

This study shows the psychometric characteristics and factor structure of the Spanish adaptation to a clinical population of an instrument for measuring anxious worry, the Anxious Thought Inventory (AnTI).
MethodParticipants were 731 adults treated at a community mental Health Center in Spain with different clinical diagnoses.
ResultsThe adaptation of the AnTI scale to the Spanish clinical population confirms the three original dimensions, social worry, health worry and meta-worry, with adequate fit. High internal consistency (from .83 to .86) was found for the three subscales, and test–retest reliability after a period of 8–10 weeks was high (r=.71). Furthermore, significant correlations were found with other worry, anxiety and general psychopathology scales.
ConclusionsThis Spanish adaptation of the AnTI in a clinical population is a reliable, valid measure of anxious worry. Therefore, it is a useful instrument for use in care contexts.
El presente estudio muestra las características psicométricas y estructura factorial de la adaptación española en población clínica de un instrumento de medida de las preocupaciones ansiosas: el Anxious Thought Inventory (AnTI).
MétodoLos participantes fueron 731 adultos tratados en un centro de salud mental comunitario español, con diferentes diagnósticos clínicos.
ResultadosSe confirman las tres dimensiones originales, preocupación social, preocupación por la salud y meta-preocupación con un adecuado ajuste. Se obtuvo una alta consistencia interna (.83-.86) para las tres subescalas, y la fiabilidad test–retest tras un período de 8-10 semanas fue alta (r=.71). Por otra parte, se obtuvieron correlaciones significativas con otras medidas de preocupación, de ansiedad, así como de psicopatología general.
ConclusionesLa presente adaptación española del AnTI en población clínica es una medida fiable y válida de las preocupaciones ansiosas. Por ello se trata de un instrumento de utilidad para su uso en distintos contextos asistenciales.
The concept of worry has had a long history in the field of anxiety disorders, although it has developed considerably since the eighties. During this period, the DSM III-R (APA, 1987) also included excessive or pathological worry as a core element of Generalized Anxiety Disorder (GAD), with growing recognition of its importance in GAD in the following editions of the DSM. The high prevalence of GAD in the population (OMS, 2016), its association with healthcare service use frequency (Wittchen, 2002) and its notable cost to society (Chisholm et al., 2016) confer these psychological disorders enormous importance.
Furthermore, worry is shown to be a common element in many disorders, especially anxiety and depressive disorders (Barlow, 1988; Startup et al., 2016). Some studies have even suggested that, more than part of the phenomenology of anxiety, worry could be a causal factor of it with an activation and maintenance role (Bailey & Wells, 2016).
Worry may be defined as a pattern characterized by the presence of repetitive intrusive and negative thoughts about future events and constitutes a cognitive component of anxiety, clearly differentiated from the somatic activation component (Borkovec, 1985). An essential aspect of pathological worry is its uncontrollable nature. This perception of uncontrollability is closely related to metacognition, a term which refers the cognitive factors which are involved in evaluation and control of thought and which has been shown to be a central construct in the appearance and maintenance of several psychological disorders (Gkika, Wittkowski, & Wells, 2018).
The metacognitive model developed by Wells (1997) distinguishes two subtypes of worry: Type 1: worry about external events and physical symptoms, and Type 2, related to negative beliefs about worries. Some of these beliefs, especially those related to thoughts as uncontrollable and dangerous, are considered a transdiagnostic factor contributing to distress and leading to a specific pattern of response to inner experiences which has been called cognitive-attentional syndrome (Wells, 2009). Although there are few studies on the incidence of each of these beliefs in the results of psychological treatments, some studies have shown that metacognitive beliefs may be a predictor of the results of psychological treatment (Nordahl, Nordahl, Hjemdal, & Wells, 2017). Hence, based on this model, treatments should focus on modifying metacognitive factors, including negative beliefs about worry itself.
The involvement of worry in anxiety and depressive disorders and the importance of these disorders, confer special interest to its study, which requires appropriate instruments for its assessment. Some instruments developed for clinical assessment of worry have focused on the propensity to worry (Meyer, Miller, Metzger, & Borkovec, 1990), understood as a trait, and in the discrimination between anxious and depressive preoccupation (Beck, Brown, Steer, Eidelson, & Riskind, 1987). However, there are few instruments directed at assessing contents and measuring processes involved in anxious worry. And even fewer are available for the Spanish population. The Metacognition Questionnaire 30 is directed at evaluating beliefs about worry and intrusive thoughts, as well as metacognitive monitoring (Ramos-Cejudo, Cano-Vindel & Salguero, 2013; Wells & Cartwright-Hatton, 2004) and the Thought Control Questionnaire evaluates the tendency to use metacognitive strategies to control intrusive thoughts (Cano, 2007; Wells & Davies, 1994).
