






To explain using a structural equation model to patient satisfaction by analysing confidence in preventive measures against COVID-19 as an antecedent of this satisfaction and the effect that these measures have on the antecedents of service quality and perceived value.
DesignAn observational cross-sectional study.
SiteOnline survey was sent via social networks for recruiting citizens resident in Spain.
ParticipantsThe final sample consisted of 149 women and 122 men. The mean age of the participants was 36.73 years, all of whom were health service users.
InterventionsNo interventions were conducted in the study.
Main measurementsThe study variables for the development of the structural equation model were: confidence in COVID-19 safety protocol, perceived value, quality and user satisfaction.
ResultsThe results showed a direct and positive effect of confidence in COVID-19 safety protocol on the quality of services provided, perceived value and user satisfaction.
ConclusionsThe study is expected to be of interest to those in charge of designing protective measures against the spread of diseases, health centre managers and marketing professionals interested in the improvement user satisfaction, affected as a result of the current pandemic.
Explicar mediante un modelo de ecuaciones estructurales la satisfacción de los pacientes, analizando la confianza en las medidas preventivas contra la COVID-19 como antecedente de esta satisfacción y el efecto que estas medidas puedan tener en la calidad del servicio y en el valor percibido.
DiseñoEstudio observacional transversal.
EmplazamientoLa encuesta online se envió a través de las redes sociales para reclutar a ciudadanos residentes en España.
ParticipantesLa muestra final estuvo compuesta por 149 mujeres y 122 hombres. La edad media de los participantes fue de 36,73 años, todos usuarios de servicios sanitarios.
IntervencionesNo se realizaron intervenciones en el estudio.
Medidas principalesLas variables del estudio para el desarrollo del modelo de ecuaciones estructurales fueron: la confianza en el protocolo de seguridad COVID-19, el valor percibido, la calidad y la satisfacción del usuario.
ResultadosLos resultados muestran un efecto directo y positivo de la confianza en el protocolo de seguridad COVID-19, el valor percibido y la satisfacción de los usuarios.
ConclusionesSe espera que el estudio sea de interés para el personal encargado de formular medidas de protección frente a la propagación de enfermedades, responsables de centros sanitarios y profesionales del marketing interesados en mejorar la satisfacción del usuario en el ámbito sanitario, mermada a consecuencia de la actual pandemia que vivimos.
Governments must prioritise the health care provided to citizens. It is the state's obligation to continuously improve medical services, ensure health coverage for citizens and guarantee the safety of service provision. Since 14 March 2020, the day on which the Spanish Government declared a state of alarm, caused by the SARSCoV-2 infection (severe acute respiratory syndrome), which has led to the COVID-19 pandemic (coronavirus disease 2019), the Public Health System has experienced an overload of infected patients.1 Although the capacity of facilities to combat the virus has been increased, it has been impossible to stop the first three waves before the first vaccines or treatment became available.2,3 In addition, essential services and day-to-day activities need to continue to be provided as much as possible.4 As a consequence, care protocols have changed in all medical facilities.5 Preventive protective measures, initially non-existent or at best insufficient, have been included for healthcare workers and for other pathologies patients. The aim is always to reduce mortality and minimise the number of people affected.4
Among the measures implemented by the government to try to prevent the pandemic are: (a) obligatory use of masks, (b) limitation of accompanying persons to the health centre, (c) selective control and measurement of body temperature when entering health centres, (d) suspension of the guarantee of response time in health care processes, first consultations in specialised care and diagnostic procedures in the Public Health System, among others.
Through these measures, patient care coverage should be guaranteed, the risk of users attending health centres should be mitigated, and confidence in the Public Health System should be improved. However, the special characteristics of the health sector led to users being treated not as consumers, but as patients.6 In the current context, patients perceive a risk related to their personal health each time they attend medical facilities. Overcoming these risks and improving user safety can influence service quality, perceived value and ultimately patient satisfaction.
Confidence is a subjective belief, referring to the reduction of a future risk (the risk of contagion in this case) and the probability of continuing to use the service provided.7,8 This concept of trust applied to institutions is called institutional or organisational confidence.9 Institutional confidence will depend on the organisational response to compliance with current regulations; this response improves the consumer's expectations of the service10 and the trust generated. Therefore, it is logical to think that the subject, after evaluating the service provided by the institution, will increase or reduce trust in the organisation.8,11 In other words, patients will feel safe and trust their healthcare facility if they consider the safety measures in place to be trustworthy.
