








The objective of this study is to identify the need for basic first aid knowledge and skills among adolescents.
MethodA cross-sectional study using multistage sampling was conducted among 375 secondary school students in Kuantan, Pahang, Malaysia. The survey was adapted from a Hong Kong Red Cross survey. A back to back translation of this instrument was carried out by two bilingual medical experts with Cronbach's alpha 0.8. The data were analyzed using SPSS (Statistical Package for the Social Sciences) in terms of descriptive analysis, and an independent t-test and chi-square test were carried out.
ResultsThere were 149 respondents from the lower form (grade level) and 226 respondents from the upper form. The majority of respondents (81.6%) were Malay. An independent t-test revealed a significant association between knowledge and attitude, as students who scored higher on first aid questions showed a more positive attitude towards first aid (1.475%). There were also significant associations between race and experience learning first aid.
ConclusionsAdolescents receive minimal first aid education. Thus, there is an urgent need to educate adolescents more in first aid to promote a safer community and to prevent any further injuries.
First aid literally means the very first assistance or immediate care given to a person who is injured or suddenly becomes ill. The American Heart Association defines first aid as the assessments and interventions that can be performed by a bystander (or victim) with minimal or no medical equipment1. First aid also includes initiating the activation of an emergency medical services (EMS) system or soliciting other medical assistance by calling an emergency line, which in Malaysia is 999. In an emergency situation, lack of first aid knowledge can lead to injury and disability and even unnecessary death, as first aid includes recognizing life-threatening conditions and taking appropriate action to keep the injured or ill person alive and in the best possible condition until medical treatment can be acquired. As stated by Başer et al.2, adolescents are exposed to various injuries and illnesses and require first aid more often than adults. They experience accidents and injuries more frequently relating to physical activities at school and in their neighborhoods. These activities include engaging in school events, such as sports, and also simply playing, riding, swimming, etc. Therefore, in the spirit of the phrase “Better safe than sorry”, it is essential to teach younger generations first aid in order to equip and prepare them to deal with the traumatic effects of an accident, which can prevent them from acting3.
A study conducted in support of the need for educating adolescents in first aid concluded that school children as early as ten years old can already perform BLS (basic life support) appropriately with only one annual training course4. Even though Malaysia has shown rapid development in prehospital care by implementing its universal emergency call system (999) and shortening ambulance response times to eight to ten minutes, it is important to ask the following: Do Malaysian civilians help victims before EMS arrive, and do they even know how to give the correct information for an emergency call?
Although one previous study developed in Malaysia examined secondary school children's knowledge and attitudes pre- and post-CPR training in a district of Kota Bharu, Kelantan5, no previous study has analyzed Malaysian secondary school students’ knowledge and attitudes concerning basic first aid, which does not solely include CPR. Basic first aid applies to various emergencies, such as burns, drowning, poisoning, musculoskeletal trauma, electric injuries, wounds and abrasions, human and animal bites, and other medical emergencies. There were lack of study discussing on how students’ sociodemographic status influences their attitudes and levels of knowledge before they receive first aid training. Therefore, this research is required to determine the relationship between students’ sociodemographic status and students’ attitudes and knowledge concerning first aid. We targeted secondary school students because the adolescent phase is the most appropriate time to learn a fundamental and sophisticated skill. Secondary school students are more active, focused, and energetic. They also like to challenge themselves and engage in activities that require an adrenaline rush. Our research was approved by the Kulliyyah (Faculty) of Nursing Research Committee and the International Islamic University Malaysia Research Ethics Committee. In addition, this research was approved by the Ministry of Education through an online application, the Pahang State Education Department, the Kuantan District Education Office, and the school principals. The objective of this study was to identify the need for basic first aid knowledge and skills among adolescents.
