




Abstracts Asociación Mexicana del Hígado (AMH) 2023
More infoHepatocellular carcinoma (HCC) represents 80-85% of primary liver malignancies, ranks fifth in annual incidence of cancer, with an annual risk in patients with cirrhosis due to hepatitis B virus (HBV) of 3-8%. It has a tendency to involve vascular structures in the liver, such as the portal vein (VP) and hepatic veins (VH). Although HCC involvement of VH is seen less frequently compared to PV, tumor thrombi (TT) have been found to extend into the inferior vena cava (IVC) and right atrium (RA) through the HV. In patients with cardiac metastasis, secondary Budd-Chiari, pulmonary infarction and/or pulmonary metastasis have been documented mainly. A certain number of patients with TT-VH may develop Budd Chiari syndrome <3%, associated with chronic HBV infection.
Materials and PatientsA 58-year-old male patient with a history of human immunodeficiency virus and HBV coinfection, E antigen negative, with virological response. He presented with intense abdominal pain in the left hypochondrium that radiated in a generalized way to the inguinal region bilaterally. During the evaluation, ultrasonographic data of cirrhosis, ascites, Budd-Chiari syndrome, extensive portal thrombosis and hepatocellular carcinoma are found.
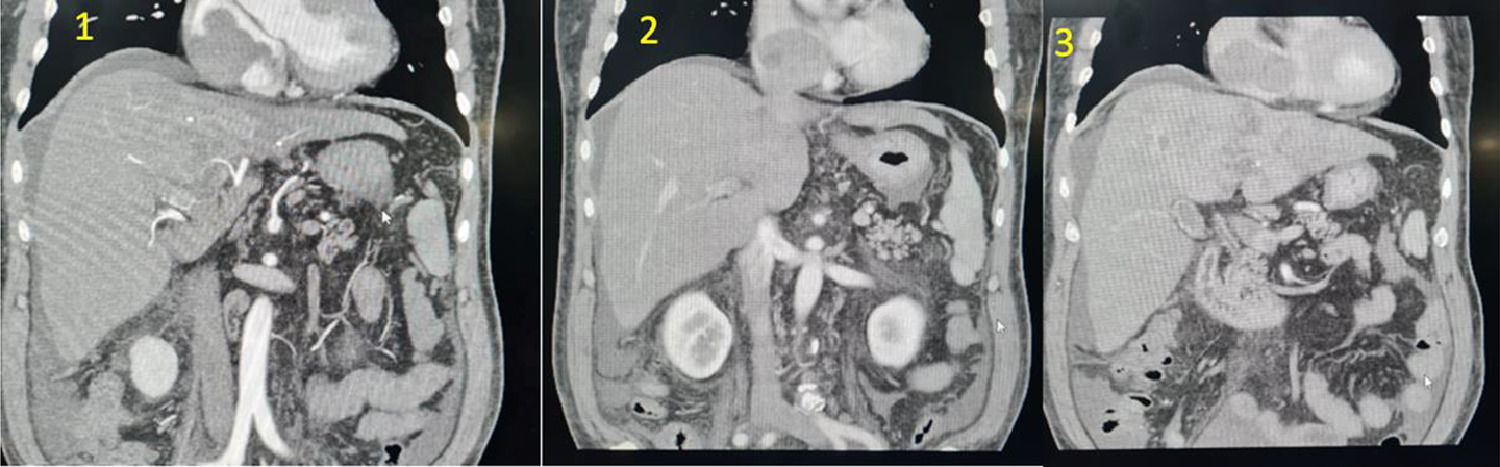
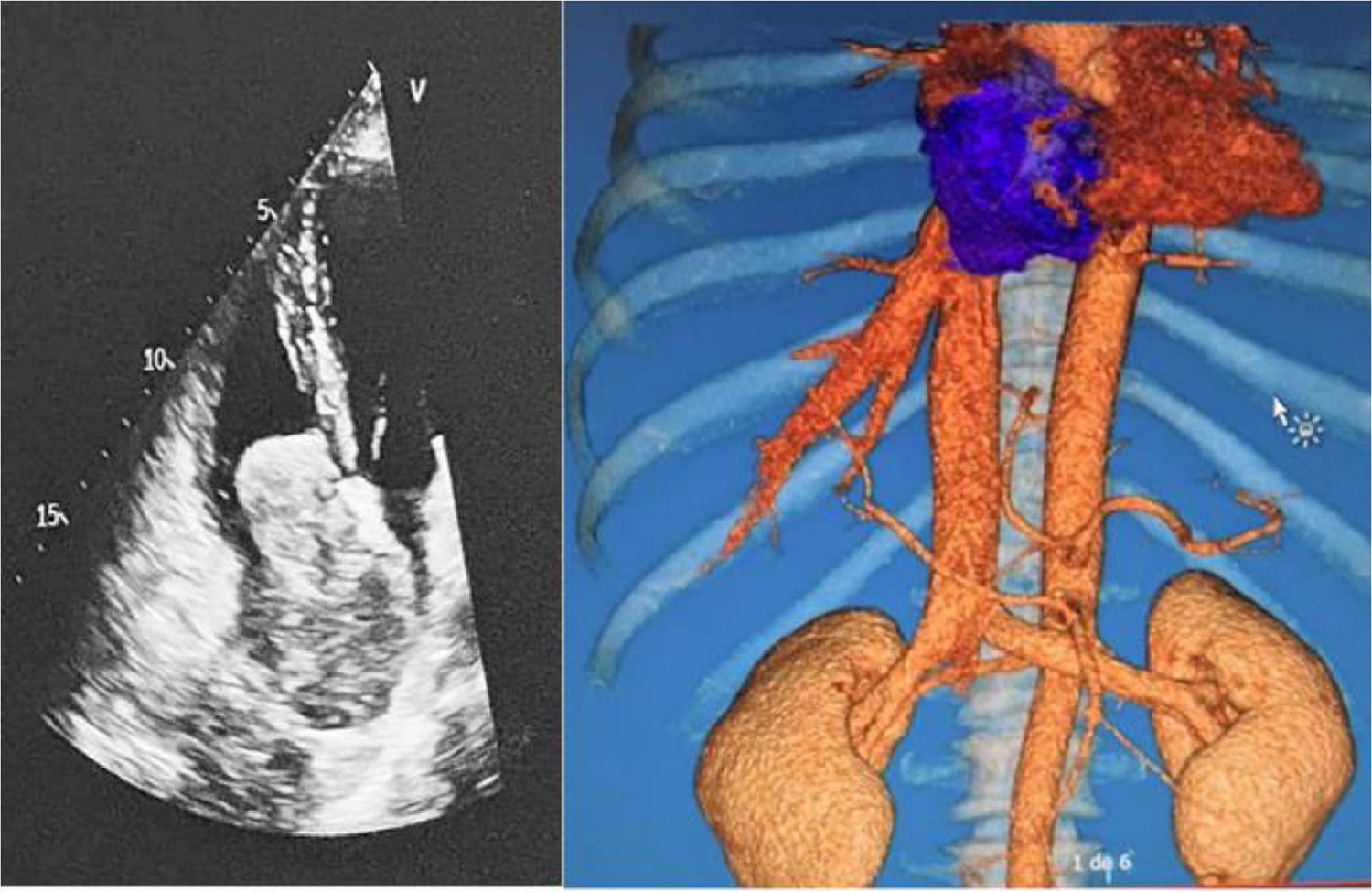
ResultsAngiotomography showing areas of ischemia and necrosis in the left hepatic lobe, with the presence of a heterogeneous lesion measuring 5.2 cm that involves segments II, III, IVA, and IVB with enhancement in the arterial phase, portal vein thrombosis, and