


Identify risk factors that determine pneumonia development in patients who have undergone cardiac surgery.
MethodsProspective study of a single cohort in a postoperative intensive care unit at a tertiary care center, encompassing all patients undergoing cardiac surgery from January to July 2014.
Results31 postoperative pneumonia cases were enrolled out of 211 patients (14.6%). The following independent risk factors were identified: hypertension (OR: 3.94, p=0.01), chronic renal failure (OR: 13.67, p=0.02), reintubation (OR: 22.29, p=0.001) and extubation after 6h (OR: 15.81, p=0.005).
ConclusionsMain determinants for pneumonia after surgery were hypertension, chronic renal failure, extubation after 6h and reintubation.
Identificar los factores de riesgo para desarrollar neumonía en el periodo postquirúrgico de pacientes sometidos a cirugía cardiaca.
MétodoEstudio de cohorte prospectiva que incluye pacientes>18 años sometidos a cirugía cardiaca de enero a julio de 2014, en el Instituto Nacional de Cardiología Ignacio Chávez, México D.F. Se considera un valor de p<0.05 como significativo.
ResultadosDe un total de 211 pacientes operados, se diagnosticaron 31 casos de neumonía postquirúrgica (14.6%). Se identificaron los siguientes factores de riesgo independientes para desarrollar neumonía: la hipertensión arterial sistémica (OR: 3.94, p=0.01), el antecedente de insuficiencia renal crónica (OR: 13.67, p=0.02). La reintubación (OR: 22.29, p=0.001) y permanecer intubado por más de 6 horas (OR: 15.81, p=0.005).
ConclusionesLos principales factores de riesgo independientes para desarrollar neumonía en el periodo postquirúrgico son la preexistencia de hipertensión arterial sistémica o insuficiencia renal crónica, la reintubación y permanecer intubado durante más de 6h.
Post-operative pneumonia is the most common acquired infection after cardiac surgery, with a prevalence rate between 2 and 13%,1–4 most commonly during the first week after surgery.2,5 It is associated with longer hospitalization6–8 and a mortality rate between 15 and 45%.9
Multiple risk factors have been identified for the development of postoperative pneumonia; most relevant studies have analyzed patients diagnosed with ventilator associated pneumonia (VAP).4,10,11 However VAP is not the only form of postoperative pneumonia; up to 43% of registered cases of postoperative pneumonia do not meet VAP criteria.12
Published literature on this topic have not focused on a predominantly Hispanic population, our group has set out to investigate which risk factors contribute to the development of postoperative pneumonia within our Mexican population. The main goal was to identify risk factors for the development of postoperative pneumonia in patients who have undergone cardiac surgery in a Mexican population at a third level hospital and compare results with those previously published.
MethodsPatient selectionData was collected from patients who were ≥18 years old and had been through a cardiac surgery procedure between January and July 2014 at our institution.
Operative criteriaAny patient with postoperative pneumonia diagnosed during the first 7 days following surgery.
The diagnosis of postoperative pneumonia relied on established clinical, radiological and microbiological criteria, and was confirmed by quantitative cultures ≥103 colony forming unit/ml.
Statistical analysisNumeric variables were summarized by mean and standard deviation depending on its distribution or median and interquartile range. Kolmogorov Smirnoff test was applied to all population and groups. Categorical variables were summarized by frequency and percentage.
A quantitative univariate analysis of independent groups was done with Student's t-test or Mann–Whitney U-test, depending on its distribution. Categorical variables analyses were done with Chi-square or Fisher exact test depending on expected values. Those variables with a p-value less than 0.05 were introduced in a logistic regression model for multivariate analysis. Significant p-values were those less than 0.05.
