

Job stress can have important consequences on the physical, mental or social health of the workers. A considerable number of studies have shown that the nursing community is especially vulnerable to suffering stress due to their work characteristics. The purpose of this research was to determine the relationship between perception of psychosocial risk factors at work, trait-anxiety and mental health in nursing.
MethodTwo hundred and ten nurses from various public hospitals in Madrid Province have participated in this study. The perception of psychosocial risk factors was evaluated with DECORE and NASA-TLX questionnaires, trait-anxiety was measured by STAI questionnaire and mental health by GHQ-28 questionnaire.
ResultsThe results of the multiple regression analysis revealed that trait-anxiety was the variable most related to mental health. To explore the isolated association between working conditions and nurses’ mental health, partial correlations controlling the nurses’ trait-anxiety level were calculated and significant correlations were found between mental health and some psychosocial risk factors like organizational support, cognitive and temporal demands and control/autonomy at work.
ConclusionTrait-anxiety influences the relations between working conditions and nurse's mental health, but regardless of the trait-anxiety level of nurses, the adverse psychosocial conditions of the workplace are directly associated with poorer mental health.
El estrés experimentado en el ámbito laboral puede tener importantes consecuencias para la salud tanto física como mental y/o social de los trabajadores. Un número considerable de investigaciones han demostrado que el colectivo de enfermería es especialmente vulnerable al estrés debido a las características particulares de su labor. El objetivo de este estudio fue analizar las relaciones entre la percepción de riesgos psicosociales, la ansiedad rasgo y la salud mental en profesionales de la enfermería.
MétodoEn este estudio han participado 210 profesionales de enfermería de varios hospitales de la Comunidad Autónoma de Madrid. La percepción de los factores psicosociales de riesgo se ha evaluado mediante los cuestionarios DECORE y NASA/TLX, el nivel de ansiedad rasgo se ha valorado con el cuestionario STAI y la salud mental, con el cuestionario GHQ-28.
ResultadosEl resultado del análisis de regresión múltiple ha revelado que la variable con mayor correlación con la salud mental fue la ansiedad rasgo. Para evaluar la relación, independientemente de la ansiedad rasgo, entre las condiciones laborales y la salud mental de las/los enfermeras/os, se calcularon las correlaciones parciales, controlando el nivel de ansiedad rasgo, y se encontraron correlaciones significativas y positivas entre una peor salud mental y la mayor presencia de factores psicosociales de riesgo, tales como menor apoyo organizacional, demandas cognitivas y temporales más altas y peor nivel de control en el trabajo.
ConclusionesLa ansiedad rasgo influye en la relación entre las condiciones laborales y la salud mental del personal de enfermería, pero independientemente del nivel de ansiedad rasgo, las condiciones laborales adversas se relacionan de forma directa con un peor nivel de salud mental.
During the last decade, the nature of work has changed drastically, mainly due to the worldwide economic crisis and its recent recession, the technological vertiginous progress and the constant economic, socio-political and demographic changes. The restructuring of the organizational environment has increased the dominance of psychosocial risk factors at work and the prevalence of disorders due to stress and work overload (Jensen et al., 2019).
Psychosocial factors refer to the interactions within the work environment, job content, organizational conditions and workers’ capacities, needs, culture, personal extra-job considerations that may, through perceptions and experience, influence health, work performance and job satisfaction (Williams, Buxton, Hinde, Bray, & Berkman, 2017). Psychosocial factors are present in all types of organizations and, depending on the employees’ individual differences, they can be perceived as threatening for their health or, by contrast, if there is an optimal balance between working conditions and individual characteristics, work can become a source of health, wellbeing, satisfaction and motivation (Lorente, Salanova, Martinez, & Vera, 2014).
Work stress is the principal consequence of being exposed to psychosocial risk factors (Sarafis et al., 2016). Although short periods of stress can have an adaptive function, under some condition of intensity, frequency or duration, those reactions can exceed a person's tolerance threshold and can be considered precursors of disease. The exposure to psychosocial risk factors at work is also related to psychosomatic diseases and a significant decline in workers’ mental health (Dewa, Hoch, Nieuwenhuijsen, Parikh, & Sluiter, 2019).
From a physical health point of view, many studies have demonstrated evidence of the relationship between job related stress and an increased risk for cardiovascular, gastrointestinal, respiratory, musculoskeletal and skin problems, central nervous system disorders, alterations of the reproductive system, headaches, migraines, ulcer, diabetes, and the stimulation in the growth of a whole row of chronic diseases, such as cancer (Bernal et al., 2015). The alteration of the behavior processes resulted from the exposure to work-related stress, can lead to substance abuse, unhealthy diets, poor sleep quality and reduced physical activity (Kirilmaz & Santas, 2016).
