





The aim of this study was to determine whether subjects with advanced hallux limitus show a diminished ability of internal rotation of the lower limb and increased foot progression angle compared with normal population. It was also intended to relate rotational and torsional patterns of lower limbs with the foot progression angle, and to compare three different methods of measurement of the foot progression angle.
Patients and methodsInternal and external rotational pattern, internal and external hip rotation and tibial torsion were measured in 30 feet of 15 subjects with advanced hallux limitus and 103 normal feet. The foot progression angle was also obtained using a pressure platform and an inked latex carpet.
ResultsThe internal rotation of the lower limb was significantly lesser and the foot progression angle was significantly greater in individuals with advanced hallux limitus (p<0.05). The Pearson correlation coefficient was −0.563 (p<0.01) for the relationship between the foot progression angle and the internal rotational pattern. The measure of the foot progression angle in the inked latex carpet was significantly greater than in the pressure platform in the left foot (p<0.05).
ConclusionSubjects with advanced hallux limitus had a lesser capacity of internal rotation of the lower extremity and greater foot progression angle in comparison with normal population. Internal rotational pattern determines the greater foot progression angle. The foot progression angle values measured with the pressure platform differ from those of the inked latex carpet.
Los objetivos de este estudio fueron determinar si los sujetos con hallux limitus avanzado, tienen disminución del patrón rotador interno y aumento del ángulo de la marcha con respecto a la población normal, relacionar los patrones rotacionales y torsionales de la extremidad inferior con el ángulo de la marcha y comparar métodos de obtención del ángulo de la marcha.
Pacientes y métodosEn 15 sujetos con hallux limitus avanzado, se valoró el patrón rotador interno y externo, rotación interna y externa de caderas y torsión tibial. Se obtuvo el ángulo de la marcha con plataforma de presiones y tapiz de látex entintado.
ResultadosEl patrón rotador interno fue significativamente menor y el ángulo de la marcha fue significativamente mayor en individuos con hallux limitus avanzado (P<0,05). El coeficiente de correlación de Pearson fue de −0,563 (P<0,01) para la relación entre el ángulo de la marcha y patrones rotadores internos. El ángulo de la marcha medido en el tapiz de látex fue significativamente mayor que en la plataforma de presiones para el pie izquierdo (P<0,05).
ConclusionesLos sujetos con hallux limitus avanzado tuvieron menor capacidad de rotación interna en la extremidad inferior y mayor ángulo de la marcha en comparación con la población normal. La disminución del patrón rotador interno determina un aumento del ángulo de la marcha. Los valores del ángulo de la marcha de la plataforma de presiones difieren de los obtenidos con el tapiz de látex.
First metatarsophalangeal joint (1st MTP) consist of the first metatarsal head and the base of the proximal phalanx1–3 and it is one of the three rotational parts of the foot that allow a forward continuous progression of the body that is supported by the foot during stance. Because of that, range of motion and sagittal plane mobility of this joint is quite important to allow propulsion in optimal conditions and to avoid compensations that could affect the foot and the whole locomotor system.3
Several anatomic and mechanical factors can have a negative influence in the normal behavior of the 1st MTP joint with a reduction of the normal dorsiflexion range of the joint such us a dorsiflexed first ray deformity, peroneus longus muscle insufficiency, abnormal length patter of the first metatarsal or first digit, sesamoid disorders, a squared head of the first metatarsal and tightness of plantar soft tissues around first metatarsophalangeal joint. All these factors can put the base of the phalanx in a plantarflexed position under the metatarsal head in an attempt to have a more stable medial column. This position of the phalanx prevents the joint to have a normal range of motion into dorsiflexion for normal propulsion predisposing to the development of a hallux limitus deformity3,4 with a limitation of dorsiflexion of 1st MTP joint.3
Lafuente et al.4,5 have showed correlation between 1st MTP joint dorsiflexion and the internal rotation pattern of the lower extremity, which can be described as an exploratory measure that encompasses hip internal rotation, tibial torsion and forefoot adduction. In their study, it was defined which 1st MTP joint dorsiflexion ranges are not possible with a low or small range of internal rotation pattern of the lower extremity. This aspect could be viewed as a new possible etiology explanation of hallux limitus deformity not explored yet.4,6
Limitation of the internal rotation pattern during gait can pose a difficult translation of loads from the external border of the foot to the first ray and loads during midstance would not be enough to dorsiflex the joint. This lack of loads in the medial border generates a plantarflexion of the digit in the proximal phalanx creating an HL. Indeed, it has been shown that the internal rotation pattern has a negative correlation with the foot progression angle and a reduction of the internal rotation pattern is associated with an increase in the foot progression angle.4
This increase in foot progression angle is a common clinical observation in people with HL. However, it is not clear weather this increase is the causing mechanism of HL deformity, as has been mentioned before,4,5 or is the compensation of an antalgic gait in an attempt to accommodate the foot into a position that avoids 1st MTP joint dorsiflexion motion during the propulsive phase.7–10 Anyway, foot progression angle has received little attention in the literature and research looking at that parameter has shown a normal range between 5° and 13°.4,11–21 However, values of this angle can be influenced by variability in measurement techniques. A previous study has proved differences in the foot progression angle between pressure platforms and inked footprints.22
With the exposed theoretical assumption that 1st MTP joint dorsiflexion limitation could be associated with a reduction in the internal rotation pattern of the lower extremity, we want to investigate if advanced HL patients have a reduced internal rotation pattern of the lower limb and if this reduction is related to an increase in the foot progression angle during gait. It will be also studied the relationship between rotational patterns of the lower extremity and foot progression angle. Moreover, with the rise of new pressure platform systems for clinical and research purposes, the present study will also try to assess differences in the foot progression angle between pressure platform systems and traditional methods of footprints study (not computer assisted).