The Anxious Thoughts Inventory (AnTI; Wells, 1994) is one of the instruments most recognized for assessment of worry. Unlike the other instruments developed for measuring worry, such as the Penn State Worry Questionnaire (Meyer et al., 1990; Sandín, Chorot, Valiente, & Lostao, 2009), which assesses the frequency of worry, the AnTI focuses on analyzing worry content. It is a multidimensional measure which assesses different types of worries and makes an important differentiation between worry (Type 1) and meta-worry (Type 2). In the first case, Type 1, worry refers to physical, social or environmental events, differentiating a first subscale of social worry from a second one on health worry. In the second case, Type 2, worry deals with the act of worrying itself and with cognitive functioning.
Assessment of each of these types of worry is of interest insofar as it can provide information relevant to understanding the processes involved in vulnerability to and evolution of anxiety and depressive disorders in which worry may have an important role. It is therefore of great interest to have validated instruments which are able to evaluate each of these types of worry.
The original English scale shows very satisfactory reliability and validity psychometric properties. The instrument's three subscales have also been shown to be sensitive to therapeutic intervention, obtaining significant differences in pre-post treatment measurements (Shahbarizad, Ghadampour, Ghazanfari, & Momeni, 2017). These results make the AnTI an important instrument in clinical practice for the detection and measurement of worry associated with the development and maintenance of anxiety and depressive disorders. Other studies have confirmed its adequate psychometric characteristics in an Iranian (Fata, Moutabi, Moloudi, & Ziayee, 2010) and Brazilian population (Moreno, Gomes, De Souza, & Gauer, 2014), in both cases with samples of undergraduates. Both studies confirmed the three-factor structure and high internal consistency, as well as significant positive correlations with measures of anxiety, depression, and in the Brazilian study, with other worry assessment instruments.
However, there is still no adaptation of the scale to the Spanish clinical population, except partial preliminary data (Vázquez Morejón, Jiménez Gª-Bóveda, & Vázquez-Morejón, 2007). Therefore, this study poses as its objective, the adaptation of the AnTI to the Spanish population for clinical use.
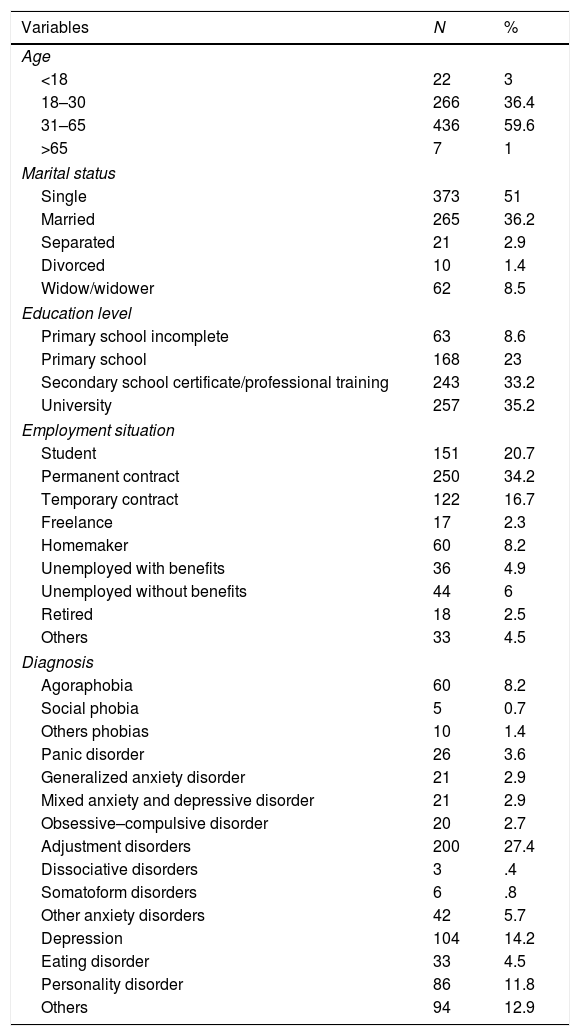
MethodParticipantsThe sample consisted of 731 patients treated in a Community Mental Health Unit. It included 470 women (64.3%) and 261 men (35.7%) with a mean age of 36.47 years (SD=13.04, range=15–84). Other sociodemographic and clinical data appear in Table 1.
