





Crossed renal ectopia is the second most common fusion anomaly after the horseshoe kidney, wherein both kidneys are present unilaterally, with the ureter of the crossed kidney opening into the bladder on the contralateral side. This condition can be associated with a number of complications. We present the case of a patient with abdominal aortic aneurysms, common bi-iliac and right external iliac aneurysms associated with crossed fused renal ectopia, which was managed with Chimney/snorkel endovascular aneurysm repair.
La ectopia renal cruzada es la segunda anomalía de fusión más común después del riñón en herradura, en la que ambos riñones están presentes de forma unilateral, con el uréter del riñón cruzado abriéndose en la vejiga del lado contralateral. Esta condición puede estar asociada a una serie de complicaciones. Presentamos el caso de un paciente con aneurismas de aorta abdominal, bi-ilíaca común e ilíaca externa derecha asociada a ectopia renal fusionada cruzada, que fue manejado con reparación endovascular de aneurisma tipo Chimney/Snorkel.
Crossed renal ectopia (C-RE) is the second most common fusion anomaly after the horseshoe kidney, wherein both kidneys are present unilaterally, with the ureter of the crossed kidney opening into the bladder on the contralateral side. The incidence of this entity ranges from 1:2000 to 1:7500 in autopsy series or 1 out of every 3078 computed tomographies (CT) scans.1 The crossed kidney is fused to the orthotopic kidney in more than 90% of the cases. It can be associated with a wide range of urological problems such as pelviureteric junction obstruction (PUJO), vesicoureteral reflux, ureteral strictures, and renal dysplasia.1 Chimney/snorkel endovascular aneurysm repair (ChEVAR) is a minimally invasive technique for the treatment of complex abdominal aneurysms. This endovascular approach is an alternative to fenestrated EVAR (FEVAR) for the treatment of juxtarenal and pararenal aortic aneurysms.2–4 In this report we present the case of a patient with abdominal aortic aneurysms (AAA), common bi-iliac and right external iliac aneurysms associated with crossed fused renal ectopia. The patient has agreed to the publication of images and details related to his case.