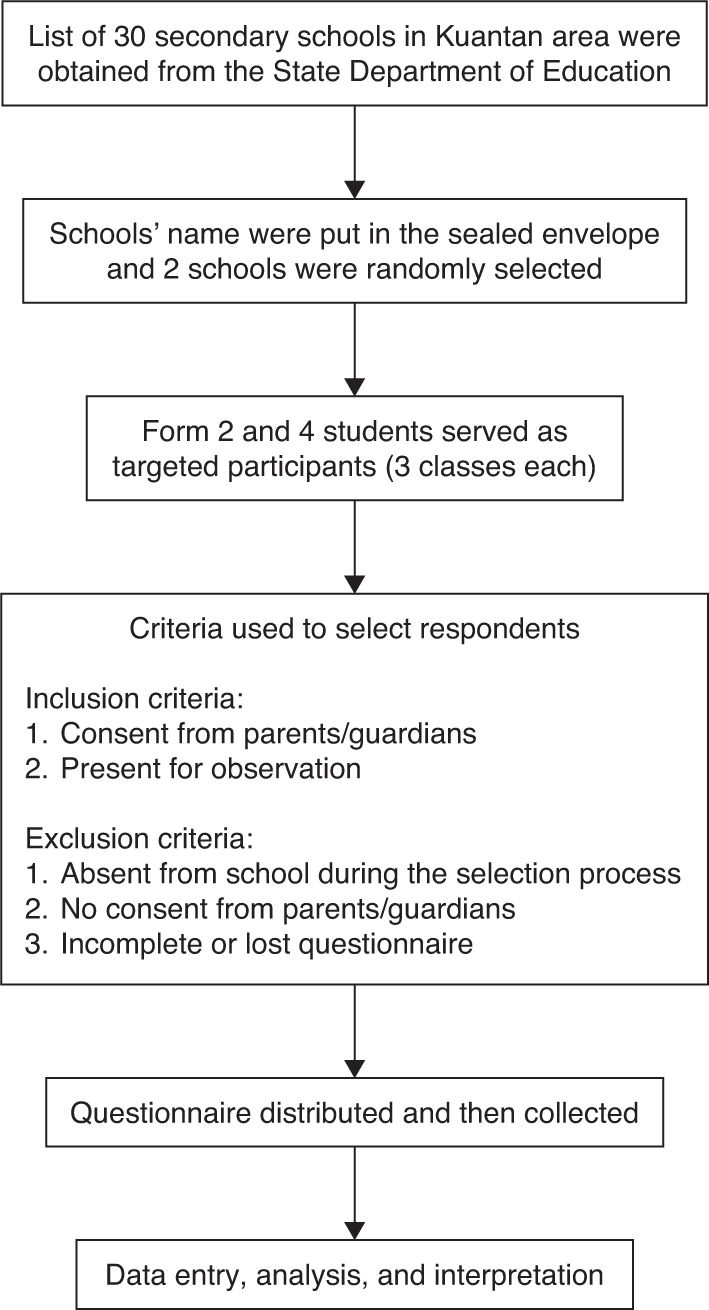
MethodWe conducted a cross-sectional study design involving secondary school students to determine their attitudes, practices, and levels of knowledge concerning first—which can explain the need for adolescents’ first aid education—in a district of Kuantan, Pahang. After obtaining ethical approval from several authorities, we executed the study in a twelveweek time period between February and April of 2015. The list of secondary schools in Kuantan area was obtained from state department of education. The total number of 30 different schools was put in the different sealed envelope. Two envelopes were randomly selected and served as the target population of the study. Students in form 2 & 4 were the targeted participants. They were selected based on the inclusion and exclusion criteria of the study (Figure 1). The inclusion criteria for form two (14-year-olds) and form four (16-year-olds) included students’ ability to understand and read Bahasa Malaysia or English and a parent or guardian's written consent. Exclusion criteria included students’ absence from school on the selection day and student enrollment in the Special Education Division.

We distributed a questionnaire adapted from a questionnaire of the Hong Kong Red Cross. Back-to-back translations and a content expert ensured the reliability and validity of the questionnaire. Two medical experts executed the initial translations from English to Bahasa Malaysia, and a medical expert whose primary language is English conducted the translation back to the English language. We used 20 students to test an early version of the questionnaire, and the participants interviewed indicated that all items of the questionnaire were globally clear and comprehensible. However, after some discussion with the expert committee including first aid trainers and emergency practitioners, we decided to change a few questions and answers to match with situation in Malaysia. The questionnaire contained three parts: Part A, Sociodemographic Data; Part B, Knowledge; and Part C, Attitude.
