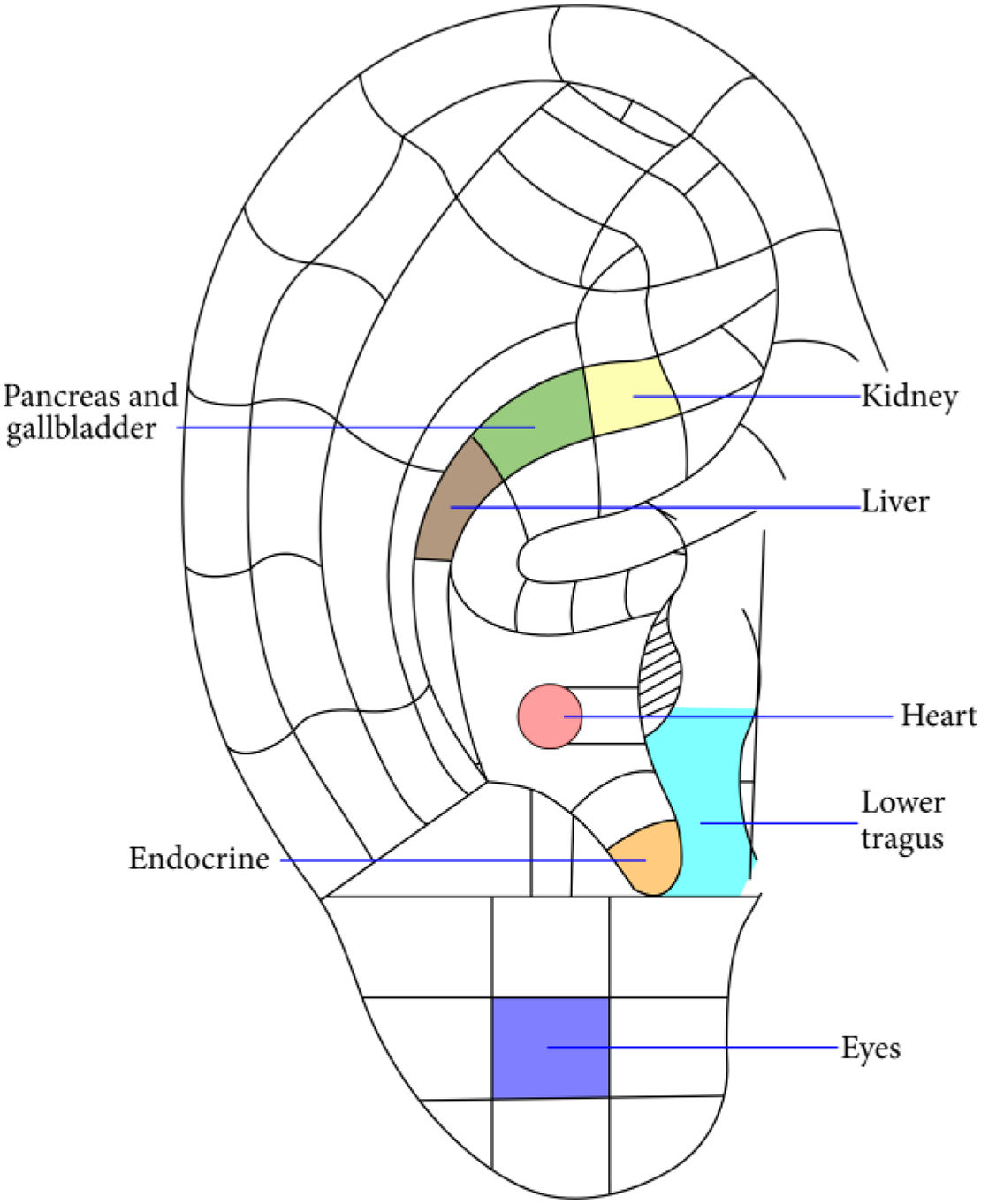
Another example is the study of Suen et al.54 with 282 participants, which found that tenderness in the “pancreas and gallbladder” and “Endocrine” auricular points and higher electrical conductivity of auricular points “Kidney” and “lower tragus” (also known as “xiao ke” in Chinese medicine, meaning “diabetes point”) were associated with diabetes mellitus status. These findings suggest that auricular diagnosis could be used to identify individuals at risk of developing diabetes mellitus or those with early-stage diabetes mellitus.
