



The cases are presented on 2 patients with bacterial endogenous endophthalmitis. The first one was caused by Streptococcus bovis, developed after colonoscopy, which had a poor outcome and resulted in evisceration. The second case was caused by a methicillin resistant Staphylococcus aureus from an arthrodesis complicated with a para-spinal abscess. It had an excellent visual outcome.
DiscussionBacterial endogenous endophthalmitis is a rare, but serious ocular disease that occurs when bacteria reach the eye via the bloodstream. It requires a very early diagnosis based on the clinical symptoms and patient history. A suitable and specific treatment with intravenous and intravitreal antibiotics may prevent a bad visual prognosis in some cases.
Presentamos 2 casos clínicos de endoftalmitis endógena bacteriana. El primero causado por Streptococcus bovis tras la realización de una colonoscopia, con mala evolución que acabó en evisceración. El segundo debido a un Staphylococcus aureus meticilin resistente procedente de un absceso paraespinal que complicaba una artrodesis, con excelente recuperación visual.
DiscusiónLa endoftalmitis endógena bacteriana es una enfermedad poco frecuente y grave en la que bacterias procedentes de un foco primario llegan por vía sanguínea hasta el ojo. El diagnóstico de sospecha ha de ser lo más precoz posible, basado en la clínica y los antecedentes del paciente. Un tratamiento adecuado y específico con antibióticos intravenosos e intravítreos puede evitar el mal pronóstico visual en algunos casos.
Endogenous endophthalmitis (EE) or metastatic endophthalmitis is a severe disease with poor visual prognosis caused by the hematogenous dissemination of bacteria or fungi from a primary infectious loci to the ocular globe.1,2 EE accounts for 2–8% of endophthalmitis cases, usually with a predisposing previous disease such as diabetes, cardiovascular or hepatic disease, neoplasia, catheterization or other pharmacologically or biological immunosuppressed conditions.1–3
Two clinical case of bacterian EE are reported, exhibiting different presentations, etiologies and responses to treatment.
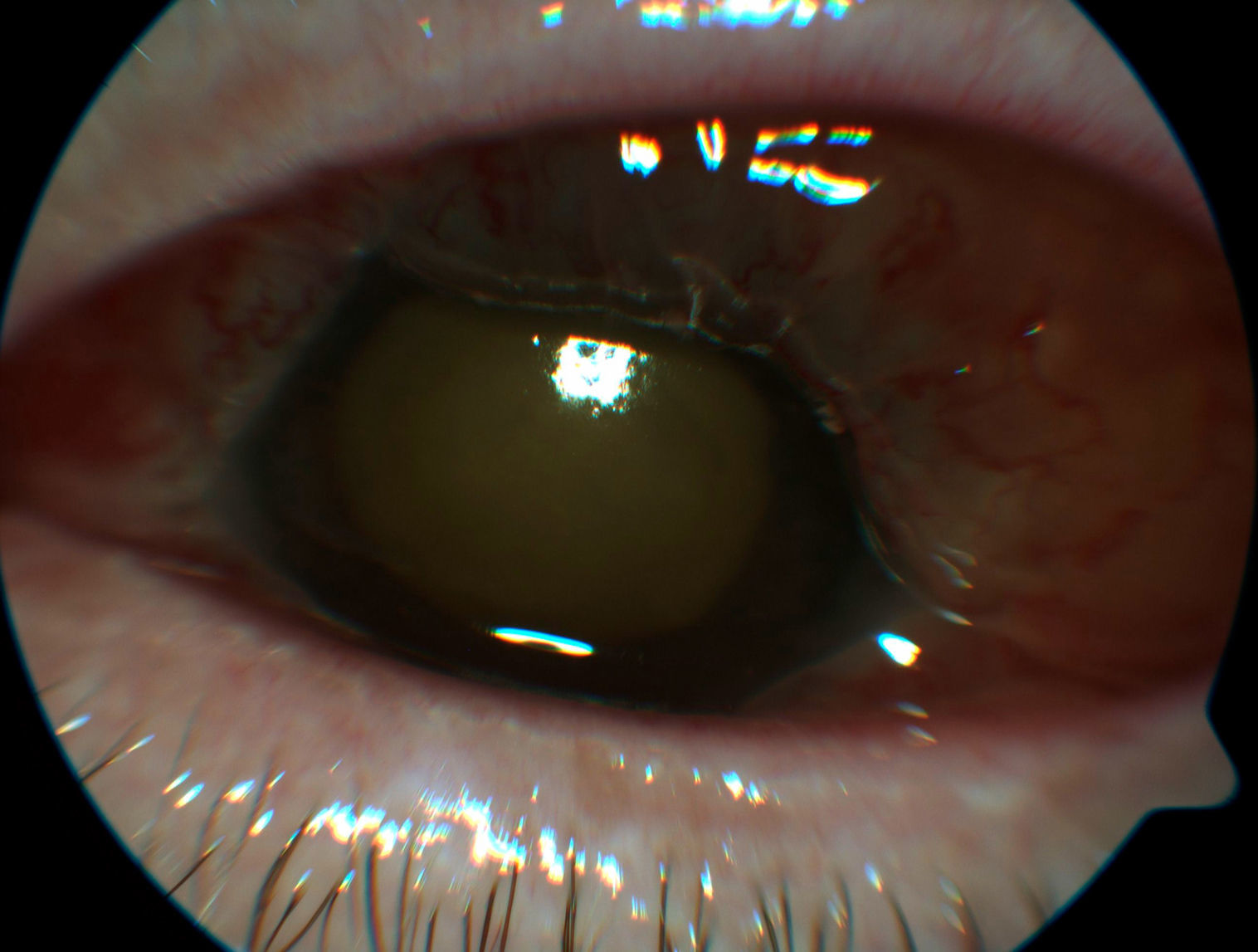
Clinical casesCase 1Female, 69, diabetic in treatment with insulin, hypertension and ischemic cardiopathy who had undergone colonoscopy 3 and 6 months earlier due to polyps. She visited the general Ophthalmology Emergency Dept. due to blurred vision and pain in the left eye (LE) with 3 days evolution. She was diagnosed with hemovitreous. Twenty-four hours later, the right eye (RE) exhibited visual acuity of 0.5, whereas the left