Patients and methodsStudy populationThe study population was formed by patients of the University Clinic of Podiatry of Universidad de Sevilla between March 2015 and June 2015 that met the inclusion criteria of the study and from podiatry students of the University of Sevilla that volunteered to participate in the study and also met the inclusion criteria.
Inclusion criteria were a decrease in 1st MTP range of motion equal or less than 35° and people older than 20 in which ossification centers were closed.18 Exclusion criteria were the use of orthotic devices (including insoles) in the lower limb, history of traumatic event or surgery in the first ray or lower limb and inflammatory, metabolic, degenerative or neuromuscular diseases that can affect the foot.
An informed consent was obtained in each participant. This consent was obtained by oral and written explanation with a document containing all the information related to the nature and extend of the study. The study was carried following the Helsinki Declaration of the World Health Organization of 1964.23
Variables measuredThe protocol of data acquisition was as follows: once the informed consent was signed by the participant, a data sheet with personal data was then filled and after that, variables were measured by examination of the same investigator (G.L.S.) thus avoiding intersubject error. First MTP joint range of motion was assessed with the subject lying supine with a two-arm manual goniometer and only people with 35° or less were accepted to participate. The center of the goniometer should be at the center of the head of the first metatarsal. The proximal arm was parallel to the bisection of the diafisis of the first metatarsal and the distal arm was also parallel to the bisection of the proximal phalanx. From neutral position of the joint, a dorsiflexion movement to maximal dorsiflexion of the joint was performed with the distal arm, allowing first metatarsal plantarflexion for normal dorsiflexion of the joint without restrictions3,4 (Fig. 1). Once subjects met the inclusion and exclusion criteria the rest of parameters were then studied in each subject.

The internal and external rotation pattern was measured with the subjects in supine position with the knee extended and the ankle at 90°. One hand of the examiner grasp the heel making maximum internal and external rotation range of motion with the other hand was holding a gravitational goniometer4 (Fig. 2).
 Starting position, b) internal rotation pattern, c) external rotation pattern.")
Hip rotation was measured with the subjects sitting in a table with flexed knees and feet hanging over the examination table. One hand was in the ankle joint making maximum internal and external rotation of the hip and the other hand was holding the gravitational goniometer in the tibia.24–26
Tibial torsion was measured with the subject in prone position and with the knee and ankle flexed 90°. Again, a two-arm manual goniometer was used with one arm in parallel to the tight bisection and the other arm parallel to the external foot border. The center of rotation of the goniometer was located in the center of the heel plantarly.24–26 All measurements were made twice by the same investigator and the mean of the two measurements was used for analysis. The protocol of assessment of the 1st MTP joint range of motion, internal rotation pattern and foot progression angle of the subjects of the study were made exactly in the same manner and by the same investigator that the protocol of assessment published in the doctoral thesis “Patrón Rotador de la Extremidad Inferior. Un Nuevo Parámetro Exploratorio. Relación con el Hallux Limitus”.4 This aspect was made with the intention of using data of a control group of normal subjects derived from the sample of that doctoral thesis for the comparison with the data of the present study.