As well, another study by Suen et al.55 found that auricular signals, such as electrical conductivity and tenderness of specific points, including the “heart”, “pancreas and gall bladder”, and “endocrine”, were associated with an increased risk of metabolic syndrome. Metabolic syndrome patients had a higher prevalence of oily auricle complexion and a higher electrical conductivity on the “endocrine” (right) acupoint than controls. Additionally, both the “heart” and “endocrine” acupoints were found to be sensitive to tenderness, with a sensitivity of 60.8% and 59.8%, respectively. These study's findings suggest that auricular “symptoms” could be a useful tool for early screening for metabolic syndrome risk. (See Fig. 5).

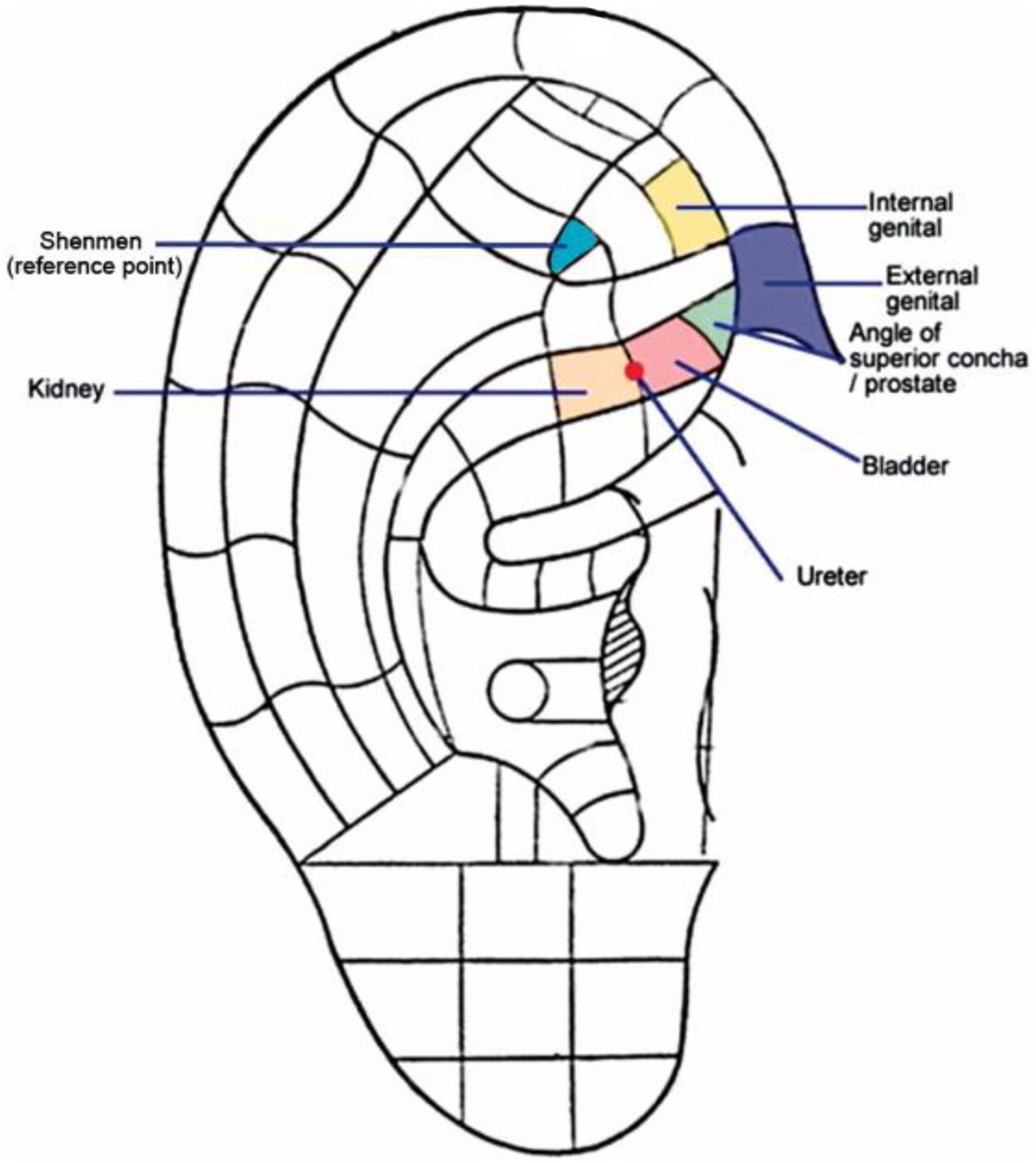
The same research team also found in another study1 that auricular diagnosis can be used to identify individuals with lower urinary tract symptoms with a high level of accuracy. The study found that auricular points such as the “angle of superior concha”, the “urinary bladder”, the “ureter”, the “kidney”, the “urethra”, and the “internal genitals” (See Fig. 6), were more tender and had lower electrical conductivity in individuals with lower urinary tract symptoms. This suggests that auricular diagnosis could be a useful tool for screening individuals for lower urinary tract symptoms and for monitoring the progression of the condition.