middle suprahepatic veins. Left, as well as a cardiac tumor dependent on the right atrium with extension to the ipsilateral ventricle and inferior vena cava. A transthoracic echocardiogram shows the involvement of the right heart cavities. Laboratory findings: Valued for oncology services without being a candidate for any therapy.
ConclusionsWe present a case with symptoms compatible with acute Budd Chiari syndrome with extension to the right atrium and right ventricle secondary to hepatocellular carcinoma. Due to the extension of the tumor, it was not a candidate for surgical therapy, thrombolysis or systemic therapy, presenting with a torpid evolution. Metastasis to the inferior vena cava and right atrium secondary to HCC are uncommon. Imaging studies play an important role in determining the type of lesion and its extension. There are few investigations on treatment since high mortality rates are reported with the performance of lumpectomy combined with thrombectomy. Gaining relevance in the search for therapeutics mainly in tertiary level hospitals and in the scrutiny to rule out HCC and HBV infection in a timely manner.
Ethical statement
The identity of the patients is protected. Consentment was obtained.
Declaration of interests
None
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.

Figure 1: Triphasic computed tomography. 1) Arterial phase: arterial enhancement stronger than the surrounding liver (wash-in). 2) Venous phase: hypodensity or hyposignal intensity compared to the surrounding liver (wash-out) in the venous phase.

Figure 2: Comparison between echocardiography and tomographic reconstruction