Sociodemographic information (N=731).
| Variables | N | % |
|---|---|---|
| Age | ||
| <18 | 22 | 3 |
| 18–30 | 266 | 36.4 |
| 31–65 | 436 | 59.6 |
| >65 | 7 | 1 |
| Marital status | ||
| Single | 373 | 51 |
| Married | 265 | 36.2 |
| Separated | 21 | 2.9 |
| Divorced | 10 | 1.4 |
| Widow/widower | 62 | 8.5 |
| Education level | ||
| Primary school incomplete | 63 | 8.6 |
| Primary school | 168 | 23 |
| Secondary school certificate/professional training | 243 | 33.2 |
| University | 257 | 35.2 |
| Employment situation | ||
| Student | 151 | 20.7 |
| Permanent contract | 250 | 34.2 |
| Temporary contract | 122 | 16.7 |
| Freelance | 17 | 2.3 |
| Homemaker | 60 | 8.2 |
| Unemployed with benefits | 36 | 4.9 |
| Unemployed without benefits | 44 | 6 |
| Retired | 18 | 2.5 |
| Others | 33 | 4.5 |
| Diagnosis | ||
| Agoraphobia | 60 | 8.2 |
| Social phobia | 5 | 0.7 |
| Others phobias | 10 | 1.4 |
| Panic disorder | 26 | 3.6 |
| Generalized anxiety disorder | 21 | 2.9 |
| Mixed anxiety and depressive disorder | 21 | 2.9 |
| Obsessive–compulsive disorder | 20 | 2.7 |
| Adjustment disorders | 200 | 27.4 |
| Dissociative disorders | 3 | .4 |
| Somatoform disorders | 6 | .8 |
| Other anxiety disorders | 42 | 5.7 |
| Depression | 104 | 14.2 |
| Eating disorder | 33 | 4.5 |
| Personality disorder | 86 | 11.8 |
| Others | 94 | 12.9 |
Anxious Thoughts Inventory (Wells, 1994). This is a self-report questionnaire with 22 items scored on a four-point Likert-type scale (1=“almost never” to 4=“almost always”). It has three factors: social worry, health worry and meta-worry. The original English version showed good reliability, with a Cronbach's alpha of .84 for social worry, .81 for health worry and .76 for meta-worry. The AnTI correlates positively with other worry scales, such as the Penn State Worry Questionnaire (Wells & Papageorgiou, 1998), with correlations of .58 with social worry and .40 with health worry. It also shows discriminant validity between different diagnostic groups, as well as between clinical and nonclinical patients (Wells, 1994).
Beck Anxiety Inventory (BAI; Beck, Epstein, Brown, & Steer, 1988). This scale has 21 items scored on a four-point Likert-type scale (0=“not at all” to 3=“severely”) for assessing the main symptoms of anxiety experienced during the previous week. The data available on the characteristics of the Spanish population sample show high internal consistency, with a Cronbach's alpha of .91 and satisfactory test–retest reliability (r=.84). They also show adequate convergent validity with other anxiety measures such as the SCL-90-R anxiety dimension (r=.86) (Sanz, 2011; Vázquez Morejón, Vázquez-Morejón, & Bellido Zanin, 2014).
Symptom Checklist 90-R (SCL-90-R; Derogatis, 1977). This is a self-report scale comprised of 90 items collecting information on a wide variety of psychopathological manifestations. The items are scored on a five-point Likert scale (0=“not at all” to 4=“much or extremely”). The Spanish adaptation used in this study (González de Rivera, de las Cuevas, Rodríguez Abuín, & Rodríguez Pulido, 2002) shows high internal consistency, with a Cronbach's alpha of .94 for the 90 items included in the test.