The first part of the questionnaire (Part A) investigated the sociodemographic data of the participant, including age, gender, race, and experience in first aid training. Part B (on knowledge) consisted of ten structured questions about first aid management, for which students had to select only one best answer. One point was given for each correct answer, and zero points were given for each incorrect answer. The grades ranged from zero to ten points and were converted into a one-hundred-point scale and then measured using the mean and standard deviation (SD). The total possible maximum score on the knowledge domain was seventy points. Lastly, Part C included five statements concerning attitudes on basic first aid. Responses to the statements were measured using a Likert scale: “strongly agree”, “agree”, “no comment”, “disagree”, and “strongly disagree”. Each score was categorized as either a positive or negative attitude.
Using a single proportion sample size calculation, the value of p is the expected proportion of individuals with the characteristics of interest, which can be obtained from the literature (Rahman et al., 2013). Therefore the minimum requirement for a sample size is 361 respondents.
Prior to the data collection, the researcher met the school administration to get permission to include students as respondents. Then we selected classes using simple random sampling, three classes for each form. We identified and approached respondents according to the inclusion and exclusion criteria. Next, we obtained written consent from respondents who were at least seventeen years old. For students under seventeen years of age, we obtained written consent from a parent or guardian. After, this step, the researcher introduced herself and explained the research purposes. The respondents answered the questionnaire themselves, and the session took about twenty to thirty minutes. During the session, the researcher assisted respondents who had difficulty. The respondents returned the completed questionnaires to the researcher, who checked them. All data collected was kept confidential. The data were analyzed using SPSS (Statistical Package for the Social Sciences), and the results of the descriptive analysis were presented in tables by showing the frequency and percentage for the distribution of the data. The results for associations between variables were interpreted based on the significant p-value with a level of significance set as α=0.05. These results were also presented in tables.
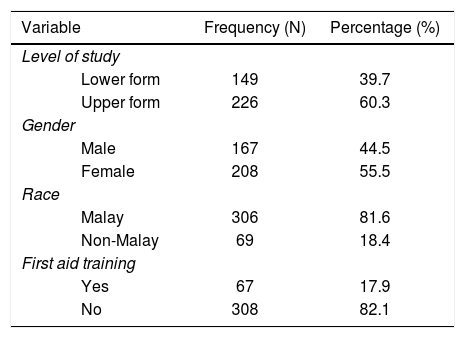
ResultsThis study included a total of 375 respondents, as required by the estimated minimum sample size of 361. All respondents were differentiated in two categories based on their level of study—lower form and upper form. The lower form consisted of secondary school students in form two with ages ranging from thirteen to fourteen years old, and the upper form consisted of students in form four with ages ranging from fifteen to sixteen years old. More than half of the respondents, 226, were from the upper form (60.3%), while the other 149 students were from the lower form (39.7%). Regarding gender, there were 167 male respondents (44.5%) and 208 female respondents (55.5%). Only 69 respondents were not Malay (18.4%), and the majority of respondents, 306, were Malay (81.6%). Meanwhile, regarding experience learning first aid, there were only 67 responses total for yes (17.9%) and 308 responses for no (82.1%). Table 1 presents the detailed distribution of sociodemographic data among the respondents.
A questionnaire with a total of ten questions measured the students’ level of knowledge on basic first aid. As presented in Table 2, the mean total knowledge score for 375 secondary school students was 33.89 (15.033) (with a maximum score of 70). Attitudes on basic first aid among adolescents were categorized as positive and negative. Table 2 also shows that 45.1% of respondents (169 out 375) had a positive attitude towards the administration of first aid in real life and 54.9% of respondents (206 out of 375) had a negative attitude. Based on the data analysis using an independent t-test, there was a significant association between knowledge and attitude (interrelated): t=4.029; p=0.001. Table 3 shows these results in detail.