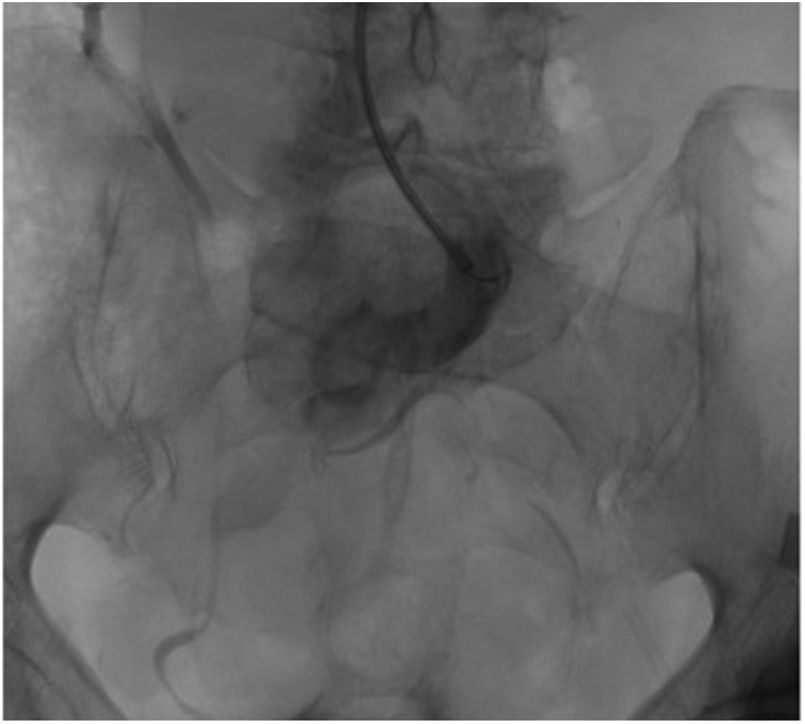
A 78-year-old man with several cardiovascular risk factors who was admitted for abdominal pain and was taken to surgery for cholecystitis performing laparoscopic cholecystectomy, aneurysms were documented incidentally. A review of computed tomography angiograms of the chest, abdomen, and pelvis on referral to our institution revealed a AAA associated with right crossed fused renal ectopia. Infrarenal abdominal aortic aneurysm with a diameter of 31mm in the bifurcation, right common iliac aneurysm with a diameter of 44mm, left common iliac aneurysm with a diameter of 31mm and a external iliac aneurysm with a diameter of 72mm. Double renal artery of the right crossed kidney in the AAA neck with a length of 65mm. The main right crossed renal artery had a diameter of 5mm and arose directly from the aneurysm neck (Fig. 1). Although open intervention using a transabdominal approach is a viable option for some patients with this pathology, the procedure has reported complication rates as high as 20%. After careful review of the patient's anatomy, comorbidities and the outcomes of the available treatment modalities, endovascular approach was deemed the better option given his lower postoperative complications and a short length of intensive care unit (ICU) and hospital stay due to the COVID-19 pandemic. The aneurysm was treated by a ChEVAR technique. The diameters of the aortic landing zone and the parallel graft were 25.5mm and 5mm, respectively. Therefore, we use a 28-mm stent graft (ETBF 28-13-145 Endurant; Medtronic, Minneapolis, Minn) with an oversizing of 10–20% based on the instruction for use of the aortic endograft and the favorable aortic neck of the aneurysm.

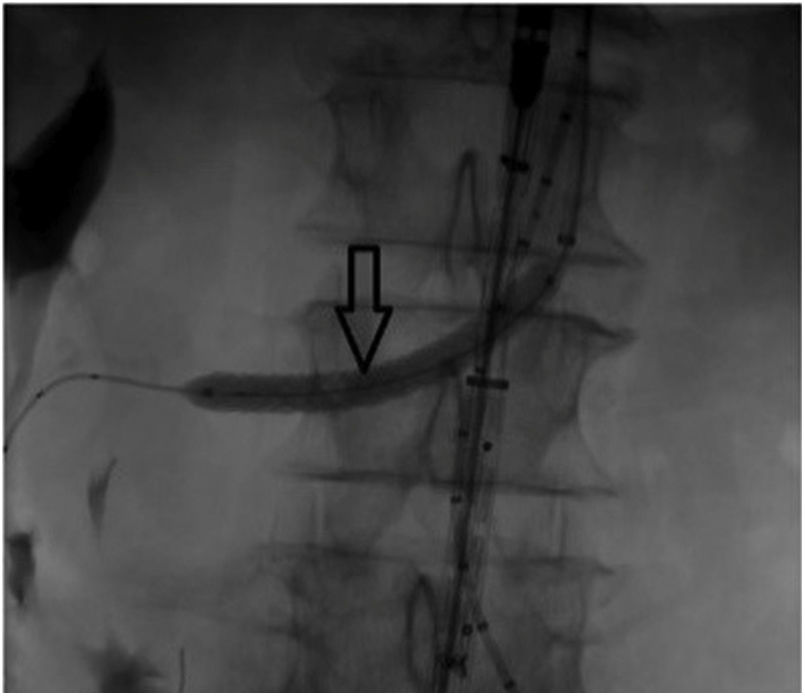
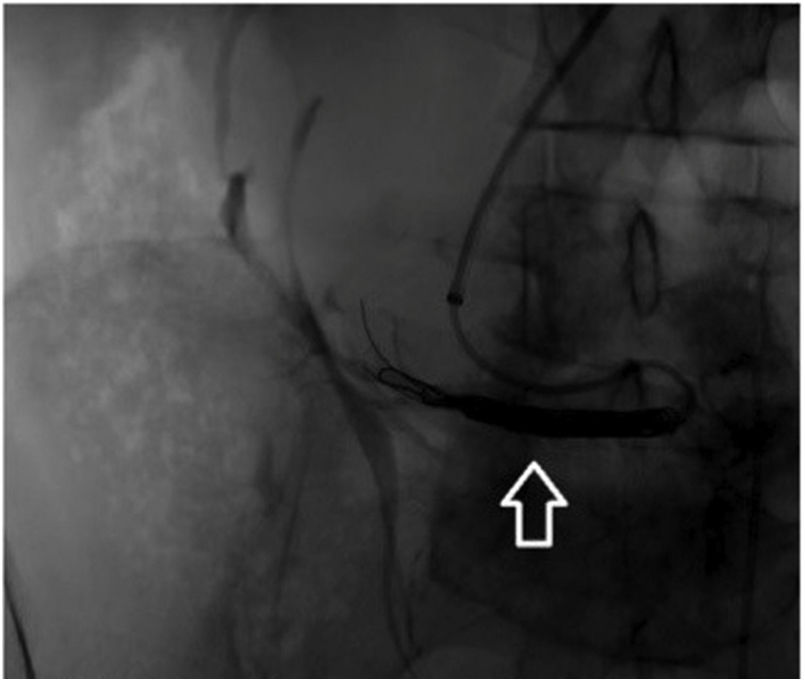
