



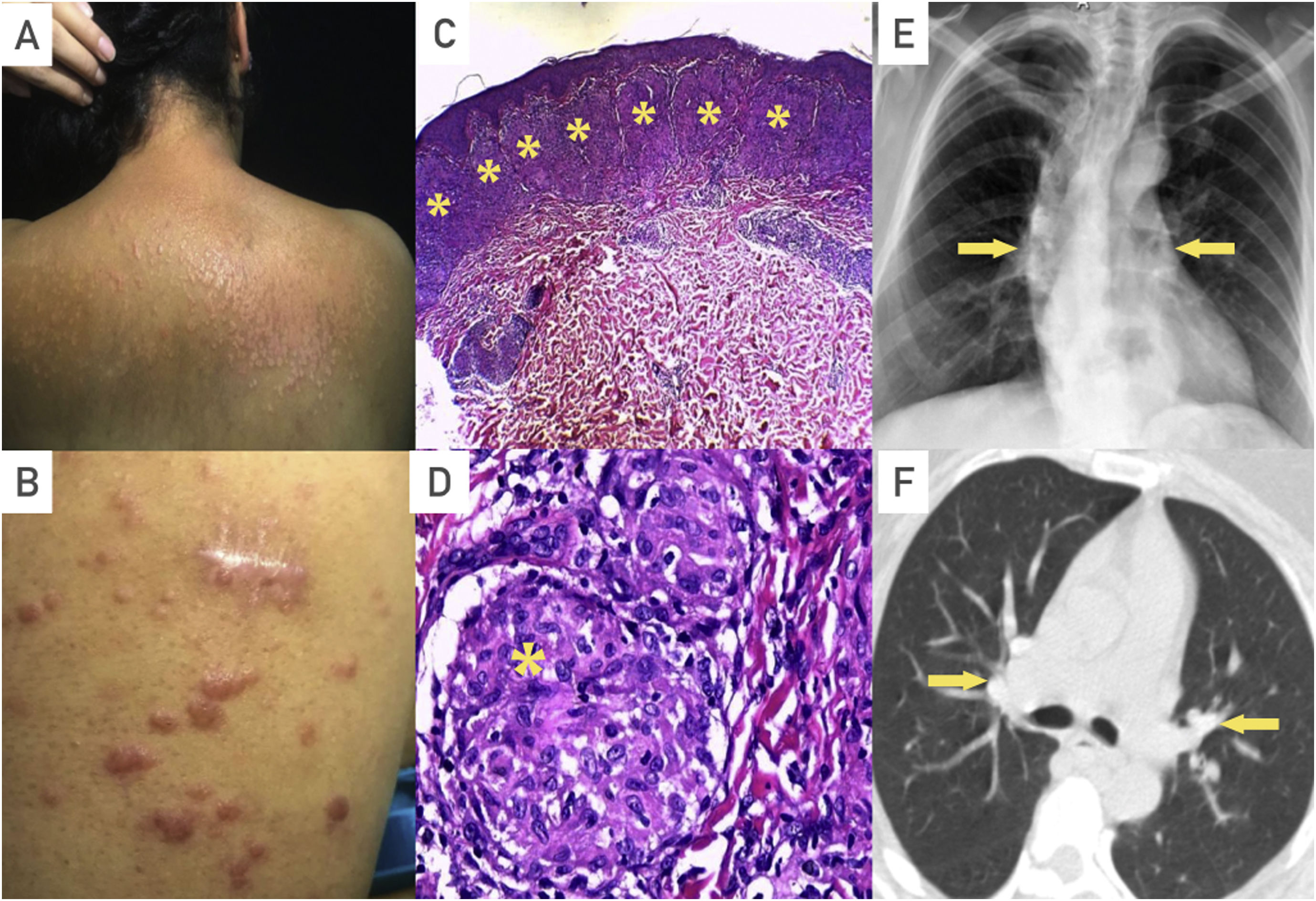
A 43-year-old previously healthy woman began with new-onset skin lesions, characterized by papules, nodules, and plaques (Fig. 1A, B). Biopsies of the lesions were performed identifying non-caseating granulomas (Fig. 1C, D), infectious diseases, malignancy and additional systemic involvement were ruled out; The patient was scheduled every six months for outpatient assessment but was lost to follow-up, and two years later, she presented to our hospital with new-onset dyspnea. Imaging studies showed bilateral hilar lymphadenopathy (Fig. 1E, F) and a mild restrictive pattern in pulmonary function test, fulfilling criteria for diagnosing sarcoidosis with systemic involvement.

Sarcoidosis is a heterogeneous systemic disease characterized by non-caseating granulomas in any organ. Therefore, it must be approached as a diagnosis of exclusion since it must be distinguished from many conditions associated with similar findings including tuberculosis, fungal infections, berylliosis, lymphoma, Crohn's disease, among others.
The skin affection ranges from 16 to 32%. This affection as the only involvement organ can result in a challenging diagnosis, mainly when the lesions are not the classic sarcoidosis lesions as erythema nodosum or lupus pernio.
Periodic monitoring with a multidisciplinary team approach can detect other system involvement and carry out an early intervention that leads to better outcomes.
Authors’ contributionsAll authors have contributed equally.
Availability of data and materialThe data that support the findings of this study are available from the corresponding author, upon reasonable request.
FundingNone reported.
Conflicts of interestNone reported.