According to the data analysis using the independent t-test, there also was a significant association between race and knowledge of basic first aid: t=−2.694 and p=0.009 (Table 4). Similarly, there was also a significant association between experience learning first aid and knowledge of first aid: t=3.262. Using the chi-square test, there was a significant association between race (chi-square=12.304, p=0.001) and experience in learning first aid (chi-square=7.057; p=0.006) with attitude (Table 5). Sociodemographic status, level of study, and gender showed no significant association with attitude towards basic first aid, with chi-square=2.772, p=0.06 and chi-square=1.436, p=0.137 (Table 5). Regarding age, an independent t-test was used to determine the value of t, and there was no significant association between age and attitude, since t=0.601 and p=0.555. Table 5 shows these results in detail.
Association between adolescents’ sociodemographic status and knowledge of basic first aid.
| Sociodemographic status | Knowledge, mean (SD) | R-valuea | P-value |
|---|---|---|---|
| Age | 33.89 (15.03) | −0.020 | 0.697 |
| Knowledge, mean (SD) | T-valueb | P-value | |
| Level of study | −1.334 | 0.179 | |
| Upper form | 33.05 (15.26) | ||
| Lower form | 35.17 (14.64) | ||
| Gender | 0.759 | 0.444 | |
| Male | 34.55 (14.34) | ||
| Female | 33.37 (15.58) | ||
| Race | −2.694 | 0.009c | |
| Malay | 32.91 (14.86) | ||
| Non-Malay | 38.26 (15.14) | ||
| First aid training | 3.262 | 0.001c | |
| Yes | 39.25 (14.70) | ||
| No | 32.73 (14.87) |
Association between adolescents’ sociodemographic status and attitude towards basic first aid.
| Sociodemographic status | Attitude, mean (SD) | T-valuea | P-value | |
|---|---|---|---|---|
| Positive | Negative | |||
| Age | 15.14 (1.35) | 15.21 (1.15) | 0.601 | 0.555 |
| Attitude, n (%) | Chi-square-valueb | P-value | ||
| Positive | Negative | |||
| Level of study | 2.772 | 0.060 | ||
| Upper form | 94 (41.6) | 132 (58.4) | ||
| Lower form | 75 (50.3) | 74 (49.7) | ||
| Gender | 1.436 | 0.137 | ||
| Male | 81 (48.5) | 86 (51.5) | ||
| Female | 88 (42.3) | 120 (57.7) | ||
| Race | 12.304 | 0.001c | ||
| Malay | 151 (49.3) | 155 (50.7) | ||
| Non-Malay | 18 (26.1) | 51 (73.9) | ||
| First aid training | 7.057 | 0.006c | ||
| Yes | 40 (59.7) | 27 (40.3) | ||
| No | 129 (41.9) | 179 (58.1) | ||
Unintentional injuries and injury-related mortalities of school-aged children and adolescents have become a global concern, as these incidents reflect the status of a region's health care services, a region's social setup, and the psychological mindset of a population6. The implementation of first aid training in schools is widely considered an excellent intervention in this problem. A study by Kanchan & Menezes emphasized that traffic injuries were mainly responsible for injury-related death among children and adolescents in Manipal, India6. The study also found that there are twice as many male mortalities as female ones and that more than 25% of global accidental deaths occur in Southern Asia. Basically, Malaysia also faces the same challenges, with increases in its population, road accidents, injury-related illnesses, heart disease, chemical and environmental hazards, and domestic accidents. Adolescents form a vital group of the total population, and, due to their vulnerability to both physical and emotional hazards, they are exposed to many fatal conditions. But injury and death can be largely prevented through appropriate school-based programs with injury prevention strategies developed by school administration.
This study examined an adolescent population from the area of Kuantan, Pahang, whose ages ranged from thirteen to sixteen years old. All respondents were categorized according to their level of study. More than half of the sample size (60.3%) included respondents in the upper form category of secondary school (form four), and the remaining respondents were in the lower form (form two). Regarding gender, male and female respondents were relatively unequal in number. We expected to have more female respondents, as they are greater in number in both schools. Thus, female respondents dominated this study, taking up 55.5% of the total sample size.