Penn State Worry Questionnaire (PSWQ; Meyer et al., 1990). This is an inventory which assesses the general tendency to worry or trait-worry. It is comprised of 16 items scored on a five-point Likert scale (1=“not at all” to 5=“severe”). In the Spanish version used here (Nuevo, Montorio, & Ruiz, 2002), which shows adequate psychometric characteristics, the five reverse-scored items in the original English version were inverted, because according to the authors, the results of a pilot study had shown problems in understanding these items. This adaptation has a Cronbach's alpha of .95 and validity is highly correlated (r=. 76) with the STAI-R trait anxiety inventory.
ProcedureFirst, after acquiring authorization from the author of the AnTI for its adaptation, the items were translated using the back translation method.1
After a first pilot test with 10 subjects to check their understanding and the adequacy of the scale, it was applied along with other instruments commonly used for assessing patients referred to the Community Mental Health Unit. In all cases, informed consent was requested after explaining the purpose of the study, as well as the voluntary nature of participation. In the 25 first cases, the Penn State Worry Questionnaire was applied simultaneously to explore the concurrent validity of the scale. The scale (Anti) was given again to 78 subjects chosen at random after 8–10 weeks to study test–retest reliability. The clinical psychologist or psychiatrist responsible for each patient made the diagnosis in a clinical interview.
Statistical analysisAfter the instruments had been applied, data were analyzed using SPSS statistical software v22. First, descriptive analyses were carried out. Then, the dimensionality of the AnTI was examined by confirmatory factor analysis (CFA) with MPLUS 7. Maximum Likelihood (ML) was used as multivariate normality could be assumed. The study sample showed .1% to 2.7% missing data depending on the item, so Full Information Maximum Likelihood (FIML) was used to estimate the model with data missing (Enders & Bandalos, 2001). Model fit was evaluated based on chi-square (X2), the root mean squared error of approximation (RMSEA) and the comparative fit index (CFI). The cutoff points were .08 for the RMSEA (Browne & Cudeck, 1993) and .90 for the CFI (Bollen, 1989).
Internal consistency of the scale's scores was found with McDonald's Omega for each of the three dimensions. test–retest reliability was analyzed using Pearson's r correlation, while the differences by sex were explored with Student's t for independent samples.
Finally, concurrent validity was explored by means of the correlation of the scores on the AnTI and those on the PSWQ, and convergent validity was tested by the correlations between the AnTI scores and those on the BAI and the SCL-90-R.
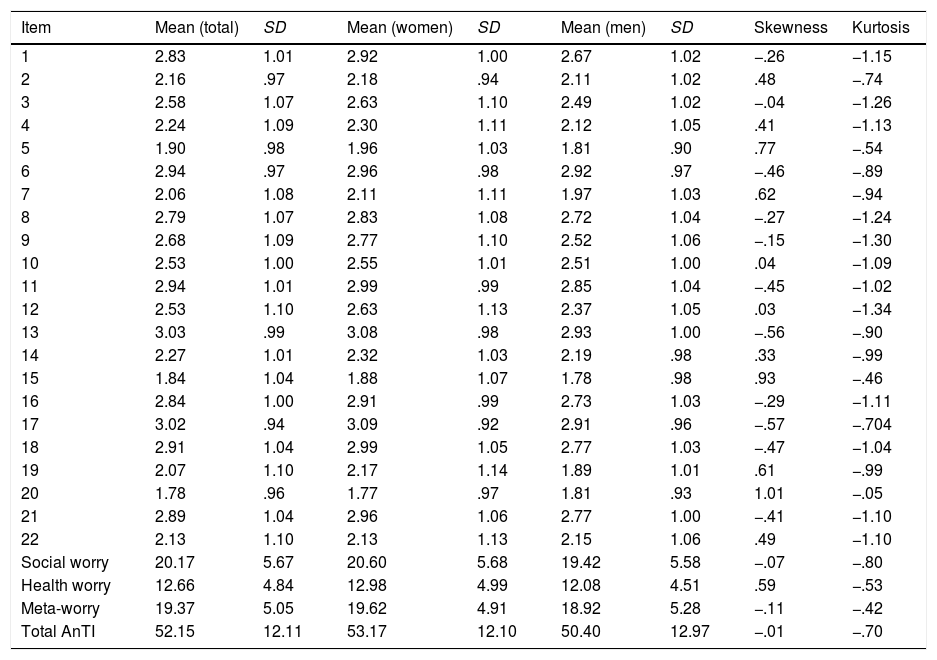
ResultsDescriptive statisticsMeans, standard deviations (total, men and women), skew and kurtosis of responses to the 22 AnTI items, subscales and total are presented in Table 2.