eye (LE) exhibited hands movement VA with chemosis, hypopyon, and fibrin in the pupillary area, nuclear cataract, 45mmHg IOP and inability to visualize fundus due to vitreous occupancy confirmed with echography (Fig. 1). Due to suspected EE, intravenous therapy was initiated with vancomycin, ceftazidim and fluconazol as well as intravitreal vancomycin repeated 72h later. Blood cultures were negative. Poor evolution required evisceration after 10 days. The microbiological analysis of eviscerated material isolated Streptococcus bovis. The Cardiology Dept considered there were no signs of bacterial endocarditis, for which reason echocardiogram was not carried out.
Case 2
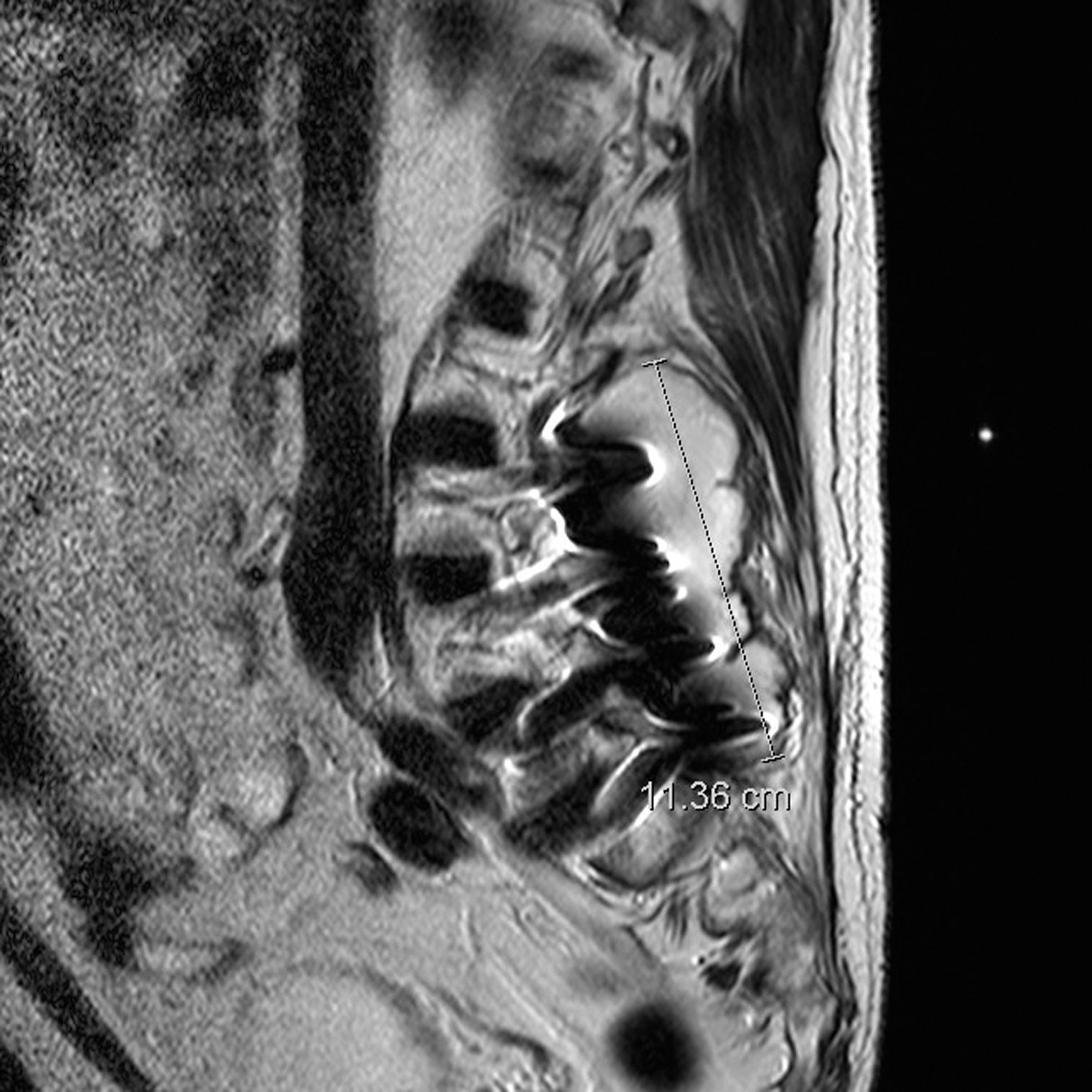
Male, 76, admitted to Internal Medicine exhibiting fever, lumbar pain and right elbow bursitis 9 months after lumbar arthrodesis surgery (reintervened one month later due to cerebrospinal fluid fistula). The bursitis was punctured and methicillin-resistant Staphylococcus aureus (MRSA) was isolated. Intravenous treatment was initiated with rifampicin and cloxacillin but 2 days after admittance the patient exhibited a painless loss of vision in the LE with finger counting VA at 3m, 1mm hypopyon, IOP of 6mmHg, tyndall and dense vitritis that prevented fundus visualization. Right eye examination was normal, with VA of 1. Topical corticoids and antibiotics were added, together with intravitreal vancomycin repeated 72h later despite positive clinic evolution. Computerized action tomography revealed a paraspinal abscess (Fig. 2) and blood culture as well as abscess samples gave positive for MRSA. Accordingly, simultaneous drainage of the abscess and elbow bursitis was performed, upon which the systemic condition resolved and VA exhibited excellent evolution and recovered the value of 1.
Discussion with paraspinal abscess measuring 11.3×10cm around the arthrodesis.")
Bacterial EE is an infrequent disease with very poor visual prognostic.4,5 Ocular signs and symptoms are similar to exogenous endophthalmitis with diminished vision, pain, absence of brightness, hypopyon, vitritis, tyndall, palpebral edema and ocular hypertension. Some cases are nonspecific, which could lead to diagnostic error.3 In addition, EE presents bilaterally in 25% of cases and has a mortality of 4%, above all if systemic antibiotics are not administered.4,5