Unnecessary risk-taking at work, the lower ability to concentrate or to pay attention, the increased number of decision making errors, the diminished quality of work and the possible occurrence of aggressive situations at work, as a result of a stressful work environment, may cause erratic job performance, greater mistakes or accidents and, consequently, work diseases, sick leave and higher absenteeism or turnover rates (Sarafis et al., 2016).
Several authors have affirmed that some employees might be prone to suffer mental disorders facing identical working conditions, since some personality patterns can exert influence in the perception of work environment, making it appear more adverse and more stressful (Parent-Lamarche & Marchand, 2018). An anxious personality, for example, can reduce the capacity for information processing, problem-solving, and the ability to control one's own actions, so more work stressors are perceived, and more distress is experienced. High levels of anxiety produce constant tension and alter the well-being of the workers (Bogiaizian, Solari, Maglio, & López, 2016). Trait-anxiety could explain why the same organizational conditions can help some employees benefit from the work experience but not be helpful to others.
One of the professional groups most vulnerable to job stress is the nursing staff. Several of the obstacles that can negatively affect their mental health status, decrease performance efficiency and increase the workload are the following: A tiring and poorly organized work environment, insufficient medical equipment, large amounts of time spent on non-nursing tasks (like administrative tasks), required attention to patients’ families, high levels of negative affect induced by the unpredictability of the tasks, frequent interruptions in the discharge of their duties and insufficient support. Nurses must deal with demanding tasks, excessive working hours, lack of control over their own work, and effort-reward imbalance, which can activate chronic work stress (Aiken, Sloanea, Bruyneel, Van den Heede, & Sermen, 2013). Sometimes, they must deal with the violent behaviors of patients and families, which imply high emotional demands, directly associated with work stress and exhaustion (Yang, Stone, Petrini, & Morris, 2018). Health care workers are prone to develop both minor (tension, anxiety, depressed, mental fatigue, and sleep disturbance) and major psychiatric disorders (depression, anxiety), which can lead to severe post traumatic syndromes (Ardekani, Kakooei, Ayattollahi, Choobineh, & Seraji, 2008). Also, nurses making the right decisions is of irrefutable importance in the maintenance of high-quality patient care. The decision-making ability is an indispensable part of the nursing profession and is a dynamic, intangible, and complicated process that can affect the outcome of patients. Anxiety is a crucial factor that affects decision-making (Polat, Kutlu, Purİsa, & Erkan, 2019). Making healthy decisions also requires making calm decisions that are free from anxiety. Different feelings can affect decision-making in different ways and high levels of continuous anxiety negatively affect decision-making due to some of the following explanations (Remmers & Zander, 2018): 1. Anxiety, by affecting the ways of processing knowledge, can lead to a tendency of heading toward threat related information, negative interpretation of ambiguous stimuli, and the emergence of the behavior of harm avoidance; 2. Anxiety impairs the effective operation of the attention system toward the target and takes the attention away from the subject by drawing it to another place. Decision-makers, rather than finding the best solution to the current problem, focus on reducing the feeling of anxiety and the stimuli related to the threat; 3. Anxiety, in some cases, might be the cause of the tendency to take excessive risks or avoiding risks. Therefore, reducing work-related stressors among nurses is essential for the prevention of medical errors and the improvement in the quality of nursing care.
The negative and unfavorable effect of job stress can cause accidents. Anxiety and stress may cause nurses to not comply with the rules and consequently not pay attention to alarming signs (Khamisa, Peltzer, Ilic, & Oldenburg, 2016). Thus, recognizing the impact of anxiety and work-related stressors on general health and the effects of nurses’ general health on poor job performance, absenteeism and increased healthcare costs is important (Poursadeghiyan et al., 2016).
Aims and hypothesisThe main goal of this research was to determine how perception of psychosocial risk factors and mental workload (stressors) are related to mental health in a group of nurses from various public hospitals in Madrid Province (Spain), considering trait-anxiety as a personality factor associated with the individuals’ perception of their working conditions and their health. The hypothesis was that trait-anxiety will be strongly related to nurses’ mental health but when controlling statistically its effect, other organizational factors, such as mental workload, organizational support and task control, will enable the prediction of mental health levels.
MethodParticipantsA descriptive cross-sectional study was conducted with a sample of 210 nurses from several public hospitals in Madrid Province. One hundred and seventy-seven were female and the other 33 participants were male. The age of the participants ranged between 22 and 62 years old, with a mean of 38.45 years (SD=8.37). The mean work experience was approximately 10 years (SD=6.50).
InstrumentsA battery of tests was applied, including the following instruments:
Socio-demographic questionnaireGender, age and years of work experience were included in this questionnaire.