Research has shown that perceived confidence is a good predictor of quality.12,13 In addition, trust measures have also been found to contribute to improved perceived value.14 This relationship was demonstrated in the work of Konuck,15 who found that increased consumer confidence in the service provider can lead to an increase in perceived value of the marketed products.
In contexts such as healthcare, where relationship building becomes essential, it is possible that trust determines the quality of services and perceived value, i.e., confidence in services will be a combination of trust in the institution itself, trust in the staff working there and the technologies used by the organisation,16 in this case by the medical centre. The work of González,17 demonstrated this relationship between trust, service quality and user satisfaction by analysing the interactions between the client and the health services.
The result of evaluating patient perceptions is an important indicator of health care.18,19 Specifically, patient satisfaction is one of the most widely used measures in the field of health management to gauge the effectiveness of the medical care received.20,21 Many studies have examined the determinants of satisfaction, showing that different variables influence this satisfaction.22–24 Among others, previous literature suggests a relationship between quality and satisfaction.24,25
In this sense, consumer perceived experiential quality can be understood as the difference between expectations and performance.26 Specifically, quality is largely a performance concept based on consumer ratings of certain criteria.25 These evaluations of the various characteristics of a service allow the patient to rate its performance and can, in the same way, directly influence satisfaction.24
The pandemic caused by COVID-19 has led to a series of incidents in the medical services provided. According to Smith et al.,27 service delivery issues can derive from the process or the outcome. The process dimension is linked to how the service is received (e.g., incident caused by safety measures and protocols), while the outcome dimension involves what clients actually receive from the service (e.g., interruption of face-to-face medical service for a few months).28
The current healthcare environment has recovered its activity after the interruption caused by the pandemic. Medical centres have reestablished service, responding to the legal measures in place. The reestablishment of the service can reinforce customer satisfaction.29,30 Moreover, it is a strategic element that can increase customer satisfaction.30,31 According to the service recovery paradox, when an organisation satisfactorily solves the problem that prevented the development of the service, users seem to be more satisfied.29–32
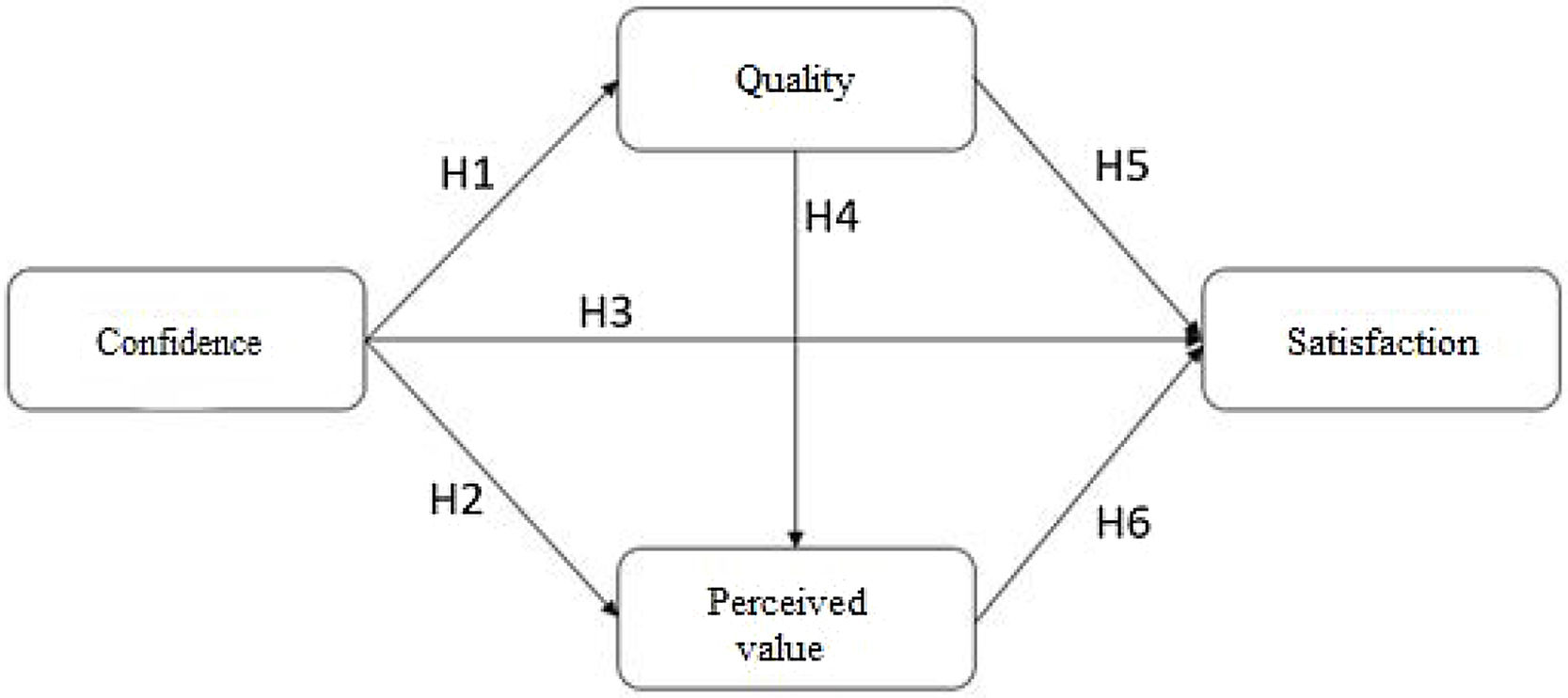