Furthermore, the study of Cheing et al.56 found that auricular examination could be used to screen for liver dysfunction. In their study, the authors found that patients with liver dysfunction had significantly more abnormalities in the appearance of the “liver” auricular acupuncture zone on both ears than patients without liver dysfunction. The study also found that patients with liver dysfunction had significantly lower electrical skin resistance on the “liver” zone on both ears than patients without liver dysfunction. The visual inspection was able to correctly identify 70% of patients with liver dysfunction. As well, visual inspection was able to correctly identify 76% of patients without liver dysfunction in the right ear and 60% of patients without liver dysfunction in the left ear. The mean difference in electrical skin resistance between patients with liver dysfunction and patients without liver dysfunction was 4.3 MΩ for the left ear and 4.5 MΩ for the right ear.
Clinical diagnosis exampleIn this article, a practical case is presented. The case is a simple clinical experience that was observed by the authors, and relates to the hypothesis of the auricle as a reflex system.
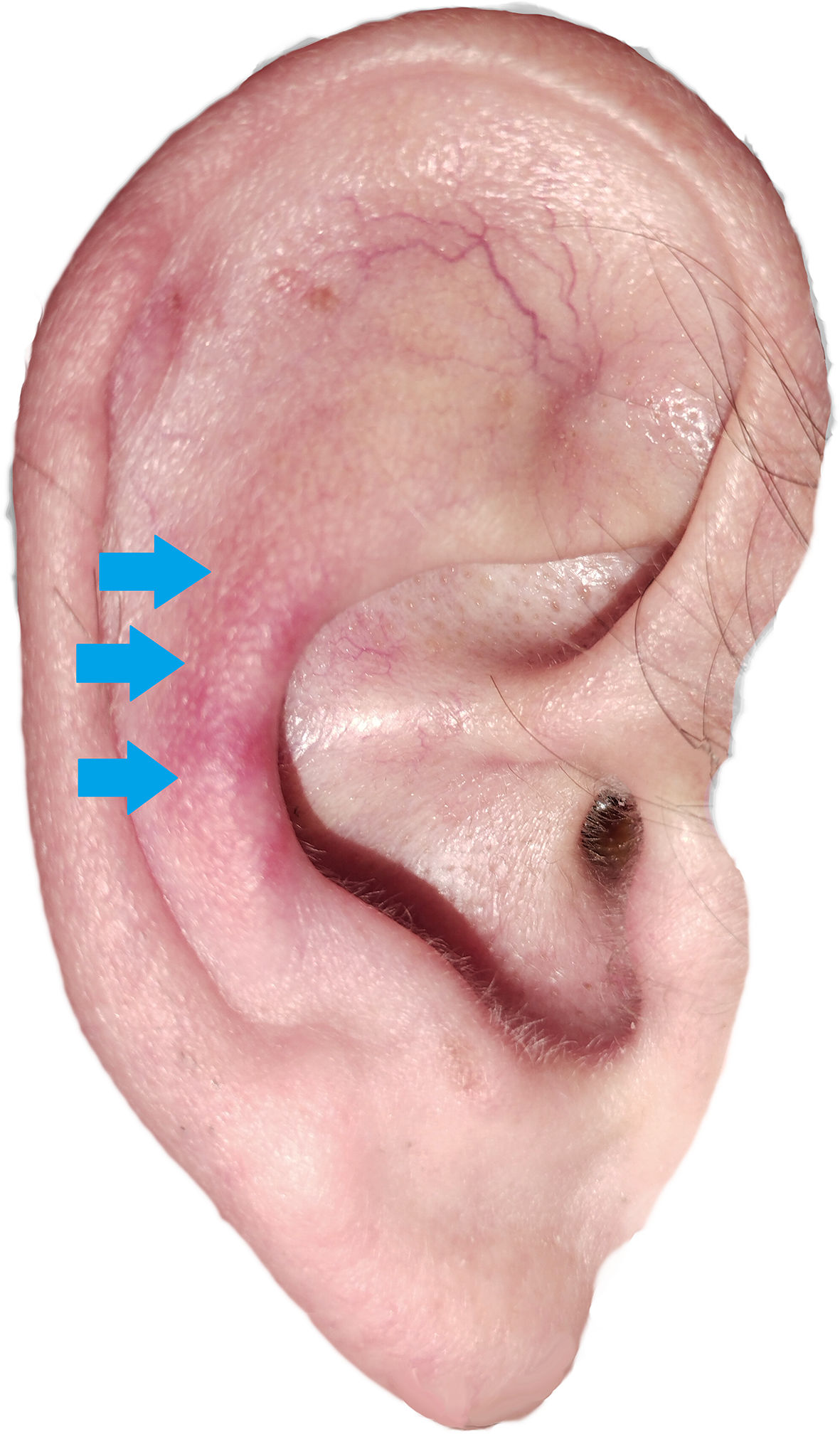
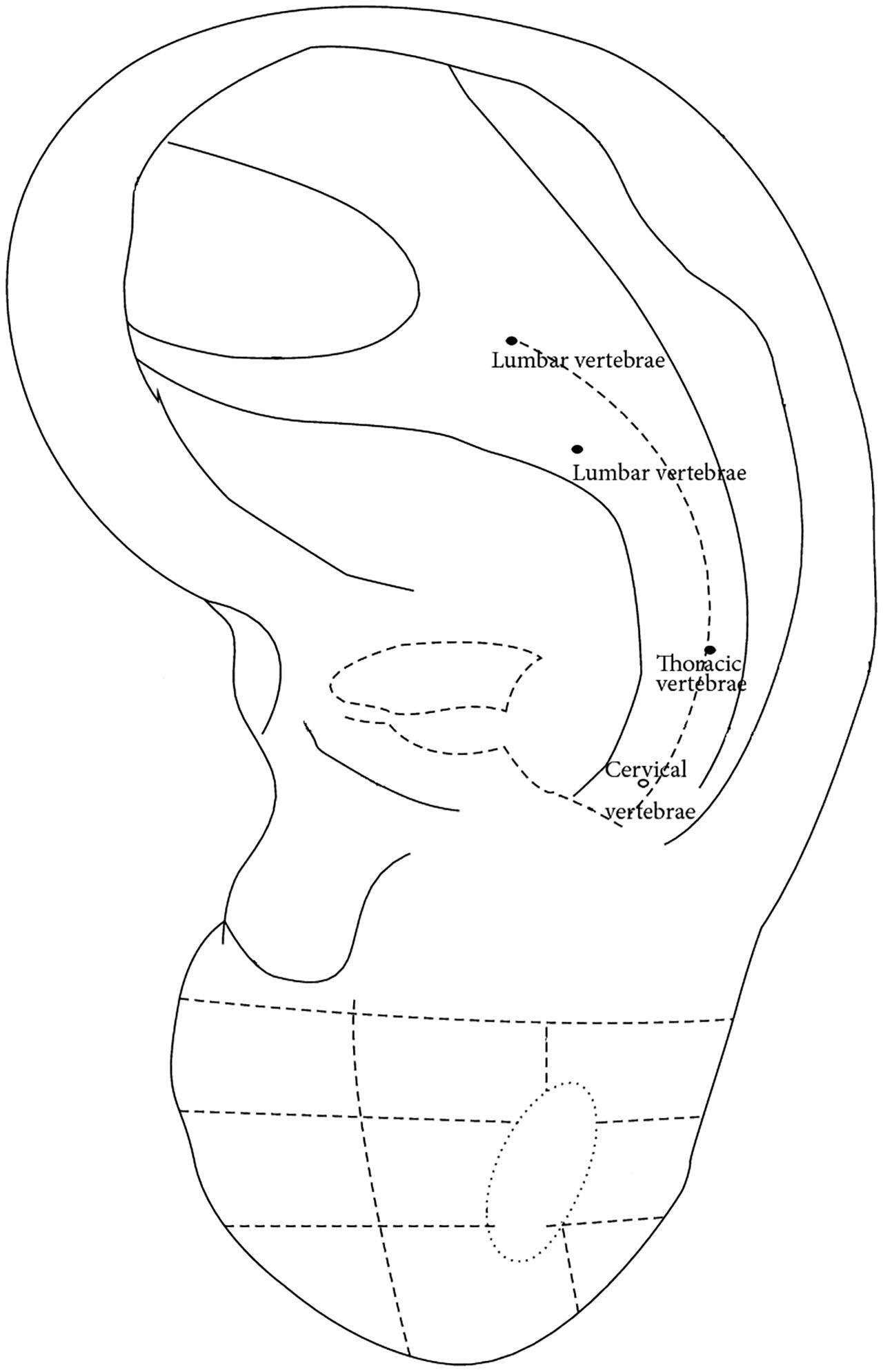
