


Heroin and its contaminants may be an important source of allergens in young people. We present a case of severe endophthalmitis in a patient that also suffered from anaphylactoid symptoms (hypotension, urticaria, glottic oedema) whenever he ingested lemon.
MethodsPrick tests with a battery of 42 aeroallergens including fruits and citrus fruits (orange, mandarin, grapefruit and lemon) and specific IgE to these allergens were carried out. Immunodetection was performed using the patient's serum and the following allergens: lemon, Candida, Aspergillus, Penicillium and Alternaria recombinant Alt 1 (Laboratories Diater).
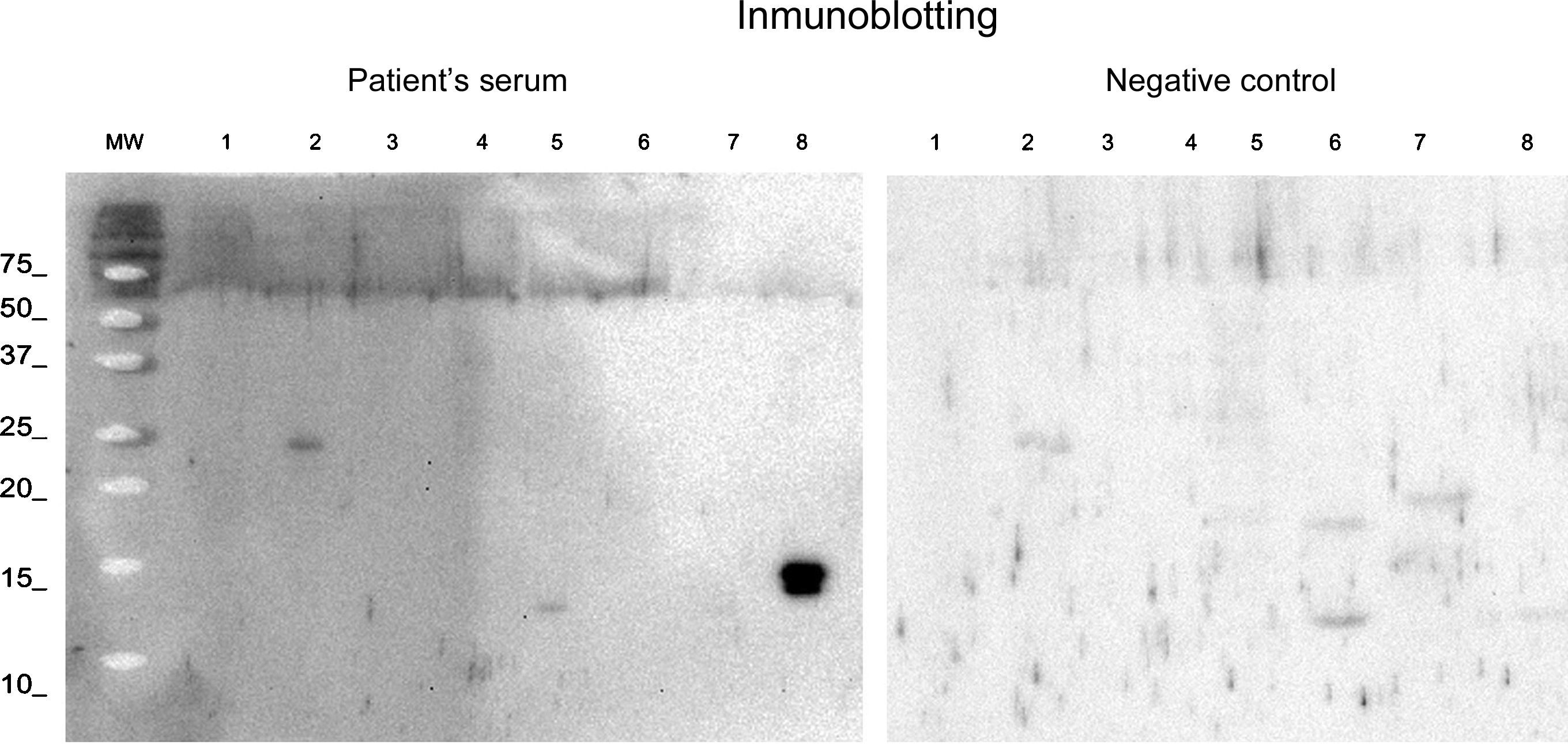
ResultsSkin tests were negative for Candida, Penicillium, Aspergillus and Cladosporium (ALK-Spain) as were specific IgE antibodies for CAP (Thermofisher, Sweden) and positive only for lemon and, doubtfully, to Candida. Specific IgE tests to pollen, arthropods, fungi, dander and foods were positive only for lemon (0.49kU/L). Serological study of fungi ruled out fungal infection at that time. The immunodetection showed that the patient's serum recognised a protein of approximately 25kDa of lemon peel, one of approximately 12–13kDa of Penicillium, and perfectly recognised Alt a 1.
ConclusionsLemon surface can be contaminated by Candida and other fungi. In heroin addicts with positive skin tests for lemon, the possibility of these serious complications should be taken into account.
Lemon hypersensitivity is rare, but has been associated with hypersensitivity to pollens, wheat and other fruits.1 Lemon is used as a solvent for intravenous heroin use.2,3 We report the case of a heroin addict with AIDS admitted due to a significant reduction in concentric vision. Hypersensitivity tests were instrumental in diagnosing the aetiology of the visual loss.