The aim of this paper is to model patient satisfaction by analysing confidence in COVID-19 preventive measures as an antecedent of patient satisfaction and the effect these measures have on the antecedents of service quality and perceived value. These relationships can be seen in the theoretical model proposed for this study (see Fig. 1). Based on this model, we propose the following hypothesis:H1 Confidence in COVID-19 prevention measures positively influences the quality of the health service. Confidence in COVID-19 prevention measures positively influences satisfaction with the health service. Confidence in COVID-19 prevention measures positively influences patient perceived value. The quality of the medical service positively influences the patient's perceived value. The quality of medical service positively influences patient satisfaction. The perceived value of the medical centre experience positively influences patient satisfaction.

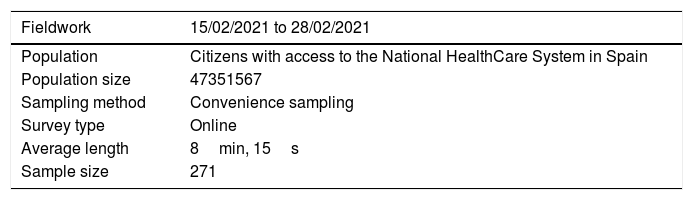
The research complied with the requirements established by the Bioethics Committee of the University of xxx (protocol code 189). This committee regulates the rights and freedoms of the participants, the right to privacy of their personal data and the aggregate treatment of the same. As for the methodological aspects applied, a quantitative method was used by means of an online survey (see Table 1). The questionnaire was designed following a review of the scientific literature on the subject under study, and was reviewed by members of the research team and by 3 experts in the health field. The Google Forms tool was used to draft the questions and collect the answers sent by a random selection of subjects who have either required face-to-face health services or have needed telephone assistance in the last year.
The survey was conducted online; participants accessed the questionnaire by invitation. The invitation to respond to the survey was disseminated through different social network groups. Given the great sensitivity of the population at this time with public health, an immediate response was obtained and a great social repercussion.
Participation was entirely voluntary. Fieldwork began on 15 February 2021 and ended on 28 February 2021. The initial database consisted of 282 surveys, and after refining the sample by applying a response time criterion, responses of less than 4min were eliminated. The final sample consisted of 149 female (55.2%) and 122 male (44.8%) participants. The mean age of the patients was 36.73 years. All from the same autonomous community. Of those surveyed, 90.4% used public health care, while 9.6% used private health care. The net monthly salary of the patients who use private health care is €2124.5 net, while the average salary of the participants who have public health care coverage is €1138.8 net per month. 3% go several times a month, 10.7% say they go at least once a month to the health centre, 37.6% go once every three months, 42.4% usually go twice a year, 6.3% go at least once a year. The main reasons for medical care were: medical check-ups (36%), emergency (30%), other causes (18%), common cold (9.5%), gastroenteritis or stomach problems (4%) and PCR test (2.5%).