After those exploratory maneuvers, the foot progression angle was measured in an inked latex carpet. The measurements of the carpet used were: depth 2mm, width 50cm and length 120cm. The carpet was inked in its inferior border over a porous paper tape of 50cm wide and 150cm in length. The subject was standing at the beginning of the carpet and was asked to walk at its self-selected speed in a straightforward direction. Two footprints were obtained in each foot.4
Foot progression angle was also measured in a 42cm×40cm pressure platform (Diagnostic Support®, Italy). Subjects were instructed to walk normally in a straight line over a corridor where the pressure platform was located in the floor. After some test trials the subject should step the pressure platform with one foot first and with the other foot in other different trial. The function of “Ang.plant.longitudinale” was used as foot progression angle provided by the pressure platform in its software program Milletrix 7 (MTX7) (Fig. 3).

A screen capture of the footprints displayed in the pressure platform was also obtained. In the capture, the footprints appeared with the foot progression angle the subject had when stepping on the platform. AutoCAD software was used to measure the foot progression angle in that condition. At the same time, footprints obtained in the paper tape were digitalized with the scanner HP Deskjet F300 and AutoCAD software was also used to measure the foot progression angle.
Statistical analysisData analysis was carried out with the software SPSS Statistics® version 22 (IBM Corp, Armonk, EE. UU.) for Windows®. Because sample size was less than 50, a normality test of the sample was conducted by means of the Shapiro-Will test. In the case of comparison of variables that followed a normal distribution, Student's t test was performed for paired and non-paired samples together with Pearson's correlation. In the case that the variable did not show a normal distribution, non-parametric tests by means of Spearman Rho test was performed. A hypothesis test was performed with a considered significant value of p<0.05.
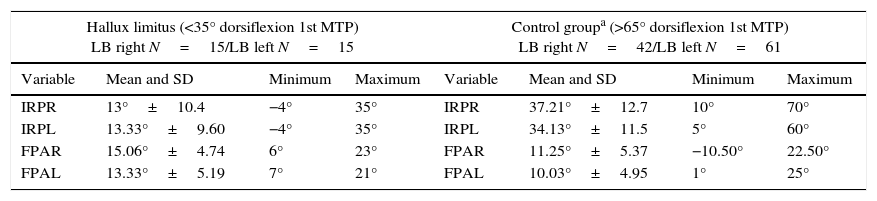
For completion of the first and second objective of the study, mean values of the internal rotation pattern and foot progression angle obtained in the inked latex carpet of the present study were compared with those of the study carried out by Lafuente4 in 2006 in his doctoral thesis as has been noted before. In that way, from the sample of 210 subjects, the subjects with a dorsiflexion range of motion of the 1st MTP joint greater or equal than 65° of dorsiflexion were selected for comparison with the subjects of the present study. That value was chosen because it can serve as a reference value for normal propulsion during gait.3 The sample of the doctoral thesis was composed of 112 men and 98 women with a mean age of 36.48 years (Table 1).
Descriptive parameters for the variables PRI and AM in the HL and control group.
| Hallux limitus (<35° dorsiflexion 1st MTP) LB right N=15/LB left N=15 | Control groupa (>65° dorsiflexion 1st MTP) LB right N=42/LB left N=61 | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Mean and SD | Minimum | Maximum | Variable | Mean and SD | Minimum | Maximum |
| IRPR | 13°±10.4 | −4° | 35° | IRPR | 37.21°±12.7 | 10° | 70° |
| IRPL | 13.33°±9.60 | −4° | 35° | IRPL | 34.13°±11.5 | 5° | 60° |
| FPAR | 15.06°±4.74 | 6° | 23° | FPAR | 11.25°±5.37 | −10.50° | 22.50° |
| FPAL | 13.33°±5.19 | 7° | 21° | FPAL | 10.03°±4.95 | 1° | 25° |
LB: lower limb; SD: standard deviation; IRPR: internal rotation pattern right; IRPL: internal rotation pattern left; FPAR: foot progression angle right; FPAL: foot progression angle left; N: sample size.
Control groups obtained from the Doctoral Thesis “Patrón Rotador de la Extremidad Inferior. Un Nuevo Parámetro Exploratorio. Relación con el Hallux Limitus”.4
The sample size of this study was composed by 30 feet in 15 subjects with a decrease in the range of motion of the 1st MTP joint (13 men and 2 women). Mean age was 37.86±19.03 years with a range of 22–73 years.
A significance test by means of Student's t-test was performed by comparing internal rotation pattern and foot progression angle in subjects with HL and subjects with normal range of motion of the 1st MTP joint (Table 2). Results allow rejection of the null hypothesis showing that individuals with advanced HL present more limitation of the internal rotation pattern and an increase in the foot progression angle compared with normal subjects.