The General Health Questionnaire (GHQ-28)To obtain information on common, non-specific psychiatric problems, the 28-item version of the General Health Questionnaire (GHQ-28) adapted to Spanish population by Lobo, Perez-Echeverría and Artal (1986) was used. GHQ-28 is a self-administered screening tool designed to detect the susceptibility of developing non-psychotic mental disorders in the general population. GHQ-28 has shown high reliability coefficients: α=.97 for the total scale, and between .91 and .97 for the subscales (Godoy-Izquierdo, Godoy, López-Torrecilla, & Sánchez-Barrera, 2002). GHQ-28 is composed of four scales: somatic symptoms (feeling of exhaustion or bodily discomfort); anxiety-insomnia (nervousness, anxiety and sleep problems); social dysfunction (problems related to performance and enjoyment of daily activities) and severe depression (thoughts and feelings of worthlessness, sadness and suicide). The score for each of the items varies from 0 (No, not at all or Better than usual) to 3 (Much worse than usual), so for each dimension a total score from 0 to 21 is possible, showing poorer health as the score gets higher. A score greater than or equal to 13 (cut-off score) in each dimension was considered an indicator of health problems.
State-Trait-Anxiety Inventory (STAI)The STAI (Spielberger, Gorsuch, & Lushene, 1970) is one of the most useful tools to assess anxiety in applied psychology research (Buela-Casal, Guillén–Riquelme, & Seisdedos-Cubero 2011). It provides a measure for two psychological dimensions: state anxiety (transient emotional condition) and/or trait-anxiety (relatively stable anxiety proneness). The Spanish version of the scale was employed to detect those individuals who generally feel anxious, leading them to perceive situations as more threatening. The response scale for each item varies from 0 (hardly ever) to 3 (almost always). A higher STAI total score indicates a higher level of anxiety. The Spanish version of the STAI presents enough methodological guarantees related to its validity and reliability and it is useful to assess the predisposition to anxiety in various settings (α=.90). Normative scores are available for the Spanish population. All participants with a percentile higher than or equal to 70 were considered to have anxiety problems (cut-off score).
DECORE Multidimensional QuestionnaireThe perception of psychosocial risk factors was assessed with the DECORE Multidimensional Questionnaire (Luceño-Moreno & Martín-García, 2008). It is developed for the Spanish working population and its basic assumption is that high demands, low control, lack of support and imbalanced perceived rewards are the main psychosocial risk factors that significantly contribute to the increase of workers’ mental strain. DECORE includes 44 items (Likert response scale from 1, strongly disagree to 5, strongly agree) grouped in four factors: Job Control (assesses workers’ freedom to decide on issues that affect their work), Organizational Support (assesses the quality of the relationships established with the supervisor or colleagues), Rewards (assesses the benefits that workers perceive, essentially economic performance and job security) and Job Cognitive Demands (assesses the quantitative and qualitative aspects of their job requirements, in relation to how much they work). Higher scores indicate a negative perception of the work environment and, therefore, higher psychosocial risk exposure. Furthermore, it provides a global risk index that enables us to have a global vision of the psychosocial situation and classifies the exposure to risk into 4 levels (excellent, healthy, alert and emergency). Alert and emergency levels represent an inadequate risk exposure. DECORE has adequate reliability (α≥.72) and validity (Luceño-Moreno, Martín-García, Rubio-Valdehita, & Díaz-Ramiro, 2010).
NASA-Task Load Index (TLX)The NASA-TLX questionnaire (Hart & Staveland, 1988) was used to evaluate the perceived mental workload. NASA-TLX is a subjective and multidimensional tool that offers a global score based on the average of six dimensions: mental demand (degree of mental and perceptual activity required); physical demand (how much physical activity is required); temporal demand (ratio between requested time and perceived pressure); performance (to what extent is the person satisfied with his/her level of performance); effort (how hard does the person have to work to accomplish that level of performance) and frustration (how insecure, discouraged, irritated, stressed, annoyed does the person feel during the tasks). A workload score from 0 to 100 is obtained for each dimension, showing more workload as the score gets higher. Scores higher than 50 indicate an excessive workload (cut-off score). NASA-TLX is the most widely used mental workload assessment instrument as it has proven to be reliable (α=.82) and valid (Díaz-Ramiro, Rubio-Valdehita, Martín-García, & Luceño-Moreno, 2010).
ProcedureThis study is part of a broader research aimed to assess the perception of the working conditions of workers in public hospitals. The first step was to contact the Prevention Services of Madrid's public hospitals to explain the research goals and the procedure. Once the study was approved by the Ethics Committee of the authors’ research center and by the hospital's managers, several instruments were applied to nurses, who participated voluntarily and anonymously, and signed an informed consent. The instruments were always applied in their paper and pencil versions. All sessions were held in small groups of 5 to 10 workers in a hospital room and during the nurses’ workday.
Data analysisSPSS version 22.0 for Windows was used for data analysis. The relationships between dimensions were tested using stepwise multiple regression analyses. First, the total GHQ-28 score was the criterion or dependent variable, and later, each GHQ-28 subscale was introduced as a criterion variable. The predictor variables in all the regression analyses were the subscales of the other questionnaires used in the present study. Next, the same analysis was repeated controlling the effect of participants’ trait-anxiety, using partial correlations as input.
