



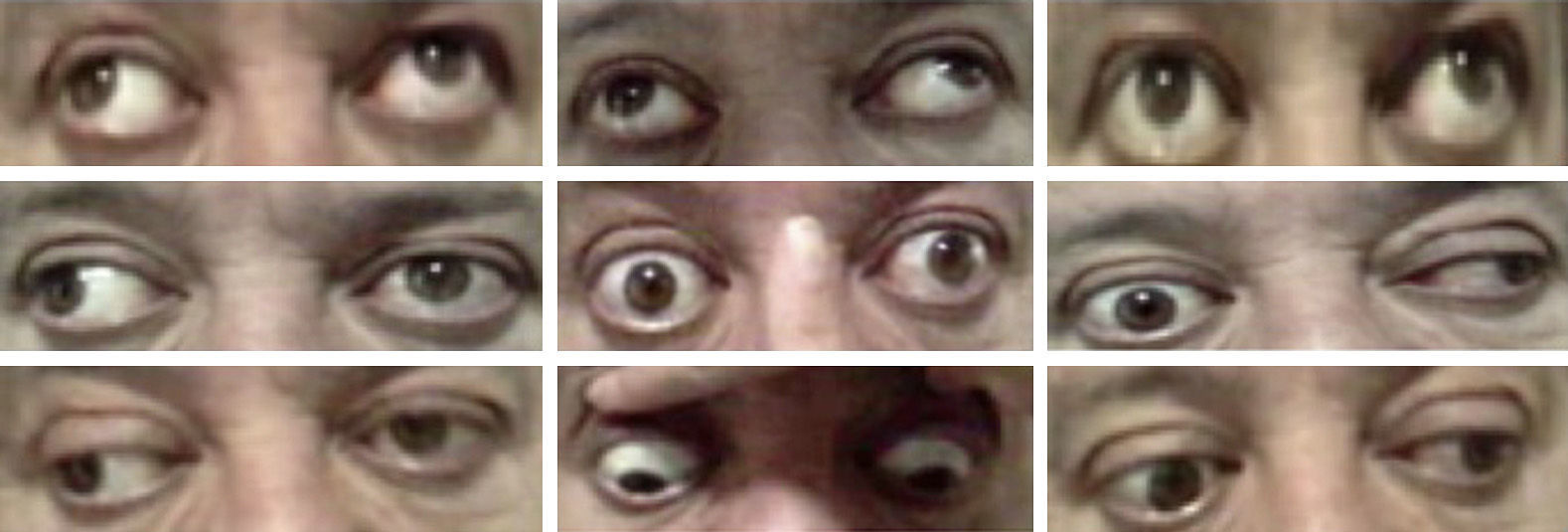
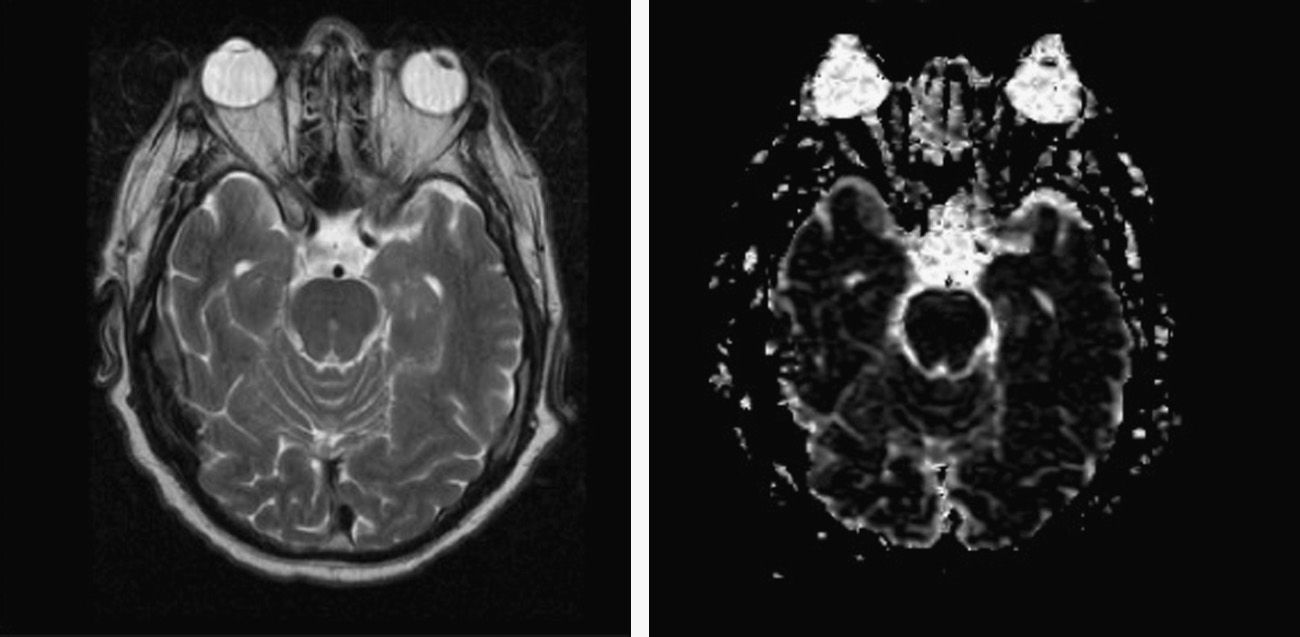
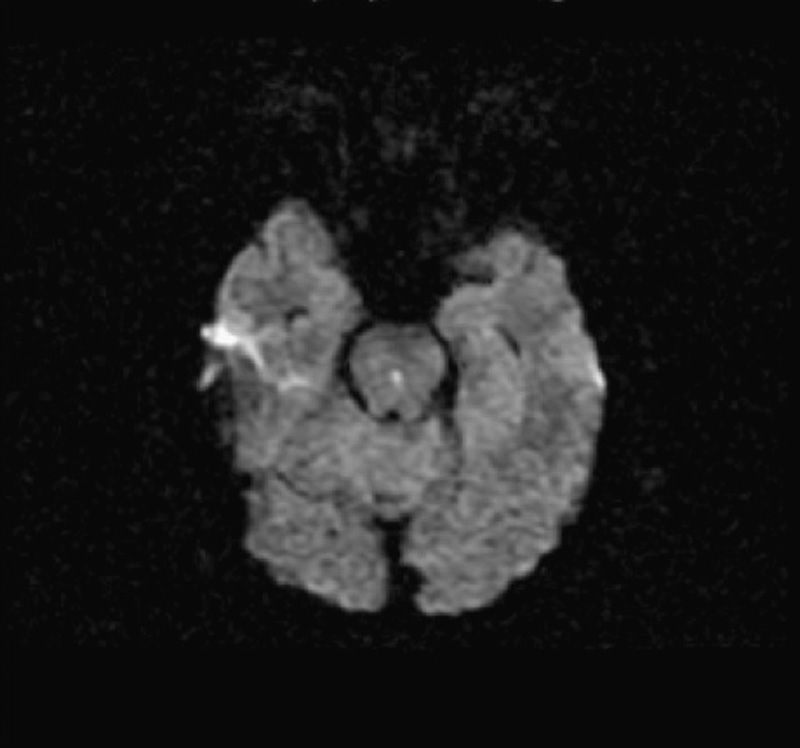
The patient is a 57-year-old obese and hypertensive male. His chief complaints were double vision and dizziness, with mild exodeviation in both eyes in primary gaze position in the ocular motility examination, but more predominant in the left eye. The exotropia was noticeably more evident on the attempted upgaze. On horizontal gaze, the abducting eye deviated fully, but the adducting eye did not cross the midline. Nystagmus in the abducting eye and convergence impairment were found. Pupil size and testing were normal. Ataxia and areflexia were also present. Bilateral internuclear ophthalmoplegia was suspected and imaging and laboratory tests were performed. The CAT scan showed a right occipital hypo-attenuated lesion. In the MRI scan, a mesencephalic subacute ischemic lesion was found, involving the medial rectus subnuclei. Blood and cerebrospinal fluid test for syphilis were positive.
DiscussionBilateral internuclear ophthalmoplegia is a very uncommon–and difficult to diagnose–condition. In the reported case the lesion involved the medial rectus subnuclei. This fact could explain the exotropia in the primary gaze position, and supports that it is not possible to exclude the involvement of the medial rectus subnuclei in the webino syndrome. The rapid identification of the pathology contributed to the better prognosis of the patient.
Paciente varón de 57 años que refiere visión doble y mareo de aparición brusca. A la exploración oftalmológica se observó una exotropía evidente en posición primaria de la mirada, ausencia de aducción de ambos ojos, nistagmo en abducción e incapacidad para la convergencia. Ante la sospecha de oftalmoplejía internuclear (OIN) bilateral se realizan pruebas de imagen y de laboratorio. La RMN craneal objetiva una lesión isquémica subaguda en el centro del mesencéfalo, afectando a los núcleos motores oculares comunes. Las pruebas para sífilis fueron positivas en sangre y líquido cefalorraquídeo.
DiscusiónEl síndrome de webino es muy infrecuente y de difícil diagnóstico. En el caso presentado, la lesión se encuentra perfectamente localizada en la zona media de la protuberancia, afectando a los núcleos motores oculares comunes. La rápida derivación del paciente y el establecimiento de tratamiento con penicilina posibilitaron la mejoría del cuadro.