Parametric testing.
| Variable | Mean and SD in HL group | Mean and SD in control groupa | Significance (p) | 95% interval confidence | |
|---|---|---|---|---|---|
| Inferior | Superior | ||||
| IRPR | 13°±10.4 | 37.21°±12.7 | <0.001 | −29.9879 | −18.4321 |
| IRPL | 13.33°±9.60 | 34.13°±11.5 | <0.001 | −26.1152 | −15.4781 |
| FPAR | 15.06°±4.74 | 11.25°±5.37 | 0.008 | 1.1901 | 6.4432 |
| FPAL | 13.33°±5.19 | 10.03°±4.95 | 0.027 | 0.4283 | 6.1783 |
SD: standard deviation; IRPR: internal rotation pattern right; IRPL: internal rotation pattern left; FPAR: foot progression angle right; FPAL: foot progression angle left.
Student's t-test.
Control groups obtained from the Doctoral Thesis “Patrón Rotador de la Extremidad Inferior. Un Nuevo Parámetro Exploratorio. Relación con el Hallux Limitus”.4
At the same time, the mean values of the foot progression angle measured in the inked latex carpet were compared with the internal and external rotation pattern angle, hip internal and external rotation angle and tibial torsion. It was intended to establish the relationship between foot progression angle and those static measurements. Pearson's correlation was applied as those variable presented normal distribution. Results showed a weak positive correlation between foot progression angle with the external rotation pattern and the hip external rotation (r=0.297 and 0.073 respectively). However, the foot progression angle also showed a moderate positive correlation with tibial torsion (r=0.472; p<0.01), moderate negative correlation with hip internal rotation (r=−0.399; p<0.05) and good negative correlation between foot progression angle and the internal rotation pattern (r=−0.563; p<0.01).
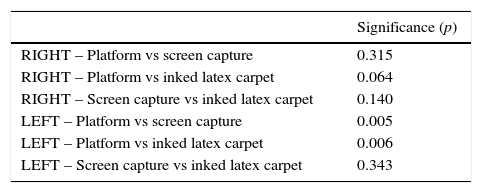
Finally, mean values of the foot progression angle obtained in the three methods studied, (inked latex carpet, platform and screen capture of the platform) were compared. A paired t-test was performed for each of the six paired comparisons (three for right foot and three for the left foot) (Table 3). Results showed statistically significant differences for the left foot between platform and screen capture and platform and inked latex carpet (p<0.05). However, the right foot had a p value of 0.064 for the comparison of platform and inked latex carpet that was closer to the established significance level.
Parametric test – foot progression angle.
| Significance (p) | |
|---|---|
| RIGHT – Platform vs screen capture | 0.315 |
| RIGHT – Platform vs inked latex carpet | 0.064 |
| RIGHT – Screen capture vs inked latex carpet | 0.140 |
| LEFT – Platform vs screen capture | 0.005 |
| LEFT – Platform vs inked latex carpet | 0.006 |
| LEFT – Screen capture vs inked latex carpet | 0.343 |
Student's t-test for paired samples.
The results of the present study have shown that subjects with advanced HL (less or equal than 35° for 1st MTP joint dorsiflexion) have a limitation of the internal rotation pattern compared with subjects with a normal extension of the first MTP joint (≥65°) (p<0.001 in both limbs). Lafuente et al.5 in 2011 performed a study that compared this aspect between a control group with more than 65° of dorsiflexion of the 1st MTP joint and a group of subjects with medium and moderate HL (35–55° range of motion). They evaluated a total of 80 subjects pointing out that the internal rotation of the lower limb was smaller in HL subjects with an internal rotation pattern of 23.22° in the HL group compared to 38.19° in the control group. Correlation of these variables were also significant in both limbs (r=0.638, p<0.0001).5 Comparing that data with the results of the present study, it can be observed that the internal rotation pattern of the subjects in the present study is smaller compared to normal values and subjects with medium HL deformity. At the same time, it can be observed that in general, subjects with fewer degrees of internal rotation pattern had less extension of the 1st MTP joint.
The finding that medium and advanced HL patients have less internal rotation range in the lower limb during static examination, allows us to propose that the inability of placing the foot straight regarding the medium axis of the body could be related with some of the etiologic factors of the HL deformity. At the beginning of the stance phase the lower limb is rotating internally which allows the whole plantar foot, including 1st MTP joint, to make contact with the ground adapting to surface irregularities. A limitation of the movement of internal rotation of the lower limb could make the 1st MTP joint to work as a dorsiflexed first ray making the proximal phalanx to plantarflex to maintain contact of the foot with the ground medially and distally in the medial column. This can create a retrograde force that increases the first ray elevation. It must be remembered that dorsiflexion of the first ray, plantarflexion of the proximal phalanx and dorsiflexion of the distal phalanx are main structural characteristics of HL.5 In the present study it has been showed that subjects with advanced HL (≤35° of 1st MTP joint dorsiflexion) have an increase of the foot progression angle compared to subjects without HL (p=0.008 for right foot and p=0.027 for left foot).