A percutaneous, ultrasound-guided, left brachial access allowed us to catheterize the crossed kidney artery with a Rosen guidewire (Cook Medical, Limerick, Ireland). A 6F Flexor sheath (Cook Medical) was then inserted in the ostium of the artery (Figs. 2 and 3). A percutaneous, ultrasound-guided, left and right femoral access were performed using two perclose Proglide suture-mediated closure system (Abbott Vascular, Clonmel, Tipperary, Ireland) to perform percutaneous arterial closure at the end of the procedure. The main body of the endoprosthesis (Endurant) was introduced through a left femoral access and then positioned undeployed in the abdominal aorta below the left renal artery. A balloon Expandable Endoprosthesis VBX stent graft (5mm×150mm; Gore Medical, Flagstaff, Ariz) was released in the main crossed right renal artery, and a balloon (5mm×150mm; Pacific [Medtronic]) was positioned inside the stent graft in order to avoid kinking or compression by the EVAR graft. The non-dominant right renal artery was embolized using 2 Coils (Concerto 20mm×40mm Medtronic, Minneapolis, Minn). The endograft's main body was deployed. We then performed a kissing balloon technique with the first balloon positioned inside of the Viabahn stent graft and a second balloon (Reliant AB46 [Medtronic]) positioned in the proximal end of the main body. The procedure was completed with deployment of the remainder of the aorto bi-iliac endograft. We reinforced the Viabahn stent graft with an E-Luminexx stent (6mm×120mm; BD Interventional, Tempe, Ariz) to avoid kinking of the parallel graft. The stent was eventually shaped with an identically sized balloon (6mm×120mm; Pacific;). Final angiography revealed patency of the Viabahn stent graft inside the crossed renal artery with normal vascularization of the renal parenchyma. No endoleaks were detected (Figs. 4–6). Renal function testing revealed no changes in serum creatinine concentration on days 1 and 3. Accordingly, the patient was discharged on day 3. Control angio TC was performed at one month postoperatively showing adequate correction of the aneurysms, with adequate renal prefusion of the orthotopic kidney and crossed kidney with patency of the stent chimney without evidence of endoleaks.