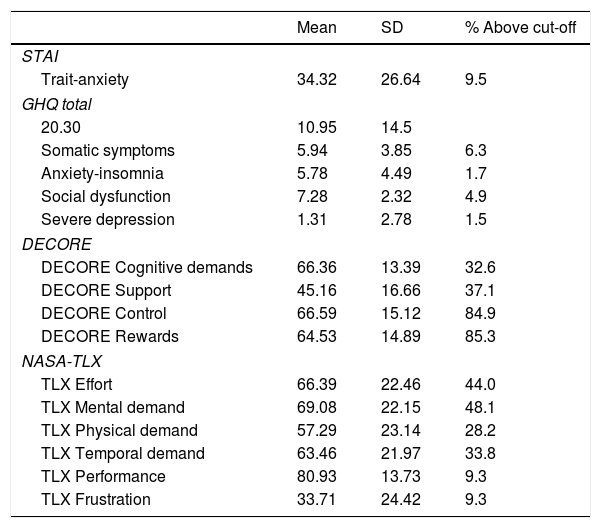
ResultsTable 1 shows means, standard deviations (SD) and percentage (%) of people scoring over the cut-off scores for all measures. The percentage (%) of people over the cut-off represents the percentage of nurses who achieved scores in alert or emergency regarding their perception of psychosocial risks, over 70 on mental workload, more than 12 in GHQ-28 subscales, or over percentile 70 on trait-anxiety.
Mean, standard deviation (SD) and % of people above cut-off on health, psychosocial factors perception, mental workload and trait-anxiety.
| Mean | SD | % Above cut-off | |
|---|---|---|---|
| STAI | |||
| Trait-anxiety | 34.32 | 26.64 | 9.5 |
| GHQ total | |||
| 20.30 | 10.95 | 14.5 | |
| Somatic symptoms | 5.94 | 3.85 | 6.3 |
| Anxiety-insomnia | 5.78 | 4.49 | 1.7 |
| Social dysfunction | 7.28 | 2.32 | 4.9 |
| Severe depression | 1.31 | 2.78 | 1.5 |
| DECORE | |||
| DECORE Cognitive demands | 66.36 | 13.39 | 32.6 |
| DECORE Support | 45.16 | 16.66 | 37.1 |
| DECORE Control | 66.59 | 15.12 | 84.9 |
| DECORE Rewards | 64.53 | 14.89 | 85.3 |
| NASA-TLX | |||
| TLX Effort | 66.39 | 22.46 | 44.0 |
| TLX Mental demand | 69.08 | 22.15 | 48.1 |
| TLX Physical demand | 57.29 | 23.14 | 28.2 |
| TLX Temporal demand | 63.46 | 21.97 | 33.8 |
| TLX Performance | 80.93 | 13.73 | 9.3 |
| TLX Frustration | 33.71 | 24.42 | 9.3 |
According to the scores obtained in DECORE, about 86% of participants were in a situation of psychosocial risk as cognitive demands, control and rewards were negatively perceived. In contrast, social support was positively perceived. A general alert situation was identified given that the Global Risk Index mean was high (M=66.80, SD=14.90). About 40% of the participants ranked on the emergency level and 48% on alert. All psychosocial risk factors are found in the alert level, except for organizational support that is within a healthy level. Interpersonal relationships established with both supervisors and co-workers are positively perceived. Cognitive demands are considered adequate. Nevertheless, control at work and rewards are considered insufficient.
The global mental workload score (the average of the six NASA-TLX dimensions) was considered intermediate (M=51.50; SD=14.40). Frustration was particularly low.
In general, the trait-anxiety of our nurses was low, although a 9.5% showed high scores (over the 75 percentile).
The mental health of the nurses in our study was mostly good. Only 6% of the participants showed some psychological health deficit, mainly due to the presence of somatic symptoms and social dysfunction. Less than 2% of participants presented symptoms of severe depression.