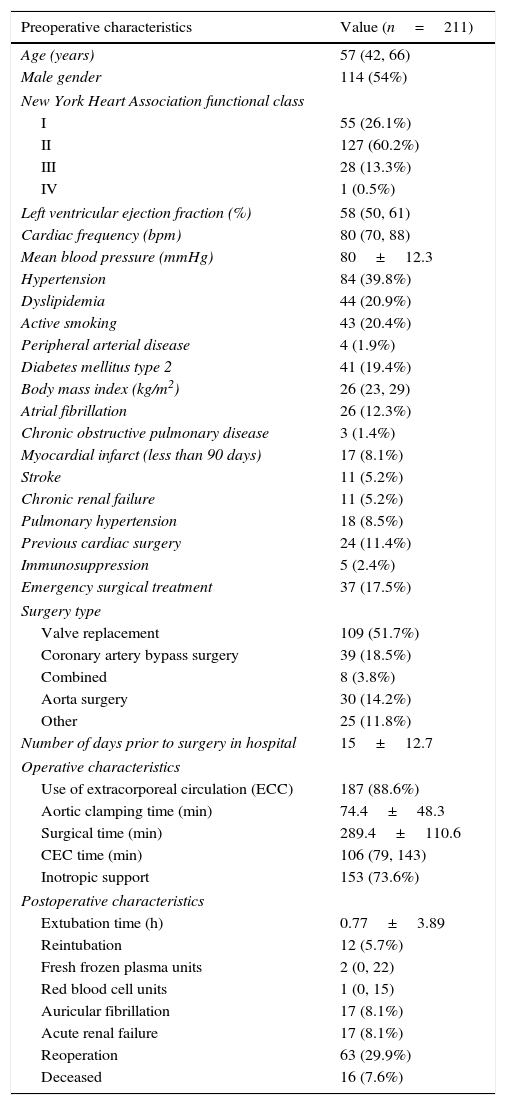
ResultsPopulation characteristicsData was collected from 211 patients who underwent cardiac surgery, the average age was 57 years and 54% of them were men. Before surgery, 13.8% were in advance New York Heart Association (NYHA) functional class (III–IV), with a median left ventricular ejection fraction of 58%. Among cardiovascular risk factors, the most dominant was hypertension as seen in 39.8% of cases. Median body mass index (BMI) was 26kg/m2 suggesting most were overweight. Recent myocardial infarction was seen in 17 patients (8%), 14 of these underwent revascularization surgery. 17% were emergency surgery cases. The most common type of surgery was valvular replacement (51%). The average number of days they remained hospitalized prior to the intervention was 14 (2 weeks). General characteristics are shown in Table 1.
Population characteristics.
| Preoperative characteristics | Value (n=211) |
|---|---|
| Age (years) | 57 (42, 66) |
| Male gender | 114 (54%) |
| New York Heart Association functional class | |
| I | 55 (26.1%) |
| II | 127 (60.2%) |
| III | 28 (13.3%) |
| IV | 1 (0.5%) |
| Left ventricular ejection fraction (%) | 58 (50, 61) |
| Cardiac frequency (bpm) | 80 (70, 88) |
| Mean blood pressure (mmHg) | 80±12.3 |
| Hypertension | 84 (39.8%) |
| Dyslipidemia | 44 (20.9%) |
| Active smoking | 43 (20.4%) |
| Peripheral arterial disease | 4 (1.9%) |
| Diabetes mellitus type 2 | 41 (19.4%) |
| Body mass index (kg/m2) | 26 (23, 29) |
| Atrial fibrillation | 26 (12.3%) |
| Chronic obstructive pulmonary disease | 3 (1.4%) |
| Myocardial infarct (less than 90 days) | 17 (8.1%) |
| Stroke | 11 (5.2%) |
| Chronic renal failure | 11 (5.2%) |
| Pulmonary hypertension | 18 (8.5%) |
| Previous cardiac surgery | 24 (11.4%) |
| Immunosuppression | 5 (2.4%) |
| Emergency surgical treatment | 37 (17.5%) |
| Surgery type | |
| Valve replacement | 109 (51.7%) |
| Coronary artery bypass surgery | 39 (18.5%) |
| Combined | 8 (3.8%) |
| Aorta surgery | 30 (14.2%) |
| Other | 25 (11.8%) |
| Number of days prior to surgery in hospital | 15±12.7 |
| Operative characteristics | |
| Use of extracorporeal circulation (ECC) | 187 (88.6%) |
| Aortic clamping time (min) | 74.4±48.3 |
| Surgical time (min) | 289.4±110.6 |
| CEC time (min) | 106 (79, 143) |
| Inotropic support | 153 (73.6%) |
| Postoperative characteristics | |
| Extubation time (h) | 0.77±3.89 |
| Reintubation | 12 (5.7%) |
| Fresh frozen plasma units | 2 (0, 22) |
| Red blood cell units | 1 (0, 15) |
| Auricular fibrillation | 17 (8.1%) |
| Acute renal failure | 17 (8.1%) |
| Reoperation | 63 (29.9%) |
| Deceased | 16 (7.6%) |
Most of them required cardiopulmonary bypass (88%), with a median time of 106min, and a mean aortic cross clamp time of 74min. Seven out of ten patients required inotropic support during surgery.
Average extubation time was 58h, 5.7% required reintubation. One out of three required reintervention. Overall mortality rate was 7.6%.
