


To identify the feasibility of 2 cardiorespiratory function field-based tests on adults with Down syndrome.
MethodsThirty-three adults with Down syndrome (mean age 27.21±8.76 years; 60.6% men) carried out the Mini-Cooper Test (MC) and the 16m shuttle run test (16-m PACER). During the performance of both tests, heart rate was monitored with the aim of measuring the degree of effort shown by the participants. The Pearson correlation coefficient was used to assess the level of concordance between both tests.
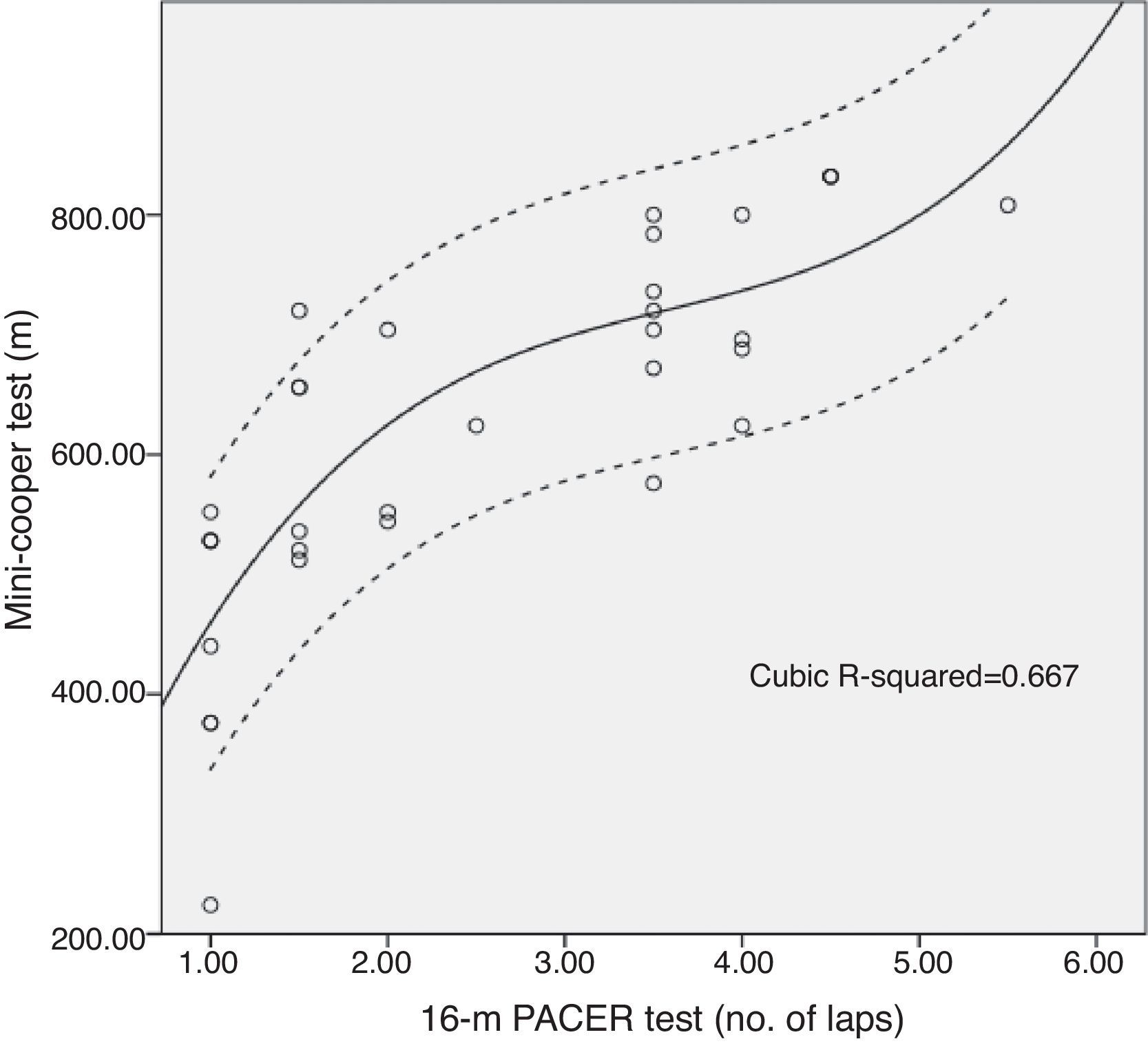
ResultsBoth the MC and the 16-m PACER were easy to administer, and understandable for all the participants. Significant differences were observed by sex. Men achieved greater distances than women in the MC (529.23±127.45 vs. 690.00±126.59m), and reached more stages in the 16-m PACER (1.69±1.07 vs. 3.15±1.28). The analysis of the degree of effort showed that final heart rate obtained at the end of both tests were around 90% of the predicted maximum heart rate. A significant degree of correlation between the MC and the 16-m PACER was observed both in men (r=0.567; sig=0.043) and in women (r=0.797; sig=0.001).