The majority of respondents were Malay, and a small number of non-Malay participants were Chinese, Indian, and other ethnicities. This is due to both schools’ limited intake of Chinese and Indian students, especially SMK Beserah, which is located more than ten kilometers from the city of Kuantan. Only 17.9% of respondents answered yes regarding having experience learning first aid. We also expected this, since the Malaysian education system does not emphasize first aid and has no compulsory syllabus for first aid in schools. In this study, level of knowledge was crucial, as it was a benchmark for what the students knew regarding fast emergency treatment given by a layman. The mean first aid knowledge score of mean (SD), 33.89 (15.033), (out of a maximum score of 70) is actually consistent with a study by Rahman et al.5, who had an intervention and control group score during pre-intervention of about 62.29 (13.68) and 62.20 (12.11), respectively (out of a maximum score of 72).
Another interesting finding was that some students provided their own answers based on the questions or situations given in the survey, even though we instructed them to choose one best answer. This means that some participants already had experience with first aid or knew what to do for a victim even though the management was wrong. This emerged from the questions regarding scalding and blister management (e.g., applying toothpaste) and questions regarding what to do when a foreign object (e.g., sand) is in someone's eye (using Eye-Mo, ophthalmic decongestants, anti-allergens, or analgesics). This study also found that, although the students had already acquired some sort of first aid training, they did not answer questions correctly. Some incorrect answers included using one's mouth to suck venom out of snakebite, inserting tissue paper to stop a nosebleed, or giving someone a mouthful of rice to resolve a choking problem. Intervention study done by Conolly et al. found that knowledge decreased considerably after six months (82.7% vs. 61.1%, p < 0.001) but remained significantly higher than the baseline (61.6% vs. 46.8%, p < 0.01)7. These errors are probably due to problems in retention of memory among participants.
The students’ level of knowledge and attitudes concerning first aid revealed how limited first aid education is in secondary schools. Only 45.1% of respondents showed a positive attitude towards first aid. This finding supports previous research by Chew and Yazid, which showed only half of medical and dental students (51.4% and 45.5%) have a positive attitude towards first aid, which they revealed by telling a crowd that they are health care students and that they offer to do CPR when they witness a cardiac arrest in an out-of-hospital setting8. In addition, some of Chew and Yazid's participants (in response to question fourteen) expressed that they truly supported the idea of first aid as the responsibility of medical professionals in order to save life. This trend is quite worrying, because what happens if people who witness a medical emergency cannot provide first aid on the scene? First aid education benefits secondary school students by making them responsible adults and instilling a caring attitude in them. However, as mentioned by Chew and Yazid, students in Malaysia are influenced by their culture and religion8. Students’ unwillingness to perform first aid might be due to low confidence, fear of making mistakes, or reluctance to touch victims of a different gender. However, the students had a very positive attitude if the victim was a family member8.
In this study, the first objective was to identify the association between secondary school students’ knowledge level and attitude concerning basic first aid. The findings support the study's hypothesis; students with a higher level of knowledge (more correct answers) showed a much more positive attitude towards first aid. With a significant value of t=4.029 and p < 0.05; including a small difference between positive attitude (37.28 [14.75]%) and negative attitude (31.12 [14.72]%), it is clear knowledge truly makes an important contribution to a student's approach when dealing with emergency situations. Most of the study's results support this idea, suggesting that learning basic first aid causes adolescents and children to become much more confident and brave in the face of emergency conditions.
This study measured four areas of sociodemographic status: level of study (upper form and lower form); gender (male and female); race (Malay and non-Malay); and experience learning first aid (some experience or no experience). The data only showed a significant association between race and experience learning first aid. By differentiating the value of the mean (SD) between races, the study found that the non-Malay students had a higher level of knowledge, with 38.26 (15.142%), while Malay students showed a lower level of knowledge, with 32.91 (14.341%). Since the majority of non-Malay students in the study were Chinese, it can be said that Chinese adolescents have much more exposure to information regarding first aid management. However, due to the small sample size of non-Malay respondents, caution must be applied to this logic. Contrary to our expectation that female students would score higher than male students, which was based on a study by Al-Khamees Nedaa7, this study did not find a significant difference between gender and level of knowledge. Based on their finding, Al-Khamees Nedaa suggested targeting first aid education to more males9. However, our study did not show a specific need for this. Rather, our result seems to be consistent with another study, which showed a significant difference in the level of knowledge between different groups (the intervention group and the control group) but no difference between genders7.