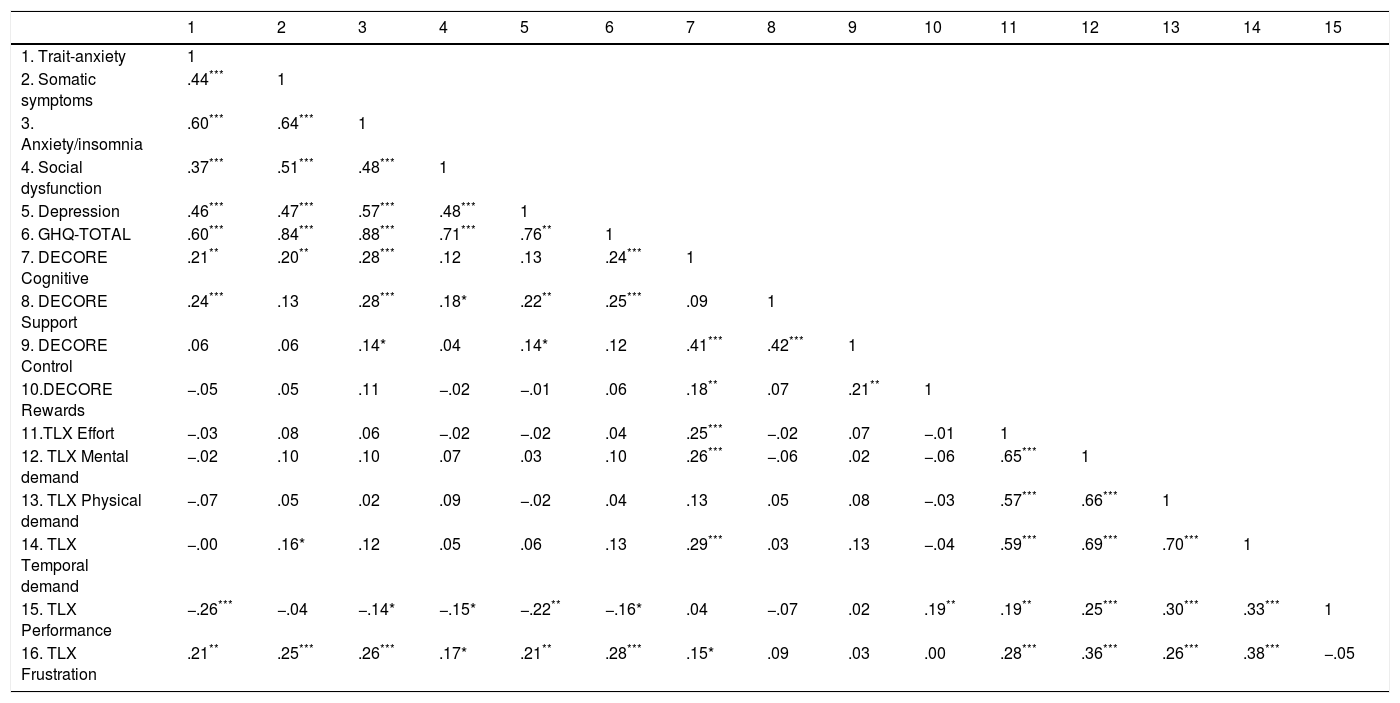
Models for prediction of nurses’ mental healthTable 2 shows the Pearson correlation coefficients between all variables. Significant correlations were found between some variables. Trait-anxiety correlated with psychological health; the higher the anxiety score, the poorer the health participants showed. Furthermore, it was found that higher levels of trait-anxiety were associated to lower job performance and greater frustration.
Pearson correlation coefficients between all measures.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Trait-anxiety | 1 | ||||||||||||||
| 2. Somatic symptoms | .44*** | 1 | |||||||||||||
| 3. Anxiety/insomnia | .60*** | .64*** | 1 | ||||||||||||
| 4. Social dysfunction | .37*** | .51*** | .48*** | 1 | |||||||||||
| 5. Depression | .46*** | .47*** | .57*** | .48*** | 1 | ||||||||||
| 6. GHQ-TOTAL | .60*** | .84*** | .88*** | .71*** | .76** | 1 | |||||||||
| 7. DECORE Cognitive | .21** | .20** | .28*** | .12 | .13 | .24*** | 1 | ||||||||
| 8. DECORE Support | .24*** | .13 | .28*** | .18* | .22** | .25*** | .09 | 1 | |||||||
| 9. DECORE Control | .06 | .06 | .14* | .04 | .14* | .12 | .41*** | .42*** | 1 | ||||||
| 10.DECORE Rewards | −.05 | .05 | .11 | −.02 | −.01 | .06 | .18** | .07 | .21** | 1 | |||||
| 11.TLX Effort | −.03 | .08 | .06 | −.02 | −.02 | .04 | .25*** | −.02 | .07 | −.01 | 1 | ||||
| 12. TLX Mental demand | −.02 | .10 | .10 | .07 | .03 | .10 | .26*** | −.06 | .02 | −.06 | .65*** | 1 | |||
| 13. TLX Physical demand | −.07 | .05 | .02 | .09 | −.02 | .04 | .13 | .05 | .08 | −.03 | .57*** | .66*** | 1 | ||
| 14. TLX Temporal demand | −.00 | .16* | .12 | .05 | .06 | .13 | .29*** | .03 | .13 | −.04 | .59*** | .69*** | .70*** | 1 | |
| 15. TLX Performance | −.26*** | −.04 | −.14* | −.15* | −.22** | −.16* | .04 | −.07 | .02 | .19** | .19** | .25*** | .30*** | .33*** | 1 |
| 16. TLX Frustration | .21** | .25*** | .26*** | .17* | .21** | .28*** | .15* | .09 | .03 | .00 | .28*** | .36*** | .26*** | .38*** | −.05 |
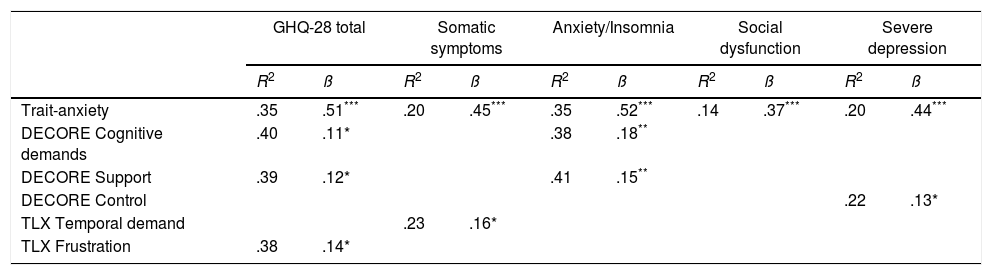