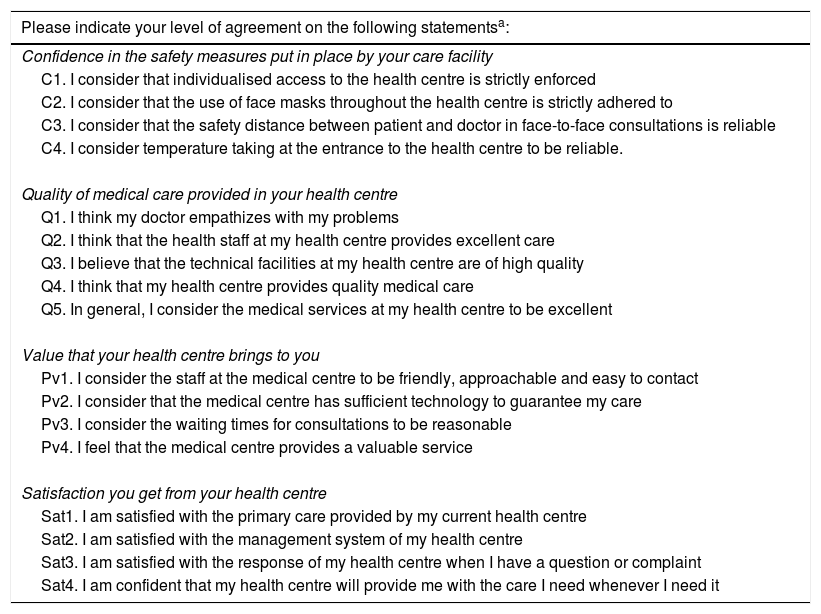
InstrumentsThe final questionnaire consisted of 36 items. All questions correspond to the conceptual theoretical model defined above, reflecting the hypothesised relationships. All items used Likert-type scales, with a graduation from 1 (minimum score) to 5 (maximum score). The constructs were measured using scales validated for the Spanish population. Perceived value was measured by adapting the Mitchell and Dacin33 and Thompson34 scale using 5 statements to assess familiarity and experience with the service. Satisfaction was assessed by adapting the 4 items from the work of Capraro et al.35 The scale of confidence with the service provider was adapted from Sirdeshmukh et al.,36 to the case of the COVID-19 protocol, using 4 items, related to the safety measures established in all health centres (individualised access, use of masks, distance from the health care provider and temperature taking).
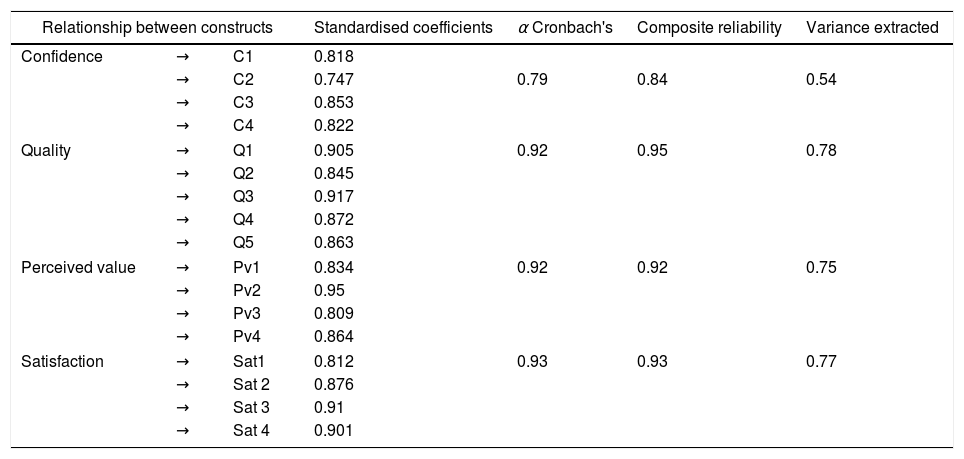
Data analysisA structural equation modelling (SEM) approach was used to examine the measurement and structural components of the model. The validity and reliability of the scales used in the study were previously tested (see Table 2) using SPSS V24 software. Data analysis was carried out following a two-stage procedure based on maximum likelihood.37 AMOS 20 was used to examine the structural model and test the research hypotheses.