ConclusionThe results of this study suggest that the MC and the 16-m PACER test can be safely performed by adults with Down syndrome in order to assess their cardiorespiratory function.
Determinar la aplicabilidad de 2 pruebas de campo de valoración de la eficiencia cardiorrespiratoria en personas adultas con síndrome de Down.
MétodosTreinta y tres adultos con síndrome de Down (edad media 27,21±8,76 años; 60,6% hombres), realizaron las pruebas Mini-Cooper Test (MC) y Carrera de 16 metros de ida y vuelta (16-m PACER). Se monitorizó la frecuencia cardiaca durante la ejecución de las mismas a fin de comprobar el grado de maximalidad demostrado por los participantes. El grado de correlación de ambas pruebas fue analizado mediante el coeficiente de correlación de Pearson.
ResultadosTanto el MC como la prueba 16-m PACER demostraron ser de fácil aplicación y comprensión por parte de los participantes. Se observaron diferencias significativas en base al sexo a favor de los hombres tanto en los metros recorridos en el MC (529,23±127,45 vs. 690±126,59) como en el número de paliers alcanzados en el 16-m PACER (1,69±1,07 vs. 3,15±1,28). El análisis de la maximalidad realizado determinó una frecuencia cardiaca final en torno al 90% de la frecuencia cardiaca máxima estimada al finalizar ambas pruebas. El grado de correlación observado entre el MC y el 16-m PACER fue significativo tanto para los hombres (r=0,567;sig=0,043) como para las mujeres (r=0,797;sig=0,001).
ConclusionesLos resultados de este estudio sugieren que las pruebas MC y 16-m PACER pueden ser aplicadas a personas adultas con síndrome de Down de manera segura, al objeto de valorar su eficiencia cardiorrespiratoria.
Cardiorespiratory function (CRF) is considered a highly relevant health marker that should be properly evaluated from early ages.1 This is especially true for the individuals with Down syndrome (DS), who generally have a high level of physical inactivity.2 In addition, people with DS usually have cardiovascular and metabolic abnormalities and problems in regulating and controlling their autonomic nervous systems that affect CRF negatively3 and, consequently, their health. That is why individuals with DS should have their CRF assessed with certain regularity and appropriately, using specific tests with previously demonstrated applicability for this population. Laboratory stress tests are considered the gold standard in this regard, as they make it possible to establish CRF under controlled conditions and in a valid, reliable way.4 However, performing this type of tests is limited by the availability of physical resources that are generally expensive. It is also limited by the presence of specialised staff to administer such tests and monitor their correct performance, which should be individualised. That is why field tests are so commonly used to assess CRF, due to their simplicity and low administration cost and the fact that they permit simultaneous assessment of various individuals in a short time. Despite this, and against what could be expected, the field tests to assess CRF in people with DS are few and almost all of them have been developed only with young and generally foreign populations.5,6 It consequently seems necessary to analyse the usefulness of field tests applied to the Spanish adult population with DS. This will make it possible to provide information about which of these tests are more recommendable for assessing CRF in adults with DS; in addition, such an analysis will present mean values as a guide to make it easier to identify the CRF level once carried out by a population similar to the reference population. In this situation, the objective of this study was to analyse the usefulness of 2 field-based CRF tests when they are administer to a group of adult Spaniards with DS.
Material and methodsParticipantsThe participants in this study were recruited through an invitation sent to 2s [sic] DS associations in the south of Galicia (Spain). The criteria for inclusion were as follows: (a) the presence of trisomy 21, (b) being an adult and (c) being capable of understanding and following simple instructions. All individuals that had any type of documented partial or total medical contraindication against performing intense physical activity were excluded from the study. The research ethics committee at the University of Vigo (Spain) approved this study. All the parents or legal guardians of the participants were informed as to the study objectives and methodology of the tests to be performed and then gave their written consent. They also provided information about the chronological age and sex of the participants.
Field testsWe selected 2 tests that were feasible to carry out in a covered sports installation having a uniform surface covering and comfortable temperatures and humidity.
Mini-Cooper TestThis test is an abbreviated version of the Cooper Test, which has been considered valid for assessing CRF in healthy populations.7 It consists of covering the maximum possible distance running, walking, or alternating both running and walking, for 6min. Once the test is finished, the distance in metres covered is recorded.