To test the influence of trait-anxiety and working conditions (psychosocial risks and mental workload) on each of mental health dimensions, a stepwise multiple regression analysis was performed. Table 3 shows the results for the predictors that were significant. Trait-anxiety and temporal demands were predictors of somatic symptoms. Anxiety/insomnia scores were predicted by trait-anxiety, cognitive demands and organizational support. Depression was associated with trait anxiety and control, and social dysfunction only with trait anxiety. The rest of the variables considered in the research were not significant (p>.05 in all cases), that is why they are not included in the table.
Prediction of mental health.
| GHQ-28 total | Somatic symptoms | Anxiety/Insomnia | Social dysfunction | Severe depression | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| R2 | ß | R2 | ß | R2 | ß | R2 | ß | R2 | ß | |
| Trait-anxiety | .35 | .51*** | .20 | .45*** | .35 | .52*** | .14 | .37*** | .20 | .44*** |
| DECORE Cognitive demands | .40 | .11* | .38 | .18** | ||||||
| DECORE Support | .39 | .12* | .41 | .15** | ||||||
| DECORE Control | .22 | .13* | ||||||||
| TLX Temporal demand | .23 | .16* | ||||||||
| TLX Frustration | .38 | .14* | ||||||||
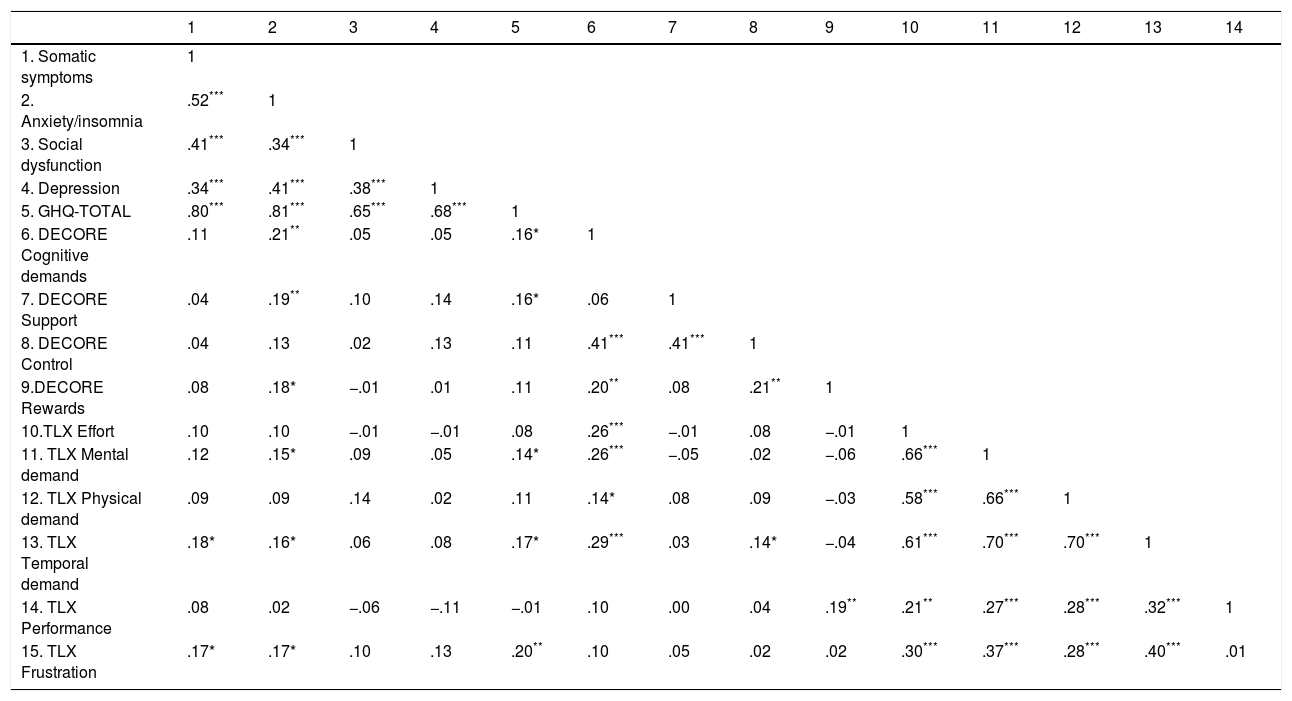
In view of these results, we concluded that trait-anxiety makes the strongest contribution to explaining participants’ metal health. To explore the sole influence of work conditions on mental health, regression analyses were repeated using partial correlations as input, controlling the moderating effect of participants’ trait-anxiety. Table 4 shows the partial correlation coefficients between mental health and psychosocial risk factors. Significant relationships were found between the dimensions of the GHQ-28 and between the dimensions of NASA-TLX. The association between control and cognitive demands of DECORE was also significant, as well as amongst control and organizational support. In this sense, the lack of job control was associated with higher cognitive demands and lower organizational support.