The patient, male, 34 years old, presented acute pain in the lower and mid back, slightly more predominant in the right side along the T11/12 and L1/L2. During the initial diagnosis stage, while contextualizing, the patient stated waking up with this pain, which led to the therapist inquiring about the previous night. The patient did not report anything in particular but hesitantly mentioned feeling a very sensitive and “burning-like” sensation in the right ear when laying his head on the pillow. It was requested the patient to precisely locate the discomfort and, upon inspection, it was noted a red predominant zone as shown in Fig. 7.
By analyzing the Chinese auricular acupuncture map57 (Fig. 8), it is observable that the area indicated by the patient is correspondent to the thoracic and lumbar vertebrae. As well, according to the international standardization,58 the signs are presented above the AH9 (Yaodfzhui) and AH11 (Xiongzhui) areas corresponding to the lumbosacral vertebrae and thoracic vertebrae, respectively.


Despite being an anecdotal evidence case, this example observed by the authors supports the suggestions provided by previous authors regarding the auricle reflex system's diagnostic potential.
Auriculotherapy's diagnostic capabilities are not intended to replace conventional medical diagnostics, such as laboratory tests or imaging studies. However, it can serve as a complementary tool to provide a more comprehensive understanding of a patient's health and guide the selection of appropriate treatment options. It may also provide a cost-effective preventive diagnosis assessment tool that can be employed in areas without access to top-of-the-line healthcare technologies, as observed in less developed countries.
ConclusionThe auricular microsystem is a system of reflex points on the ear that correspond to various parts of the body. Auriculotherapy and auricular acupuncture are techniques that involve stimulating these reflex points to treat a variety of conditions. However, this reflex system may also be important for diagnosis, complementing conventional diagnosis methods and improving healthcare accessibility.
There is growing scientific evidence to support the auricular microsystem theory. However, more research is needed to confirm the mechanisms and efficacy of auriculotherapy and auricular acupuncture.
FundingThis research received no external funding.
Ethical approvalThis review does not require ethical approval.
CRediT statementConceptualization, J.M.R.; data curation, J.M.R., O.M., K.S., G.C. and P.B.S; methodology, J.M.R.; supervision, J.M.R. and J.P.M.; validation, J.M.R and J.P.M.; visualization, J.M.R. and J.P.M.; writing—original draft, J.M.R and K.S.; writing—review and editing, J.M.R, K.S., O.M., G.C., P.B.S. and J.P.M.
All authors have read and agreed to the published version of the manuscript.