The same positive correlation was found between race and experience in learning first aid and also attitude among the 375 respondents. As mentioned before, attitude towards first aid correlated with level of knowledge. Thus, a clear significant association between race (non-Malay) and attitude was shown. This is in agreement with studies by Kuramoto et al.10, which showed that having CPR training is closely associated with willingness to attempt CPR. Our study showed that 59.7% respondents with experience in first aid courses had a positive view on first aid. Once again, an expectation we had based on Al-Khamees Nedaa's9 findings did not play out. The observed differences between levels of study and between younger and older students were not significant, as both levels (the upper and lower forms) in this study showed an equally negative attitude. This attitude was mainly revealed by questions thirteen, fourteen, and fifteen: Learning first aid is very difficult. It is the responsibility of a medical professional to save life and to give first aid, and if I have adequate first aid knowledge and skill, I will perform first aid for people in need. Although the factors that influenced the students’ mindset are unclear, the study showed that a greater effort may be needed to introduce first aid courses to secondary school students, as most respondents were not keen to be the one who provides first aid in a medical emergency (negative attitude: 54.9%).
We see the same patterns and associations of attitude, knowledge level, and sociodemographic status in many studies, especially a Rahman et al.’s study5, which was conducted in the district of Kota Bharu, Kelantan. However, we did not take into account Rahman et al.’s results for different areas (rural and urban), as both schools in our study were in a strategic location and had been transformed by rapid development and modernization. As a result of our respondents’ low level of knowledge and low level of positivity towards first aid administration, as well as the effects/consequences of having first aid courses in school, we conclude that basic first aid education for adolescents is highly needed. First aid education has a great impact; it can change the way adolescents both think and act (thus reducing risky behavior). Having first aid courses in secondary schools can also encourage the dissemination of first aid knowledge to the wider public, including adults, who are less likely to practice first aid11. Hence, it is highly supported that first aid should be a compulsory subject in schools, even if it requires extensive effort for students and administrators alike3.
This study had several limitations. First of all, the time allotted for data collection was limited. The researcher had to wait for ethical approval from the Ministry of Education and other related authorities. In addition, some of the respondents were not counted in the data, as the researcher was unable to get consent from their parent or guardian. Also, several limitations inherent to the questionnaire model were inevitable. For example, there were a few missing values from the respondents on the questionnaires because they did not give only one best answer; rather, they picked two or wrote their own answer on the page. This study was also limited in its ability to determine students’ skills in implementing first aid, as a survey cannot actually elicit the correct attitude of respondents regarding whether they would administer first aid and truly help people in need. Furthermore, since the data was gathered mostly with the help of a counseling teacher and a classroom teacher, there are inherent possibilities that respondents answered dishonestly. Lastly, since most of the respondents were Malay, the results might be influenced by differences in culture, ethics, and other social circumstances.
We have shown that level of knowledge of first aid has a significant association with attitude. This means that students who score higher on first aid knowledge tend to have a much more positive attitude towards first aid. As for sociodemographic factors, adolescents’ race and experience learning first aid have a significant association with their knowledge levels and attitudes concerning basic first aid. Gender and level of study have no associations at all, supporting most previous research concerning knowledge and skills regarding CPR and first aid. Lastly, as a result of respondents’ low level of knowledge and low level of positivity towards first aid administration, as well as the effects/ consequences of having first aid courses in school, we conclude that basic first aid education for adolescents is highly needed in the education system.
We acknowledge the Hong Kong Red Cross Survey on Knowledge and Attitude in First Aid. Our survey is an interpreted copy. The Malaysian translation thereof is for reference only, and the English version supplied by the Hong Kong Red Cross shall always prevail in the case of discrepancies or in consistencies.