Questionnaire used.
| Please indicate your level of agreement on the following statementsa: |
|---|
| Confidence in the safety measures put in place by your care facility |
| C1. I consider that individualised access to the health centre is strictly enforced |
| C2. I consider that the use of face masks throughout the health centre is strictly adhered to |
| C3. I consider that the safety distance between patient and doctor in face-to-face consultations is reliable |
| C4. I consider temperature taking at the entrance to the health centre to be reliable. |
| Quality of medical care provided in your health centre |
| Q1. I think my doctor empathizes with my problems |
| Q2. I think that the health staff at my health centre provides excellent care |
| Q3. I believe that the technical facilities at my health centre are of high quality |
| Q4. I think that my health centre provides quality medical care |
| Q5. In general, I consider the medical services at my health centre to be excellent |
| Value that your health centre brings to you |
| Pv1. I consider the staff at the medical centre to be friendly, approachable and easy to contact |
| Pv2. I consider that the medical centre has sufficient technology to guarantee my care |
| Pv3. I consider the waiting times for consultations to be reasonable |
| Pv4. I feel that the medical centre provides a valuable service |
| Satisfaction you get from your health centre |
| Sat1. I am satisfied with the primary care provided by my current health centre |
| Sat2. I am satisfied with the management system of my health centre |
| Sat3. I am satisfied with the response of my health centre when I have a question or complaint |
| Sat4. I am confident that my health centre will provide me with the care I need whenever I need it |
Confidence in the COVID-19 measures was considered as the only exogenous variable; quality, perceived value and satisfaction were considered as endogenous variables. This technique allows distinguishing between the measurement and structural model and takes into account measurement errors in the estimation of the model. Therefore, it is suitable for validating and testing causal relationships between constructs.38
Global model adjustmentsThe results in Tables 3 and 4 show the goodness-of-fit measures of the model of satisfaction with primary care at the health centre. The Normalised Chi-square (NSQ) values were between 1 and 5 (1.564), the Tucker-Lewis Index (TLI) was greater than 0.9 (0.981), the Bollen Incremental Fit Index (IFI) was also greater than 0.9 (0.984), the Root Mean Square Error of Approximation (RMSEA) is less than 0.05 (0.45). In addition, the Goodness-of-Fit Index (GFI) and the comparative fit index (CFI) exceed the recommended value 0.9.
Convergent validity and internal consistency analysis.
| Relationship between constructs | Standardised coefficients | α Cronbach's | Composite reliability | Variance extracted | ||
|---|---|---|---|---|---|---|
| Confidence | → | C1 | 0.818 | |||
| → | C2 | 0.747 | 0.79 | 0.84 | 0.54 | |
| → | C3 | 0.853 | ||||
| → | C4 | 0.822 | ||||
| Quality | → | Q1 | 0.905 | 0.92 | 0.95 | 0.78 |
| → | Q2 | 0.845 | ||||
| → | Q3 | 0.917 | ||||
| → | Q4 | 0.872 | ||||
| → | Q5 | 0.863 | ||||
| Perceived value | → | Pv1 | 0.834 | 0.92 | 0.92 | 0.75 |
| → | Pv2 | 0.95 | ||||
| → | Pv3 | 0.809 | ||||
| → | Pv4 | 0.864 | ||||
| Satisfaction | → | Sat1 | 0.812 | 0.93 | 0.93 | 0.77 |
| → | Sat 2 | 0.876 | ||||
| → | Sat 3 | 0.91 | ||||
| → | Sat 4 | 0.901 | ||||
Therefore, all indicators were found to exceed the values recommended by the literature,38 demonstrating that the model fit is efficient and reproduces the population variance-covariance matrix reasonably well.