Means, standard deviations (total, women and men), skew and kurtosis of responses to the 22 AnTI items, subscales and total scale scores.
| Item | Mean (total) | SD | Mean (women) | SD | Mean (men) | SD | Skewness | Kurtosis |
|---|---|---|---|---|---|---|---|---|
| 1 | 2.83 | 1.01 | 2.92 | 1.00 | 2.67 | 1.02 | −.26 | −1.15 |
| 2 | 2.16 | .97 | 2.18 | .94 | 2.11 | 1.02 | .48 | −.74 |
| 3 | 2.58 | 1.07 | 2.63 | 1.10 | 2.49 | 1.02 | −.04 | −1.26 |
| 4 | 2.24 | 1.09 | 2.30 | 1.11 | 2.12 | 1.05 | .41 | −1.13 |
| 5 | 1.90 | .98 | 1.96 | 1.03 | 1.81 | .90 | .77 | −.54 |
| 6 | 2.94 | .97 | 2.96 | .98 | 2.92 | .97 | −.46 | −.89 |
| 7 | 2.06 | 1.08 | 2.11 | 1.11 | 1.97 | 1.03 | .62 | −.94 |
| 8 | 2.79 | 1.07 | 2.83 | 1.08 | 2.72 | 1.04 | −.27 | −1.24 |
| 9 | 2.68 | 1.09 | 2.77 | 1.10 | 2.52 | 1.06 | −.15 | −1.30 |
| 10 | 2.53 | 1.00 | 2.55 | 1.01 | 2.51 | 1.00 | .04 | −1.09 |
| 11 | 2.94 | 1.01 | 2.99 | .99 | 2.85 | 1.04 | −.45 | −1.02 |
| 12 | 2.53 | 1.10 | 2.63 | 1.13 | 2.37 | 1.05 | .03 | −1.34 |
| 13 | 3.03 | .99 | 3.08 | .98 | 2.93 | 1.00 | −.56 | −.90 |
| 14 | 2.27 | 1.01 | 2.32 | 1.03 | 2.19 | .98 | .33 | −.99 |
| 15 | 1.84 | 1.04 | 1.88 | 1.07 | 1.78 | .98 | .93 | −.46 |
| 16 | 2.84 | 1.00 | 2.91 | .99 | 2.73 | 1.03 | −.29 | −1.11 |
| 17 | 3.02 | .94 | 3.09 | .92 | 2.91 | .96 | −.57 | −.704 |
| 18 | 2.91 | 1.04 | 2.99 | 1.05 | 2.77 | 1.03 | −.47 | −1.04 |
| 19 | 2.07 | 1.10 | 2.17 | 1.14 | 1.89 | 1.01 | .61 | −.99 |
| 20 | 1.78 | .96 | 1.77 | .97 | 1.81 | .93 | 1.01 | −.05 |
| 21 | 2.89 | 1.04 | 2.96 | 1.06 | 2.77 | 1.00 | −.41 | −1.10 |
| 22 | 2.13 | 1.10 | 2.13 | 1.13 | 2.15 | 1.06 | .49 | −1.10 |
| Social worry | 20.17 | 5.67 | 20.60 | 5.68 | 19.42 | 5.58 | −.07 | −.80 |
| Health worry | 12.66 | 4.84 | 12.98 | 4.99 | 12.08 | 4.51 | .59 | −.53 |
| Meta-worry | 19.37 | 5.05 | 19.62 | 4.91 | 18.92 | 5.28 | −.11 | −.42 |
| Total AnTI | 52.15 | 12.11 | 53.17 | 12.10 | 50.40 | 12.97 | −.01 | −.70 |
Scores were significantly different for men and women on the overall scale (t=2.97; p=.003; d=.22) and the health worry (t=2.39; p=.017; d=19) and social worry dimensions (t=2.67; p=.008; d=21), while there were no significant differences in meta-worry (t=1.77; p=.078; d=14). In spite of the differences observed, the effect size was small. Whenever differences were observed, the highest scores appeared in women.