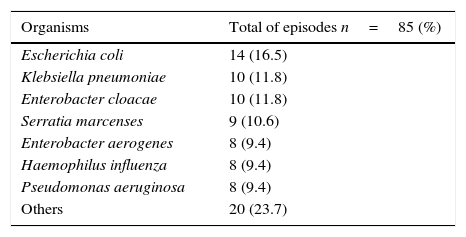
Main isolated microorganisms seen in patients suffering post-surgery pneumonia were Escherichia coli (16.5%), Klebsiella pneumoniae (11.8%) and Enterobacter cloacae (11.8%), see Table 2.
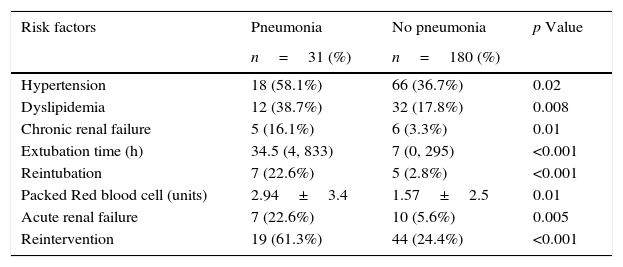
Univariate analyses (see Table 3) evaluated population by outcome and revealed the development of postoperative pneumonia in 31 patients. No significant differences were recorded regarding age, gender, ejection fraction, diabetes mellitus, previous heart attack, pulmonary hypertension, previous cardiac surgery or preoperative immunosuppression status. It was observed that patients who developed pneumonia had hypertension (58 vs 36%, p=0.02), dyslipidemia (58 vs 36%, p=0.02) and chronic renal failure (16 vs 3%, p=0.01).
Univariate analysis of risk factors for postoperative Pneumonia.
| Risk factors | Pneumonia | No pneumonia | p Value |
|---|---|---|---|
| n=31 (%) | n=180 (%) | ||
| Hypertension | 18 (58.1%) | 66 (36.7%) | 0.02 |
| Dyslipidemia | 12 (38.7%) | 32 (17.8%) | 0.008 |
| Chronic renal failure | 5 (16.1%) | 6 (3.3%) | 0.01 |
| Extubation time (h) | 34.5 (4, 833) | 7 (0, 295) | <0.001 |
| Reintubation | 7 (22.6%) | 5 (2.8%) | <0.001 |
| Packed Red blood cell (units) | 2.94±3.4 | 1.57±2.5 | 0.01 |
| Acute renal failure | 7 (22.6%) | 10 (5.6%) | 0.005 |
| Reintervention | 19 (61.3%) | 44 (24.4%) | <0.001 |
The number of hospitalization days prior to surgery was not different between groups. Intra-operative variables, cardiopulmonary bypass time (117 vs 109min, p 0.56), aortic cross clamp time (79 vs 73min, p 0.53), and the use of inotropes support during surgery (25 vs 128min, p 0.33) did not show a significant difference between groups. Patients suffering from pneumonia had a higher need of reintubation (22 vs 2%, p=0.0001), more frequent blood transfusions and developed acute renal failure more commonly (22 vs 5%, p=0.005). Most of these patients required reintervention (61 vs 24%, p=0.0001). Mortality rate was higher for the pneumonia group (22 vs 5%, p=0.003).
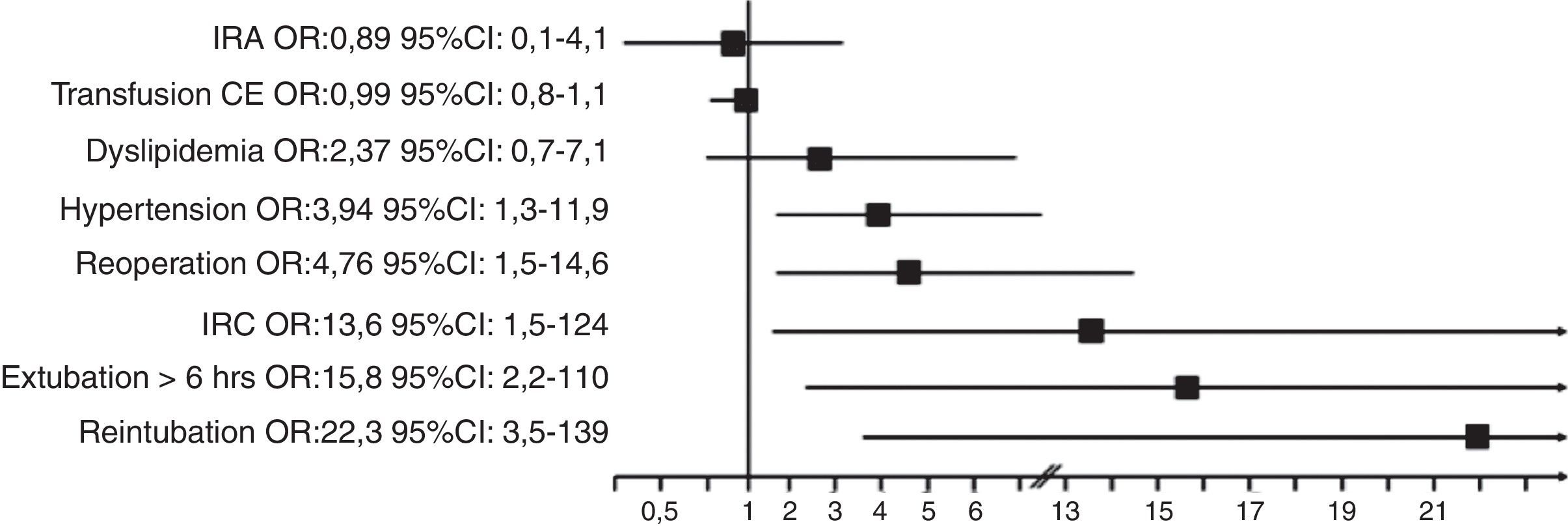
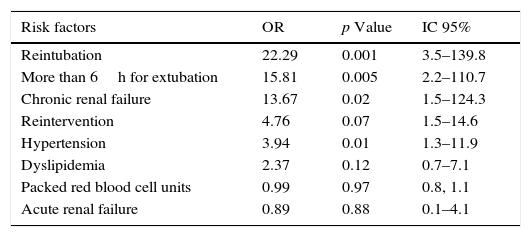
Multivariate logistic regression analysis (see Table 4) showed that the main independent risk factors for postoperative pneumonia development during pre-operative period were hypertension (OR: 3.94, p=0.01) and chronic renal failure (OR: 13.67, p=0.02). Post-operative, reintubation (OR: 22.29, p=0.001) and requiring intubation for more than 6h (OR: 15.81 p=0.005) (Fig. 1).
Multivariate analysis of risk factors for postoperative Pneumonia.
| Risk factors | OR | p Value | IC 95% |
|---|---|---|---|
| Reintubation | 22.29 | 0.001 | 3.5–139.8 |
| More than 6h for extubation | 15.81 | 0.005 | 2.2–110.7 |
| Chronic renal failure | 13.67 | 0.02 | 1.5–124.3 |