Sixteen-metre shuttle run testThe initial objective of this study was to analyse the applicability of a 20-m shuttle walk/run test validated for assessing CRF in healthy populations. However, a small pilot study with part of the recruited sample revealed that the participants found it very difficult to cover the distance established at the performance rhythm set in the protocol. Consequently, we decided to administer the 16-metre shuttle run test (16-m PACER [progressive aerobic cardiovascular endurance run]), which is a shorter distance test that has been adapted and validated in adolescents with intellectual disability.8 This test consists of finishing a previously established distance by running/walking back and forth. Test rhythm is set by an audio signal that indicates the time in which the participants have to cover a distance and, consequently, determines their speed. This is an incremental test in which the speed increases at 1-min intervals, called laps (palieres), until exhaustion. The test ends when the participant, in 2 consecutive tries, is incapable of completing the 16-m course before the signal sounds. The last lap completed is then recorded.
ProcedureThis transversal study lasted 6 weeks. During the first 2 weeks, we performed a pilot study to explain and trial the administration protocols of the Mini-Cooper (MC) and the 16-m PACER tests, and performed an anthropometrical assessment of the study sample. Height was evaluated using a stadiometer (SECA®, Model 217), weight was evaluated using an electronic weight scale (SECA®, Model 899) and waist circumference with a non-extensible measuring tape (SECA®, Model 203) following standard protocol. Body mass index was calculated as weight (kg)/height (m2). Finally, a pulsometer (Polar RS400, Kempele, Finland) was used to obtain the basal heart rate (HR) basal of the participants.
There was no intervention at all during the third and fifth weeks. Throughout the fourth and sixth weeks, the MC and the 16-m PACER tests were administered, respectively. To administer the MC test, a 16×16m2 was established with 8 cones to help the participants run around its perimeter, like a “rope”. For the shuttle test, a distance of 16m was established with cones, leaving a space of 2m to turn. The test began with an audio signal that marked the initial test speed of 8.5km/h; this was increased bit by bit by 0.5km/h/min (per lap), so that the time interval between the 2 signals was reduced each minute that passed.
Both tests were carried out with small groups, after a previous guided warm-up. Auxiliaries were allowed to collaborate to give a verbal reference of the test rhythm to motivate and encourage the participants to perform the test to the best of their ability. The protocol for both tests included a single preliminary trial.
To identify the maximum for each of the field test, the maximum HR of the participants was estimated through an equation proposed and validated for adults with DS9 and their HR was monitored during the tests. This maximum was defined as the percentage of the maximum HR reached by each participant calculated based on the HR recorded at the end of each test. Trained staff with previous experience in specifying physical exercise for individuals with DS performed all the assessments.
Statistical analysisThe descriptive analysis of the data is presented over-all and stratified by gender, through the mean and standard deviation. Normality of the sample was checked using the Kolmogorov–Smirnov test (P>.005). The existence of statistically significant differences between the sexes was verified using Student's T-test for independent data. A correlation analysis was performed using the Pearson correlation coefficient to analyse the relationship between the parameters – age (years), body mass index (kg/m2), MC (m) and 16-m PACER (no. of laps). The statistical software used in the statistical analyses was the SPSS Statistics 21 (SPSS Inc. Chicago, IL, USA). The level of statistical significance set for all analyses was a P-value of 0.05.
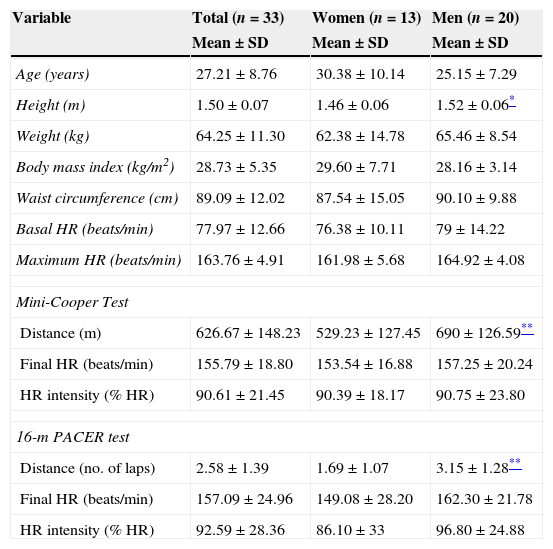
ResultsA total of 33 adults with DS (mean age 27.21±8.76 years; 60.6% males) presented themselves as volunteers and finished the study. Their characteristics are shown in Table 1. No great difficulties or adverse events were observed during the administration of the MC and the 16-m PACER tests. The participants found both tests to be easily carried out and easily understood. After the tests ended, statistically significant differences were found in CRF based on sex in favour of the men, both in metres covered in the MC test (529.23±127.45 vs 690±126.59) and in the number of laps achieved in the 16-m PACER test (1.69±1.07 vs. 3.15±1.28). The analysis of the maximum performed established that the participants reached a final HR in both tests around 90% of the estimated maximum HR (Table 1). The degree of correlation observed between the MC and 16-m PACER tests was statistically significant for both the men (r=0.567; significance=0.043) and the women (r=0.797; significance=0.001). Fig. 1 presents the concordance of the 2 tests, taking the entire study population as reference.