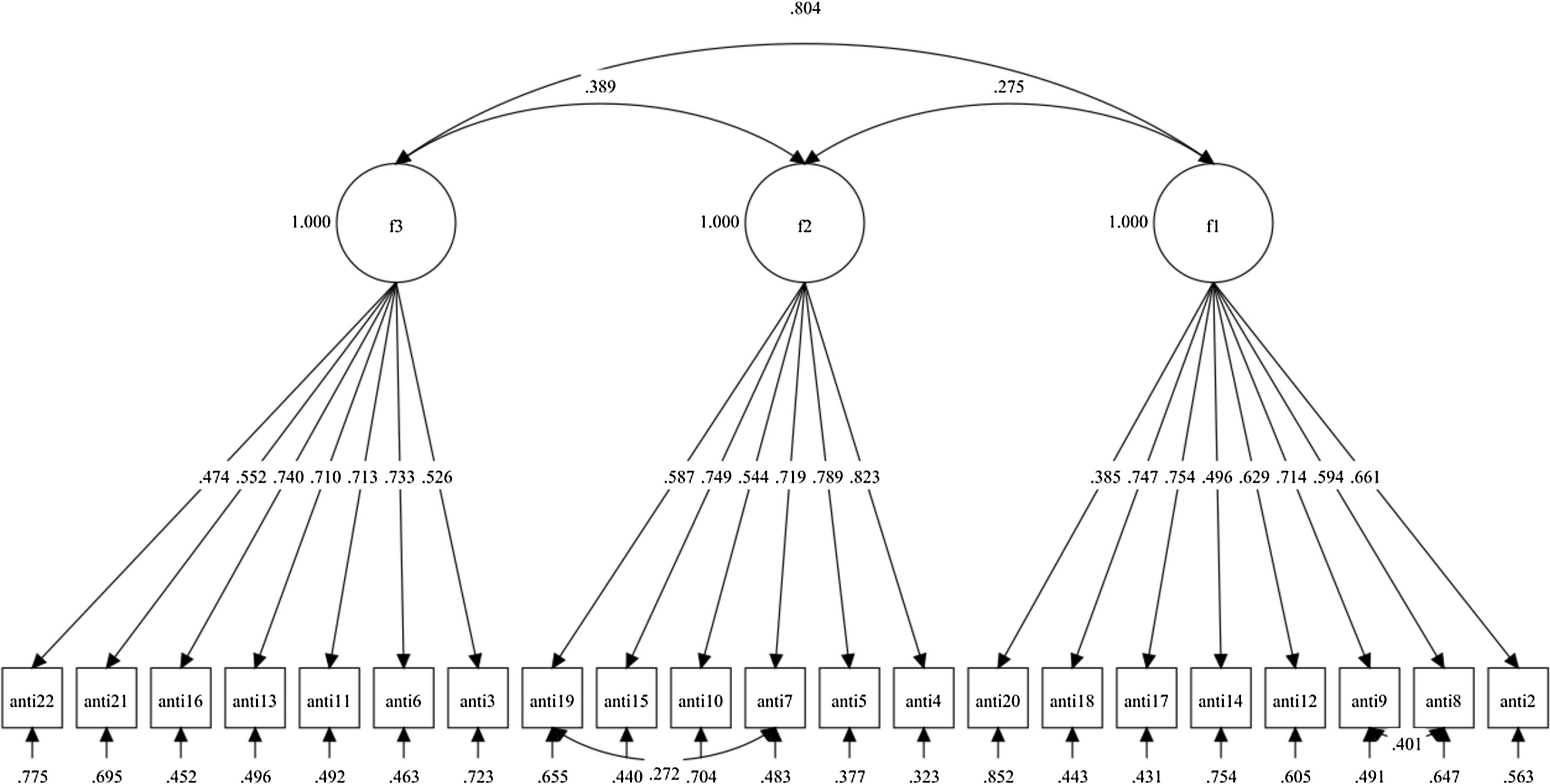
Construct validityThe original AnTI instrument model made up of three correlated factors, social worry, health worry and meta-worry, was tested by CFA. The factor solution of the original model [X2(206)=1067.110; RMSEA=.076; CFI=.865] did not fit well according to the recommended CFI cutoff points. Based on the observation of the factor loadings, it was found that Item 1 saturated below the recommendation on Factor 1 (λ1=.144), and therefore, it was eliminated from the scale. Model fit improved significantly [X2(186)=937.742; RMSEA=.074; CFI=.880], however, the CFI observed was still below the cutoff point. So then the modification indices (MI) were analyzed. According to them, it was advisable to add a covariance error between Items 8 and 9 (MI=94.323). After that, the model again improved significantly [X2(185)=842.606; RMSEA=.070; CFI=.895], however, the CFI was still below .90. Therefore, again based on the MI analysis, a covariance error was added between Items 7 and 19 (MI=42.486). Finally, the model showed adequate fit [X2(184)=801.088; RMSEA=.068; CFI=.901]. In the final model, all the items showed standardized factor loadings from .385 to .823, as observed in Fig. 1.