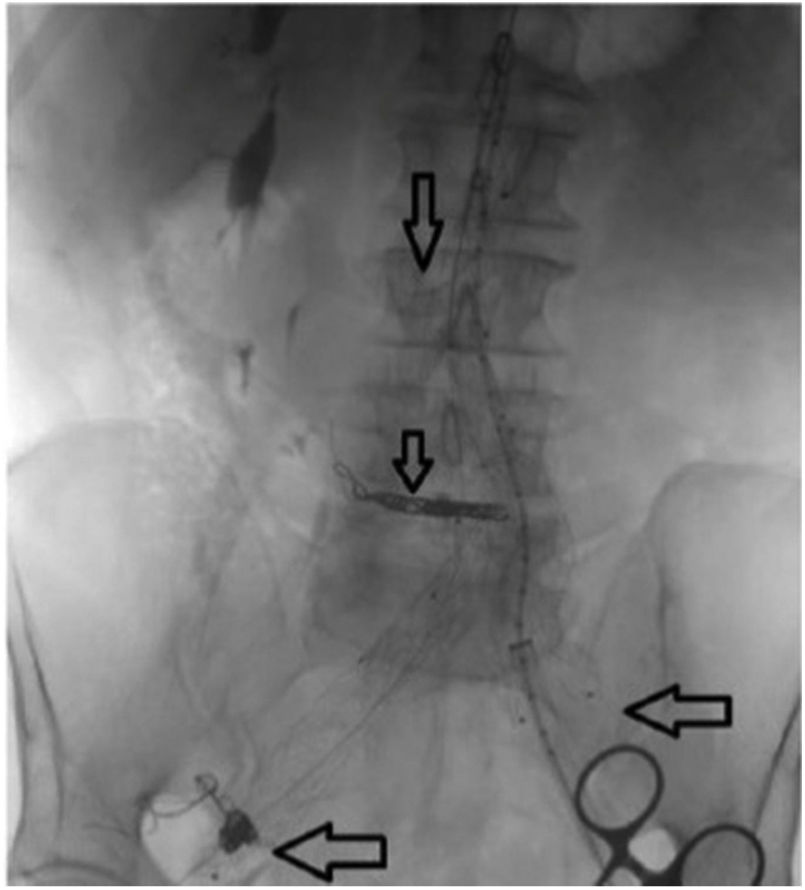
![Arrow, chimney. Viabahn stent graft (5mm×150mm; Gore Medical, Flagstaff, Ariz) was released in the main crossed right renal artery, and a balloon (5mm×150mm; Pacific [Medtronic]) was positioned inside the stent graft.](https://static.elsevier.es/multimedia/11340096/0000002900000005/v1_202209170528/S1134009622000547/v1_202209170528/en/main.assets/gr4.jpeg?xkr=ue/ImdikoIMrsJoerZ+w997EogCnBdOOD93cPFbanNc3bCucKqHBXNJDIEUXCwNL99MRCTsWR8l2VEc5tmSO8Ka7lXz8YrJaO1YYHrosFFWZXwNnEUYFyRdFtk/qN0zD2y1hAXn3XwWYsCzFNhFpPErJ/rT6RjWIMXFuvzi/MyDzI7/mMZV05CSJ1aqSngciDM4yXQMaBzDflMBLDGbtZb7Xf5xtWk6f0BRMJLjPxMIeZFz3JPudKnXTgd2aXYKH0rQMsBpQYf0oObPQOxUXZA8o1F4dWSuE63G1igR9NV4= "Arrow, chimney. Viabahn stent graft (5mm×150mm; Gore Medical, Flagstaff, Ariz) was released in the main crossed right renal artery, and a balloon (5mm×150mm; Pacific [Medtronic]) was positioned inside the stent graft.")
.")
, embolization of the lower renal pole (middle arrow), embolization of the right hypogastric artery (lower left arrow), correction of the left iliac aneurysm with bell bottom (lower right arrow).")
There are only two case reports about this specific type of patients treated with EVAR approach, one with ChEVAR and the other one with custom made FEVAR. The use of Ch-EVAR allowed the preservation of ectopic renal artery patency in a patient with high cardiopulmonary risk and it is a feasible and safe minimally invasive technique to treat this complex AAA anatomy cases.1–4 This brief case contributes to the current paucity of evidence on outcomes in the management of patients with abdominal aortic aneurysm associated with crossed fused renal ectopia, using the ChEVAR technique.
Ethical considerationsThe ethics committee of the Hospital Militar Central approved this case report. Constant of the use of medical data is obtained verbally and in written form from the patient.
Financial disclosuresNone.
Conflict of interestThe authors declare that they have no conflicts of interest.
None.