Partial correlation coefficients between measures, controlling trait-anxiety effect.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Somatic symptoms | 1 | |||||||||||||
| 2. Anxiety/insomnia | .52*** | 1 | ||||||||||||
| 3. Social dysfunction | .41*** | .34*** | 1 | |||||||||||
| 4. Depression | .34*** | .41*** | .38*** | 1 | ||||||||||
| 5. GHQ-TOTAL | .80*** | .81*** | .65*** | .68*** | 1 | |||||||||
| 6. DECORE Cognitive demands | .11 | .21** | .05 | .05 | .16* | 1 | ||||||||
| 7. DECORE Support | .04 | .19** | .10 | .14 | .16* | .06 | 1 | |||||||
| 8. DECORE Control | .04 | .13 | .02 | .13 | .11 | .41*** | .41*** | 1 | ||||||
| 9.DECORE Rewards | .08 | .18* | −.01 | .01 | .11 | .20** | .08 | .21** | 1 | |||||
| 10.TLX Effort | .10 | .10 | −.01 | −.01 | .08 | .26*** | −.01 | .08 | −.01 | 1 | ||||
| 11. TLX Mental demand | .12 | .15* | .09 | .05 | .14* | .26*** | −.05 | .02 | −.06 | .66*** | 1 | |||
| 12. TLX Physical demand | .09 | .09 | .14 | .02 | .11 | .14* | .08 | .09 | −.03 | .58*** | .66*** | 1 | ||
| 13. TLX Temporal demand | .18* | .16* | .06 | .08 | .17* | .29*** | .03 | .14* | −.04 | .61*** | .70*** | .70*** | 1 | |
| 14. TLX Performance | .08 | .02 | −.06 | −.11 | −.01 | .10 | .00 | .04 | .19** | .21** | .27*** | .28*** | .32*** | 1 |
| 15. TLX Frustration | .17* | .17* | .10 | .13 | .20** | .10 | .05 | .02 | .02 | .30*** | .37*** | .28*** | .40*** | .01 |
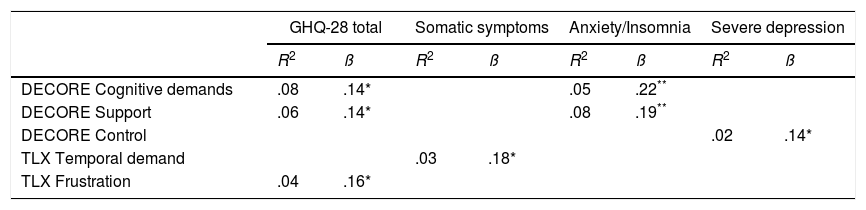
Table 5 shows the results of the multiple linear regression analysis carried out controlling the effect of trait-anxiety. Frustration, organizational support and cognitive demands were significant predictors of global mental health. The rest of the variables were not significant (p>.05 in all cases). Regarding social dysfunction, none of the predictors were statistically significant (p>.05 in all cases).
Prediction of mental health controlling nurses’ trait-anxiety.
Our results support the findings of other studies concerning the impact of adverse working conditions on the mental health of nurses (Díaz-Ramiro, Rubio-Valdehita, López, & Aparicio, 2020). Approximately 90% of our participants reported a negative perception of their psychosocial working conditions, since their perception of control and rewards exceeded the limits considered tolerable (see Table 1). Similar results were found by Kane (2009) in a study with Indian nurses. Kirilmaz and Santas (2016) also found a high rate of job stress in nurses from Turkey.