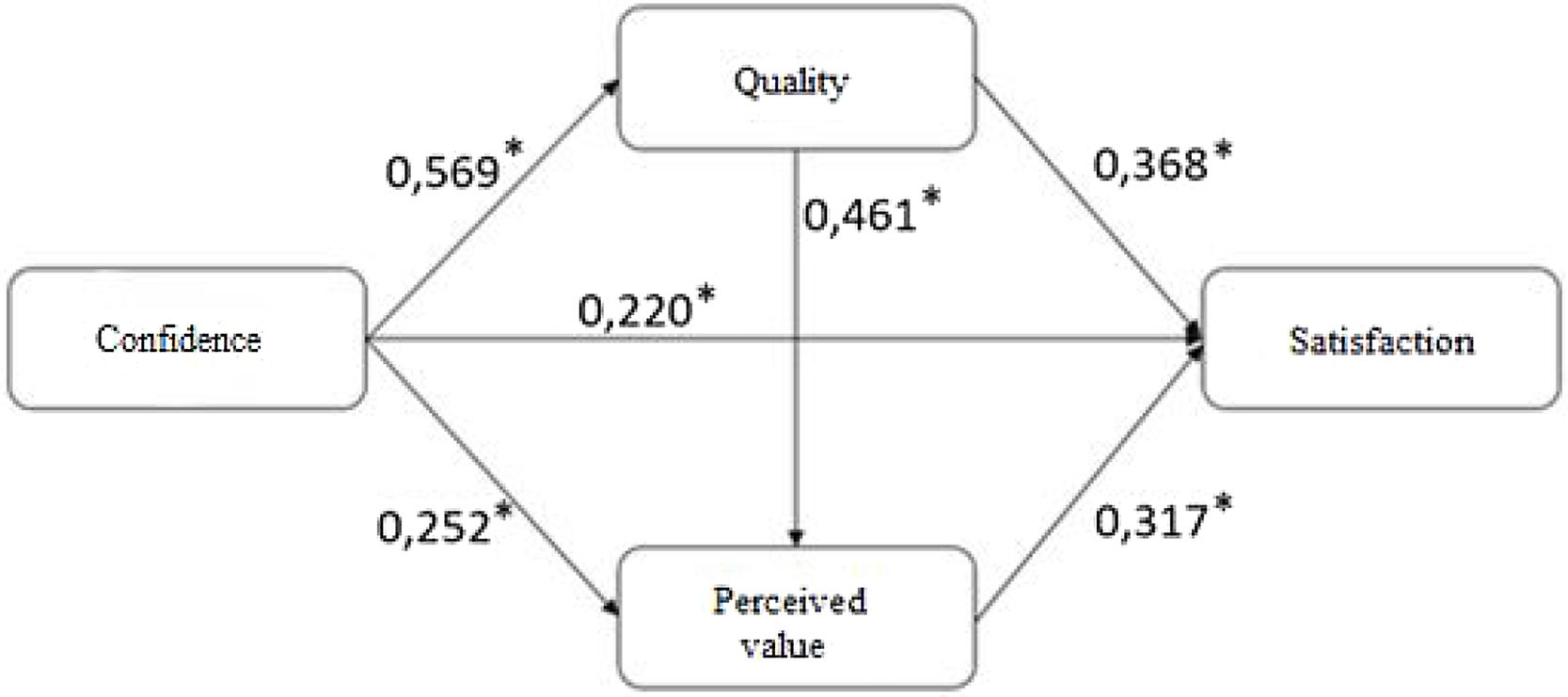
Hypothesis testingThis section analyses the statistical significance of the causal relationships proposed in the research hypotheses, reflected in the value of the standardised coefficients. The model of user satisfaction with the care received (see Fig. 2) made it possible to test all the hypotheses proposed.