Alpha reliabilities. Note. Parameters displayed are standardized; f1=Social worry; f2=Health worry; f3=Meta-worry.")
The McDonald's Omega for each subscale was adequate: social worry .84, health worry .86, and meta-worry .83.
Test–retest reliabilityPearson's test–retest correlations found for 78 patients who were given the AnTI for a second time after a period of 8–10 weeks were high in all cases, except in the meta-worry scale, which was somewhat lower: for the social worry subscale .79 (p<.001), for health worry .89 (p<.001), for meta-worry .49 (p<.001) and for the total score on the scale the correlation found was .71 (p<.001).
Concurrent validityIn the analysis of the relationship of the AnTI as a scale for assessing worry with another specific worry assessment instrument like the PSWQ, significant correlations with each of the dimensions and the total score observed had effect sizes from medium to large: r=.40 (p<.05) with the health worry dimension, r=.67 (p<.01) with social worry, r=.75 (p<.01) with meta-worry and r=.78 (p<.01) with the total AnTI score.
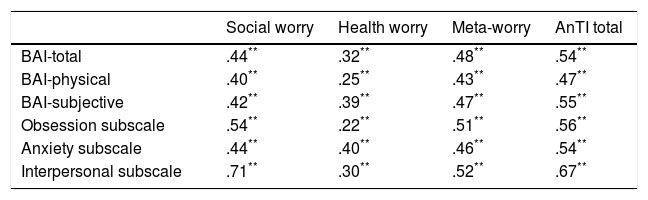
Convergent validityConsidering that worry is a component of anxiety, it is to be expected that AnTI scores would correlate with other anxiety evaluation scales. The relationships observed with two of the most widely used instruments for assessing anxiety, the BAI and the SCL-90-R, showed positive correlations between the overall AnTI scores and the overall BAI (r=.54; p<.001) score and the SCL-90-R anxiety dimension score (r=.54; p<.001). Significant positive correlations were also observed between the various dimensions of these instruments (see Table 3), with effect sizes from medium to large in all cases, except for the health worry subscale with the physical dimension of the BAI and the SCL-90-R obsession subscale, where it was small.
Convergent validity. Pearson correlations between AnTI total score, its subscales, BAI and obsession, anxiety and interpersonal sensitivity SCL-90-R subscales (N=731).
In general terms, the results show adequate psychometric properties of this Spanish adaptation of the AnTI in a clinical population.
According to the results of the confirmatory factor analysis, the adaptation of the AnTI scale to the Spanish clinical population confirms the three original dimensions, social worry, health worry and meta-worry (Wells, 1994), with adequate fit. However, also according to the results found, Item 1 (referred to worry about own appearance), showed low correlation with the rest of the items in the factor, so it was eliminated from the scale. The performance of this item could have different explanations. Although placement of worry about physical appearance in the social worry dimension may seem logical, observation of the rest of the items on this subscale identifies it as the only item that refers to something physical. This could explain its somewhat different behavior. Therefore, it cannot be discarded that, although in general it could be understood from its content as a type of socially related worry, some subjects understand it not as worry, but as interest in their appearance, distancing themselves from the scope of worry reflected by the rest of the items on the social worry subscale. In any case, it would be advisable for future studies to analyze the behavior observed on Item 1 with a view to confirming whether this could be due to the translation itself or simply the characteristics of the study sample.
It should be pointed out concerning the saturation of the items on each of the factors that except for Item 20, which is slightly lower, all the items show saturations above .40, which coincides with those found in the English version. However, saturation of Item 20, although also coinciding in the dimension of social worry, is lower than in the English version. This may be because the meaning of this item is slightly different in these two versions. While in the English version, “lose control of oneself” seems to be understood as worry about portraying a negative self-image, the Spanish version seems to have less of a social connotation, implying a certain worry about controllability of thought processes and of one's own behavior, an aspect which could also have some relationship with meta-worry.