Most of our nurses were satisfied with their jobs and, hence, their frustration was low. This may be due to nursing having a strong vocational character (Kirilmaz & Santas, 2016). In our study, we determined that satisfaction with rewards was not significantly related to psychological well-being. However, the absence of control at work was a significant predictor of depression scores. The lack of control in nursing may be a result of the accelerating changes in the health sector and the unpredictability of their tasks (Aiken et al., 2013), and, many times, nursing is not adequately remunerated, has no promotional prospects and their salaries are considered low (Mosadeghrad, 2013; Oliveira, Pinel, Gonçalves, & Diniz, 2013).
In contrast, our results showed that organizational support was in general positively perceived. Some previous studies found social and organizational support to be of high quality (Freiman & Merisalu, 2015), but others have shown that nursing is characterized by poor communication and collaboration with others, and by conflictive relationships with physicians and peers (Mosadeghrad, 2013). Our results pointed out that the lack of good organizational support is significantly associated with higher scores in anxiety and insomnia, even when controlling the trait-anxiety of the participant.
In our research, mental demand was the most significant source of nurses’ workload, followed by temporal and physical demands. As previous research has pointed out, nursing involves abundant responsibilities and a relevant amount of cognitive and emotional demands that have to be carried out at a very fast pace (Freiman & Merisalu, 2015). Time pressure, excessive workload and the obligation to do administrative tasks, are just a few of the potential sources of discomfort for nurses, as these reduce the available time to perform specific nursing tasks (Mosadeghrad, 2013). Our results indicate that high cognitive demands are associated with high levels of anxiety and insomnia, while temporary demands would be directly related to the presence of more somatic symptoms.
We have also found that trait-anxiety plays a relevant role in determining the mental health of the nurses who participated in the study. High anxiety was associated with worse mental health. Nurses’ psychological health was also related, although to a lesser extent, with insufficient organizational support and high cognitive demands. Similarly, Freiman and Merisalu (2015), with a sample of 404 Estonian nurses, found that quantitative and emotional demands, work pace and role conflicts were related to mental health problems.
Having an anxious personality has proven to be the main factor related to the anxiety/insomnia scores. This statement could be considered obvious given that those individuals with elevated levels of trait-anxiety are more likely to have higher state-anxiety. Certain adverse organizational factors tend to aggravate perceived risk and can lead to severe anxiety and, in worse cases, to develop frequent anxiety reactions. The quality of personal relationships established at work as well as cognitive requirements may have an impact on nervousness, tension, anxiety and sleep problems. In other studies, it was revealed that temporal demands have a huge role in the increasing of anxiety and insomnia. Work shifts produce fatigue, irritability, difficulty to concentrate and may also affect the quality and quantity of sleep (Jaafarpour & Khani, 2012). Recently, Díaz-Ramiro et al. (2020) observed that the perceived psychological wellbeing of healthcare professionals from Madrid is connected to sleep quality and daytime sleepiness and, in addition, they confirmed that high trait-anxiety is related to a decline in performance and satisfaction with daily activities (social dysfunction). Similarly, Ardekani et al. (2008) stated that fixed work shifts in the nursing community were associated with both the anxiety/insomnia and the social dysfunction scales, and Gómez-García et al. (2016) have highlighted that a working environment with insufficient resources, economic constraints, and time pressure, may reduce the quality of care in hospitals and lead to develop feelings of frustration and weakness in health-care professionals.
An important correlation between trait-anxiety and the severe depression scale was found. This result suggests that anxious proneness can influence those thoughts and feelings of worthlessness, sadness, hopelessness and suicide. Also, the lack of autonomy to decide about issues related to the own work (control), has been found to be a significant factor associated to the severe depression score. These results agree with other researches that have as well found a strong correlation between the development of the depression symptomatology, work demands and organizational support (Jensen et al., 2019).
Since the perception of the working conditions can be influenced by personality, we controlled the effect of trait-anxiety, so that the assessment of psychosocial risks was not affected by this personal factor. In this case, the results showed that regardless of the trait-anxiety level, the adverse psychosocial conditions of the workplace are directly associated with worse levels of mental health. High cognitive and temporal demands, lack of social support, and an insufficient control over the tasks, are psychosocial risk factors especially associated with worse mental health in nursing. It is necessary, therefore, to consider that although personality could play an important role in the development of mental health problems at work, when the impact of a psychosocial factor is permanent, individual predisposition may be less important.
Finally, Aalto, Heponiemi, Josefsson, Arffman, and Elovainio (2018) concluded that health-care organizations should take actions to decrease the workload and increase organizational support of employees. In this sense, we think that the results of our study could have useful and practical implications.
Sources of fundingThe present work has been, in part, funded by the National Institute of Safety and Hygiene (INSHT), an agency under the Spanish Ministry of Labor and Social Affairs (Ref. UCM/CARMEN).
Conflict of interestNone declared.