A 35-year-old male with a history of HIV and drug dependence, and treatment with ETR+DRV/r.RTG from May 2012 until the present.
He was admitted in July 2014 due to bouts of tachycardia with wide QR coinciding with a seizure. He was discharged with a diagnosis of eosinophilic esophagitis grade III, and symptomatic treatment of esophagitis has begun with pump inhibitors.
Structural cardiac or neurological disease was ruled out. The patient reported a doubtful history of hypersensitivity to morphine and penicillin.
The patient attended the emergency room in August 2014 complaining of visual disturbances (seeing wavy images) and occipital headache. Seizures were ruled out, the symptoms were considered secondary to heroin ingestion, and the patient was discharged. Two months later, the patient was referred by his primary care physician to the ophthalmology department due to significant visual loss. Ophthalmologic tests suggested the lesions were due to endophthalmitis, but no microbiological study of the vitreous humour was made, as it was considered that the infection had resolved and therefore the aetiological agent was unknown.
A month later, tests were requested from the allergy unit due to a doubtful hypersensitivity to beta-lactams, which was ruled out by the usual in vivo and in vitro techniques (skin, specific IgE and negative provocations). In this time we do not suspected other drug sensitisation and basal tryptase was not measured. However, the patient reported choking and, sometimes, anaphylactoid symptoms (hypotension, urticaria, glottic oedema) whenever he ingested lemon.
Allergic tests to a battery of 42 aeroallergens including fruits and citrus fruits (orange, mandarin, grapefruit and lemon) were positive only for lemon (5mm×8mm) and Candida (3mm×3mm). Histamine control revealed a wheal of 5mm×5mm. Specific IgE tests to pollen, arthropods, fungi, dander and foods were positive only for lemon (0.49kU/L). A provocation test with lemon was refused for the patient.
Given the possibility that the patient had injected lemon juice contaminated by fungi (as he reported occasionally using lemons in a poor state), and that the visual deficit was due to endophthalmitis due to Candida, a serological study of fungi was made which ruled out fungal infection at that time. Skin tests were negative for Candida, Penicillium, Aspergillus and Cladosporium (ALK-Spain) as were specific IgE antibodies for CAP (Thermofisher, Sweden). Immunodetection was performed using the patient's serum and the following allergens: lemon, Candida, Aspergillus, Penicillium and Alternaria recombinant Alt 1 (Laboratories Diater). The results (Fig. 1) showed that the patient's serum recognised a protein of approximately 25kDa of lemon peel, one of approximately 12–13kDa of Penicillium, and perfectly recognised Alt a 1. After demonstration of the response to fungi, a shock dose of intravenous amphotericin B (Fungizone®) which acts against Cryptococcus, Alternaria and Aspergillus, was administered. Currently, the patient remains on maintenance treatment with Fluconazol (Diflucan®) 200mg/day, with improvement in vision being observed. The positive response positive response to Fluconazol might lead one to think that there was a role played by fungal agents.

Lemon juice is used to dissolve heroin in Spain and has been found in studies in 104 opioid addicts in London.2,3 Heroin is smoked, inhaled or injected subcutaneously either intravenously or intramuscularly. Parenteral administration was most commonly used until the discovery of AIDS; heroin is dissolved in water heated in a spoon and, after adding a few drops of lemon juice or vinegar, is introduced into the syringe and injected. It may reach the brain in 15–30s. Currently, smoking or snorting is more common, with the heroin being heated in foil and the vapours inhaled through a tube.
Oshikata et al. recently reported the first reported fatal case of pneumonia caused by Penicillium digitatum, an environmental fungus considered pathogenic for plants, specifically for poorly-stored citrus fruits, but not for humans.4
Since 1984, various studies have described the possibility of candidiasis in heroin addicts.5–8 In 1984 and 1989 endophthalmitis due to Candida was described in drug addicts and was associated with contamination of lemons used to dissolve heroin by this fungus.8,9
In the case presented here, positive tests for lemon allergy led to the search for Candida infection as the cause of endophthalmitis and the diagnosis of eosinophilic oesophagitis due to citrus fruit with seizures associated with anaphylaxis due to lemon. In heroin addicts with positive skin tests for lemon, the possibility of these serious complications should be taken into account.
Ethical disclosuresProtection of human subjects and animals in researchThe authors declare that the procedures followed were in accordance with the regulations of the responsible Clinical Research Ethics Committee and in accordance with those of the World Medical Association and the Helsinki Declaration.
Confidentiality of dataThe authors declare that they have followed the protocols of their work centre on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to privacy and informed consentThe authors have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence is in possession of this document.
FundingNone.
Author contributionI declare that all the authors, Alicia Armentia, Blanca Martín, Carmen Ramos, F.J. Martin-Gil, Fernando Pineda and Ricardo Palacios, have participated in the conception, design of the study, analysis and interpretation of the data. Alicia Armentia performed a careful clinical work-up, and a reminder about a rare allergy and an unusual risk factor. Blanca Martin performed IgE and other analysis, F.J. Martín-Gil and Carmen Ramos have contributed in the generation, analysis and interpretation of data with the rest of the authors. Fernando Pineda and Ricardo Palacios carried out the immunodetection and IgE-western blot. All authors have participated in the preparation and critical revision of the letter and all authors have seen and approved the final version of the manuscript. I also declare that all the authors have no conflict of interest in connection with this paper, other than any noted in the covering letter to the Editor.
Conflict of interestThe authors report no conflict of interest.