Lafuente et al.5 compared the foot progression angle between a control group (with more than 65° of dorsiflexion of the 1st MTP joint) and a group of patients with medium HL (53–55°). The results showed that foot progression angle was bigger in subjects with medium HL (11.91°) compared to control group (10.66°), although this result was not statistically significant (p=0.115). By comparing those results with the results of the present study, it seems that the foot progression angle increases with limitation of the 1st MTP joint dorsiflexion (15.06° for right foot and 13.33° for left foot). It is the opinion of the authors that the absence of differences in the study of Lafuente et al.5 could be explained because the patient group had mild HL deformity and that result probably would have changed with advanced HL patients as in the present study has occurred (p=0.008 for right foot and p=0.27 for left foot). From these results it can mean that foot progression angle increases with an increase in 1st MTP joint limitation into dorsiflexion.
The increase in the foot progression angle seen in patients with advanced HL can be produced by a limitation of the internal rotation pattern of the lower limb or, conversely, it can be viewed as a consequence of the restriction of motion in that joint in an attempt to avoid pain during midstance and propulsion. The inability to dorsiflex the joint adequately during gait can be compensated with forefoot supination, decrease in arch height and absence of propulsion because of lack of subtalar joint supination during propulsion.5,8
Finally, the foot progression angle was analyzed with three different methods to observe differences between them. The three methods were, firstly the value provided by the platform, secondly the measure of the screen capture of the footprints given by the platform and finally the footprints of the inked latex carpet. In first place, it was observed that the results showed bigger values for the right foot compared with the left foot in the foot progression angle. Curiously, this results are in accordance with several authors that compare this angle between limbs.4,12,18,21,27 Some studies included a sample with children, young and adult participants12,18,27 and it can be thought that the foot progression angle increases with age as children and young patients had reduced values of the foot progression angle compared with adults.
The values of the foot progression angle measured with the three methods showed statistically significant differences between the platform and the screen capture of the platform in the left foot (p=0.005) and between the platform and the inked latex carpet (p=0.006). However, the right foot obtained a p value of 0.06 for the comparison of the platform with the inked latex carpet. Although this result did not reach statistical significance, it was very close and we think that the result would have been positive with an increased sample size.
The introduction of new pressure platform systems for clinical examinations supposes new methods for the study of the foot progression angle. This kind of systems seems to give an easier way of calculating that angle. However, it was not possible to discover the reference points used by the system for the calculation of the foot progression angle. Manufacturer was unable to provide that information. For that reason, in the present study we compared the value of the foot progression angle provided by the platform with other two methods. From the results of the study it does not seems possible to use the values provided by the platform certainly in the clinical and research environment because those values showed differences with the other two methods of measurement used.
Regarding the limitations of the study, we consider the fact that the foot progression angle was taken only from the measurement of one single footprint in each foot for each method of study as a main drawback, as foot progression angle can vary dynamically from one step to other.22
In the future it would be interesting to equilibrate the sample size regarding sex variable as this could influence the results obtained. At the same time, it would be interesting to increase sample size including several ranges of age in the sample. As it has been noted, studies have shown a tendency to increase foot progression angle with age.4,12,18,21,27 Another future investigation would include equality of right and left handed subjects in the sample. In the present investigation foot progression angle was bigger in the right foot compared to the left and except one, all subject were right handed. This point is important as could relate some kind of relationship between cerebral dominance and foot progression angle. Moreover, we would consider of interest looking at other factors that could have some influence in the foot progression angle such as the pelvis position in stance28,29 that has not been considered in this study.
In conclusion, the present study has shown that subjects with advanced HL have a decrease in the internal rotation pattern and an increase in the foot progression angle compared to normal population, being these results statistically significant. The decrease in the internal rotation pattern resolves an increase in the foot progression angle. The values for the foot progression angle provided by the platform used in this study are not the same as that of the values obtained with a screen capture of the platform and with the inked latex carpet.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that no patient data appears in this article.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.
Conflict of interestsThe authors declare no conflict of interest.
This study has previously been presented as a master's thesis in the Master's New Trends in Health Sciences at the Universidad de Sevilla in November 2015.