With regard to factor correlations, medium correlations were observed between the social and health worry dimensions as well as between health worry and meta-worry, while the effect size of the correlation between social worry and meta-worry was high. These correlations are similar to those given for the English version, except for social worry and meta-worry. Although in both versions these are the most correlated dimensions, in the English version the correlation is medium and in the Spanish one it is high. Although other explanations may not be discarded, the different composition of the samples could be at the root of this difference, which would be of interest to confirm in new studies.
Regarding reliability, the subscales’ high internal consistency should be emphasized, varying from .83 (meta-worry) to .86 (health worry). These scores are similar to those given by Wells (1994), which varied from .75 (meta-worry) to .84 (social worry) and to those found for the Brazilian adaptation (Moreno et al., 2014) for the overall scale (.86).
Temporal stability of the scale's scores observed in the test–retest correlation was likewise very satisfactory, particularly in the social and health dimensions, both above .78 and somewhat more moderate in meta-worry, which was below the .77 found by Wells (1994). This lower stability could be related partly to the difference in the time interval employed, which was somewhat longer in this study, and also more probably, to the different composition of the samples in the two studies. While the English sample in which temporal stability was explored was comprised exclusively of students, the sample in this study was a clinical population. This could reflect lower stability in the meta-worry dimension scores in a clinical population, a point which must be corroborated in further studies. These results cannot be compared with the Brazilian validation since no data on temporal stability were provided for the scale.
Concerning validity, in the first place, the high correlation of r=.76 between the total score on the AnTI and the PSWQ should be stressed. Also, particularly intense is the correlation with the meta-worry dimension, with an r=.75, which was to be expected given the generic evaluation of worry in this dimension and not specific as in the health and social dimensions. This high correlation with a specific instrument for evaluating worry like the PSWQ supports the validity of the AnTI as a measure of worry assessment.
The AnTI's correlations with other anxiety assessment instruments like the BAI and the SCL-90-R anxiety dimension support its convergent validity, coinciding completely with the results found in other studies on the AnTi (Moreno et al., 2014; Wells, 1994). The high correlation observed between the AnTI social worry and the SCL-90-R interpersonal sensitivity subscale should also be mentioned.
It is of further interest to notice that the results found for gender differences show more worry in women, both in general and in the social and health dimensions, although no differences were observed in meta-worry. Such different scores for the two genders, higher in women, have been shown in other studies, relating them to higher frequency of Generalized Anxiety Disorder in women (Johnson & Whisman, 2013) and pointing out the importance of considering the gender variable in studies on worry.
Among limitations of the study, the absence of a nonclinical sample should be mentioned, as well as the small number of subjects included in some of the diagnostic categories and the diagnostic procedure based on clinical history and diagnostic evaluation in which no structured interviews were used to confirm them. In addition, the factorial invariance by gender or age was not analyzed in this study.
As future lines of research, studies including nonclinical samples with structured interviews and a larger number of subjects with some of the specific diagnoses of anxiety (such as social phobia, dissociative and somatoform disorders) are needed to facilitate the study of discriminant validity of the AnTI with respect to the various anxiety disorders.
The gender differences observed further suggest the need for future studies to analyze the invariance of the scale between men and women by Multigroup Analysis. This analysis would make it possible to understand how the instrument should be adjusted for men and women. In future studies it would also be of interest to analyze invariance across age or clinical diagnoses.
To summarize, the Spanish adaptation of the AnTI may be said to have satisfactory psychometric characteristics, with high reliability and internal consistency, as well as adequate validity, facilitating assessment of basic dimensions of worry and the processes involved. Availability of an instrument with adequate evidence of validity and reliability which can evaluate the content of worry, and differentiate worry (Type 1) from meta-worry (Type 2) could contribute significantly to a better understanding of the role of worry in psychological disorders, especially anxiety disorders, as well as the associated psychological vulnerability, in line with the findings of Nordahl and Wells (2017), contributing to the development of preventive strategies. Similarly, its use in clinical contexts could increase the understanding of the processes underlying psychological disorders and evaluation of the impact of interventions designed for these population groups.
Conflict of interestsThe authors declare that they have no conflict of interest.