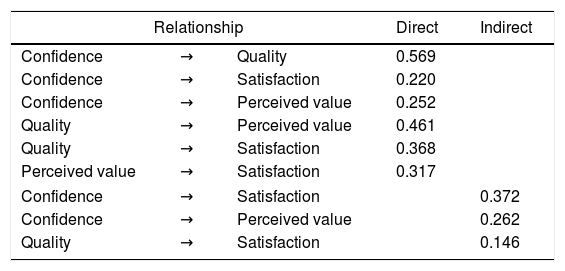
The model explained the 62.6% of the variance in patient satisfaction with the care received at the medical centre. The direct effects of the model made it possible to test all the research hypotheses. The impact of the antecedent variables reflects the influence of confidence in safety protocols and shows the impact on satisfaction through quality and perceived value. In addition, the indirect impact on satisfaction and perceived value through quality can be observed (see Table 5). The positive relationship between the confidence in safety protocols established in the health centres and quality was demonstrated, confirming the first research hypothesis (H1), with a significant standardised coefficient greater than 0.5 (β=0.569; p<0.001). Therefore, trust in safety protocols has been found to have a positive impact on perceived quality. Hypothesis H2, which proposes that the greater the confidence in the safety measures implemented to safeguard against COVID-19, the greater the perceived value in the health centre, was confirmed with a somewhat more moderate relationship between these variables (β=0.252; p<0.001), thus finding that the greater the confidence in the safety protocol in the medical centres, the greater the value perceived by the patient.
Total effects.
| Relationship | Direct | Indirect | ||
|---|---|---|---|---|
| Confidence | → | Quality | 0.569 | |
| Confidence | → | Satisfaction | 0.220 | |
| Confidence | → | Perceived value | 0.252 | |
| Quality | → | Perceived value | 0.461 | |
| Quality | → | Satisfaction | 0.368 | |
| Perceived value | → | Satisfaction | 0.317 | |
| Confidence | → | Satisfaction | 0.372 | |
| Confidence | → | Perceived value | 0.262 | |
| Quality | → | Satisfaction | 0.146 | |
The relationship posed by H3, between the COVID-19 safety protocol and patient satisfaction, is significant, although weaker than in the previous case (β=0.220; p<0.001). Thus, it was found that the greater the confidence in the safety measures established in the protocol for access, treatment or protection against COVID-19, the greater the users’ satisfaction with the health centre.
H4, which establishes a relationship between quality and perceived value, was confirmed, showing a positive and moderate influence on the relationship (β=0.461; p<0.001) as anticipated by previous literature. Thus, it was found that the higher the quality offered in terms of treatment, empathy, facilities or health centre staff, the higher the value perceived by the patient. The causal relationship proposed by H5 between quality and patient satisfaction was confirmed, establishing a moderate-weak relationship between the variables considered (β=0.368; p<0.001). Thus, it was found that the higher the quality offered by the health centre, the greater the satisfaction experienced by users of the health service.
Hypothesis H6, which proposes a causal relationship between perceived value and satisfaction, establishes a weak link between the two variables. The value obtained for the standardised coefficients was (β=0.317; p<0.001). We conclude that the more value the centre places on its patients, the greater the satisfaction with the care received.
DiscussionThe health crisis has led to a change in the way patients are treated, organised and cared for in public and private health centres. These changes in traditional healthcare patterns are affecting patient behaviour. Hence, there is a need for intervention from a management and marketing point of view to improve society's perception of current medical services.
To our knowledge, this research is the first to report on the impact of trust in safety protocol on user satisfaction with medical services. It is hoped that the study will be of interest to healthcare managers and marketers interested in improving service quality, perceived value and ultimately patient satisfaction, which has been diminished as a result of the current pandemic.
The results showed that the trust placed in protective measures has a direct benefit on the quality of the services provided. In line with the work of Moorman et al.,39 our work showed that the quality perceived by patients was affected by the trust placed by users in safety protocols.
It seems that the risk of contagion to which patients are exposed, make them value positively the health measures provided to safeguard personal health. Furthermore, confidence in these preventive measures seems to contribute to a higher perception of quality.40 Our work supports those investigations that consider trust as a necessary antecedent of quality in the user-provider relationship,41 in this case of medical services.
According to the work of Dehghanpouri et al.,42 the results achieved suggest that both trust and perceived quality can improve user satisfaction.
Our findings support those works that argue that quality and perceived value, anticipate user satisfaction.43,44 Consistent with Guenzi et al.45 we show that higher user trust can increase perceived value. Specifically, our results confirm those achieved in the work of Hu et al.,43 highlighting the mediating role of perceived value, in the perceived quality and satisfaction relationship. In contrast, the work of Wu et al.,44 who found when analyzing satisfaction with medical tourism that perceived quality anticipates trust and perceived value. Although the authors support that both variables are determinants of patient satisfaction, they found no relationship between them.