Characteristics of the participants and mean values reached.
| Variable | Total (n=33) | Women (n=13) | Men (n=20) |
|---|---|---|---|
| Mean±SD | Mean±SD | Mean±SD | |
| Age (years) | 27.21±8.76 | 30.38±10.14 | 25.15±7.29 |
| Height (m) | 1.50±0.07 | 1.46±0.06 | 1.52±0.06* |
| Weight (kg) | 64.25±11.30 | 62.38±14.78 | 65.46±8.54 |
| Body mass index (kg/m2) | 28.73±5.35 | 29.60±7.71 | 28.16±3.14 |
| Waist circumference (cm) | 89.09±12.02 | 87.54±15.05 | 90.10±9.88 |
| Basal HR (beats/min) | 77.97±12.66 | 76.38±10.11 | 79±14.22 |
| Maximum HR (beats/min) | 163.76±4.91 | 161.98±5.68 | 164.92±4.08 |
| Mini-Cooper Test | |||
| Distance (m) | 626.67±148.23 | 529.23±127.45 | 690±126.59** |
| Final HR (beats/min) | 155.79±18.80 | 153.54±16.88 | 157.25±20.24 |
| HR intensity (% HR) | 90.61±21.45 | 90.39±18.17 | 90.75±23.80 |
| 16-m PACER test | |||
| Distance (no. of laps) | 2.58±1.39 | 1.69±1.07 | 3.15±1.28** |
| Final HR (beats/min) | 157.09±24.96 | 149.08±28.20 | 162.30±21.78 |
| HR intensity (% HR) | 92.59±28.36 | 86.10±33 | 96.80±24.88 |
SD: Standard deviation; HR: heart rate.

Cardiorespiratory function contributes positively to the autonomy of adults with DS, given that it has a close relationship with functional capacity.10 Consequently, it seemed necessary to identify which field-based tests can be useful in evaluating this population. The results of this study contribute to this proposition, as we studied the applicability of the MC and 16-m PACER tests when administered to adults with DS. The MC test is generally administered to school-age boys/girls; the authors of this study have no knowledge of any studies in which it was administered to cohorts with DS. It is thus not feasible to compare the mean values obtained in this test by our study participants. At any rate, its administration did not cause the participants great difficulties in maintaining test cadence and rhythm and in supporting fatigue. These problems have indeed been seen when individuals with intellectual disability performed the Cooper Test,11 which counts in favour of the usefulness of the MC test in an adult population with DS.
Different researchers have studied the applicability of the shuttle test, in both the 16-m and 20-m versions.9,12,13 However, in those studies and in the few cases in which that test has been given to samples specifically composed of individuals with DS,14–18 adults have not been included as part of the population to evaluate, with a single exception.19 In that study, similar mean values were seen for the males; however, the means found for the females were distinct from those found in our study. These differences might be due to the different ethnic origin of the 2 populations, which would indicate the need to develop further studies of this type with autochthonous samples.
The lack of observable difficulties in the development of both tests and the existence of a high degree of correlation between them are 2 aspects that should be ratified to confirm the applicability of these tests.20 In this study, both criteria are fulfilled. Not only that: the results obtained indicate that both the MC and 16-m PACER tests can be considered as maximum stress tests when they are performed by adults with DS, judging by the percentage of maximum HR reached by the end of the tests. These findings suggest that the MC and the 16-m PACER are field-based tests that can be used to assess CRF in this population. However, it should be pointed out that it is impossible to estimate maximum oxygen consumption based on these tests. In the case of the MC test this is because, as far as the authors have found, it has not been administer to individuals with DS and no method has consequently been developed; and in the case of the 16-m PACER this is because it has been seen that the equation used for populations with intellectual disability is invalid for people with DS.14,17 At any rate, both tests can indeed be used for establishing the capacity to economise effort and for assessing the effect of various interventions aimed at improving CRF in adults with DS; these capabilities have been observed for other populations in which it is at present impossible to estimate the maximum oxygen consumption based on this type of field tests.21
In spite of the originality of this study, we should acknowledge certain methodological weaknesses inherent to its design and which limit transferring the results presented. The main ones are the small sample size and the lack of information about the participants’ intellectual coefficients, a factor that strongly affects the way that adults with DS carry out CRF tests.22
In short, the results of this study show that the MC and 16-m PACER tests can be applied with adults with DS safely, with the objective of assessing their CRF. Future studies should analyse the reliability and validity of these tests when administered in this population.
Conflicts of interestsThe authors have no conflicts of interest to declare.