When bacterial EE is suspected, empirical treatment must be established with intravenous drugs which are crucial because, in contrast with exogenous endophthalmitis, dissemination takes place through the bloodstream.3 Broad range antibiotics are generally applied, such as a vancomycin for Gram+, ceftazidime for Gram− or fourth-generation quinolones such as moxifloxacin that cover both types of bacteria.1,4 Therapy seems to be more effective when associating intravitreal administration such as vancomycin (1mg/0.1ml) and ceftazidime (2mg/0.1ml), that can be repeated 48h later if no clinical improvement is observed.2–4,6 The role of vitrectomy is not defined although the best results are obtained when performed with an acceptable baseline VA, even more so if the bacteria is a Gram+ cocci.4,6 Fungal endophthalmitis suspicion requires systemic fluconazole and intravitreal amphotericin.2
The definitive diagnostic of bacterial EE requires cultures to identify the germ which, in blood, are positive in approximately 50% whereas in intraocular samples (vitreous and aqueous) the percentage ranges between 36 and 73%.4–6 The most frequent original loci are hepatic abscesses, catheters, genitourinary tract infections, endocarditis, meningitis, pneumonia, arthritis, peritonitis and cerebral abscesses.1,2,7 If the patient presents with isolated ocular symptoms, infectious tracking tests can be carried out such as abdominopelvic CAT, abdominal echography, echocardiography and vertebral magnetic resonance to detect hepatic abscesses, endocarditis or osteomyelitis.6
In the first patient, S. bovis was cultured in the evisceration material. This bacteria is typically found in the digestive system, which is consistent with previous colonoscopy that can produce temporary bacteremia.8 The second case had a paraspinal abscess produced by a MRSA, a complication of a lumbar arthrodesis, frequently resistant to fourth-generation quinolones but not to vancomycin.9 In what concerns management, not knowing the germ in the first case recommended the association of intravitreal ceftazidime with a vancomycin, while in the latter case the isolation of MRSA in bursitis justified the exclusive use of intravitreal vancomycin, although the excellent response did not encourage a different dosage. None of the cases underwent vitreous biopsy.
The end result is highly variable, ranging from no perception of light or evisceration to VA similar to pre-existing values. Even so, despite adequate and early treatment, over 50% of cases end up with VA below 0.1, above all with Gram− bacteria.4,5
Conflict of interestsNo conflict of interests was declared by the authors.
Please cite this article as: Cubillas M, Sampedro A, Domínguez B, Carrio I, Bango V, Barbón JJ. Endoftalmitis endógenas bacterianas. A propósito de 2 casos. Arch Soc Esp Oftalmol. 2017;92:280–282.