| Reintervention | 4.76 | 0.07 | 1.5–14.6 |
| Hypertension | 3.94 | 0.01 | 1.3–11.9 |
| Dyslipidemia | 2.37 | 0.12 | 0.7–7.1 |
| Packed red blood cell units | 0.99 | 0.97 | 0.8, 1.1 |
| Acute renal failure | 0.89 | 0.88 | 0.1–4.1 |

This study confirms the high incidence of pneumonia developed by patients who undergo cardiac surgery (14.6%). As reported in previous studies, a higher incidence of pneumonia was shown in those patients who required more than 48h of intubation after surgery (45.1%).
Our population was younger (56 vs 64.7 years old). Main isolated microorganisms were Enterobacteria; which matches data reported by Allou et al.,11 but differs from Hortal et al.10 results in 2009, that group found that the main microorganisms isolated were Pseudomonas aeruginosa, Staphylococcus aureus and Haemophilus influenza.
Of note, our group identified hypertension as an independent risk factor, to our knowledge this had not been previously reported in this setting. Chronic renal failure did not reach statistical significance in our cohort but previous groups have reported it (Hortal et al.10) Chronic obstructive pulmonary disease was not recorded in those patients developing pneumonia and their age was not an independent risk factor. In contrast to previous reports by Allou et al. and Hortal et al., none of the intraoperative variables reached statistical relevance in our cohort.
While analyzing postoperative variables; atrial fibrillation was not relevant (5 vs 12, p 0.14). The number of blood transfusions seemed to be a relevant factor in the univariate analysis (p=0.01); but did not retain significance when evaluated in the multivariate analysis; interestingly this has also been reported. As expected, those patients who developed pneumonia in the postoperative period had a higher mortality rate.
In our study, the strongest independent predictors for the development of pneumonia were: reintubation, chronic renal failure and requirement of mechanical ventilation for more than 6h. Our identification of hypertension as a novel, relevant risk factor may warrant further investigation as this finding had not been reported previously. Our limitations include: the wide confidence intervals suggesting the need for a greater population, in this single center study.
ConclusionsMain independent risk factors that suggest pneumonia development in postoperative period are hypertension, chronic renal failure, reintubation and the requirement of intubation for more than 6h.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that no patient data appears in this article.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.
FundingNo endorsement of any kind received to conduct this study/article.
Conflict of interestThe authors declare no conflict of interest.