The results suggest that as confidence in the safety measures set out in the protocol for access, treatment or protection from COVID-19 increases, patients tend to be more satisfied with the care they receive. In line with the research of Thom, et al.,45 our work demonstrated that trust not only determines quality of care, but also directly impacts satisfaction.46,47 This research reinforces the literature indicating that the higher the patients’ trust in health services, the higher the satisfaction, given the existence of a positive causal relationship between both variables.48,49
The findings found in our work reinforce the findings of Wu et al.,44 who demonstrated that experiential quality determines perceived value. It appears that, improving the quality of the medical centre experience translates into higher levels of perceived value. Although previous literature argues for this causal relationship, in the context of healthcare management, few papers have studied the relationship between quality and perceived value.49
In addition to influencing value perception, our work supports those researches that link the quality of the healthcare experience, with satisfaction.50 Our data suggest that, increasing the quality of the healthcare experience, patient satisfaction can be improved. According to previous literature, service recovery per se, increases the perceived quality of the service offered and improves patient satisfaction.29,51
Evaluations of perceived value have demonstrated its influence on the satisfaction of health service users. Our work seems to indicate that, as patients perceive an increase in the value of the services provided, user satisfaction with the healthcare received increases. Different empirical works show that a higher perception of the value of the healthcare services offered increases the level of patient satisfaction.52,53
ConclusionThe main theoretical contributions worth mentioning in this research derive from the findings achieved. First, we demonstrate a relationship between trust in the new safety protocols established in health centres, medical service quality, perceived value and user satisfaction in this new health care setting. Secondly, an indirect effect of trust in safety measures was found through the perceived value of the healthcare consumer. Confirmation of this relationship may inform the design of marketing strategies aimed at improving user trust, which could lead to an improvement in perceived value and ultimately to greater patient satisfaction. Thirdly, to understand the mediating role (demonstrated through the indirect effects of the exogenous variable, confidence in the COVID-19 safety protocol) of the quality of the services offered by the medical centre on user satisfaction. This finding has important implications for management, as it also makes it possible to establish strategies aimed at patient confidence that can have an impact on the quality of service and, indirectly, on patient satisfaction. Fourth, the research supports the literature indicating the existence of a mediating effect between service quality and user satisfaction through perceived value. That is, we suggest that by improving service quality it is possible to improve perceived value and ultimately patient satisfaction indirectly.
LimitationsThis work, like many others, has some limitations. On the one hand, this study was carried out in a state of alarm and, therefore, some causal relationships could be questioned once the pandemic is over. Future studies could analyse these relationships over time to reaffirm the causality between variables. On the other hand, this research examines the recovery of health services in health centres, with the safety measures in place. However, the special characteristics of the medical services cannot be generalised to other research contexts, without certain nuances. Furthermore, the geographical scope of the empirical study, restricted to a region in southern Spain, also limits the generalizability of the results obtained.
Finally, although the institution requesting participation was indicated in the survey presentation, it is possible that many of the invited patients did not want to participate, either because of mistrust of the institution or because of dissatisfaction with the health care received at their health centre.
- •
There is a relationship between perceived quality and patient satisfaction.
- •
Confidence is a positive predictor of quality and perceived value of care.
- •
Satisfaction is one of the main measures of healthcare quality.
- •
Safety and quality measures are precursors of consumer satisfaction.
- •
Confidence in protection measures brings direct benefits in terms of the quality of services provided, perceived value and user satisfaction.
- •
Users positively value the minimisation of risk that compliance with them brings.
- •
The mediating role of service quality. The improvement of the elements that comprise it (screens, appointment dispensers), the reduction of response times to tests, the transmission of proximity, closeness and trust in the treatment, improves satisfaction.
- •
Marketing strategies aimed at improving user confidence will result in an improvement in perceived value and therefore in customer satisfaction.
This work has been carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki). At all times the participants were informed of their right not to participate or to leave the survey incomplete. The data of the participants were treated in accordance with the Law on Protection of Personal Data and guarantee of digital rights 3/2018.
FundingThis study does not have public or private funding.
Conflict of interestsThe authors declare that they have no conflicts of interest that may have influenced the research work carried out in this manuscript.
This study was supported by the University Institute of Research in Social Sustainable Development (INDESS).
