


Bronchogenic cyst is a rare congenital malformation and commonly located in the mediastinum and lung parenchyma.
ObjectiveTo determine the clinical characteristics of the patients with diagnosis of bronchogenic cysts, their location and the infectious bacteria when the cysts are infected. The cases were collected from 1st January 2005 to 1st January 2013, in a third level hospital.
Material and methodsThe cases with bronchogenic cysts resected by thoracotomy were confirmed by histological study. Age, sex, admission diagnosis, location, size, imagenologic studies, and bacteriological cultures were evaluated.
ResultsOf the12 cases with diagnosis of bronchogenic cysts surgically resected by thoracotomy, six were male and six female, with 50% located in lung parenchyma and 50% in mediastinum, one of the latter was para-oesophageal. Bacteriological study of the cystic content demonstrated bacterial infection in seven (58%) cases.
ConclusionsBronchogenic cysts are rare congenital benign lesions. They must be resected because their content might be infected. The histopathology study is necessary to confirm the diagnosis, together with bacteriological examination. Thoracotomy is a safe procedure to resect bronchogenic cysts.
El quiste broncogénico es una malformación congénita benigna poco frecuente, se localiza principalmente en el mediastino y en el parénquima pulmonar.
ObjetivoDeterminar las características clínicas de los pacientes con diagnóstico de quiste broncogénico, su localización y las bacterias responsables en caso de presentar un proceso infeccioso, diagnosticados del 1 de enero de 2005 al 1 de enero de 2013, en un hospital de concentración de tercer nivel.
Material y métodosSe estudiaron los casos de quistes broncogénicos resecados por toracotomía que fueron confirmados por estudio histopatológico; se evaluaron: sexo, edad, diagnóstico de ingreso, localización, tamaño, cuadro clínico, estudios de imagen y cultivos bacteriológicos.
ResultadosSe encontraron 12 casos de pacientes con diagnóstico de quiste broncogénico resecados quirúrgicamente por toracotomía, 6 pacientes del género masculino y 6 del femenino; el 50% con localización pulmonar y el 50% en mediastino, de estos últimos uno fue paraesofágico. El estudio bacteriológico del contenido quístico demostró que el 58% de los casos tenía una infección agregada.
ConclusionesLos quistes broncogénicos son lesiones congénitas raras de naturaleza benigna, deben ser resecados porque su contenido puede infectarse. El estudio histopatológico es determinante para confirmar el diagnóstico conjuntamente con el examen bacteriológico. La toracotomía es un procedimiento seguro para resecar quistes broncogénicos.
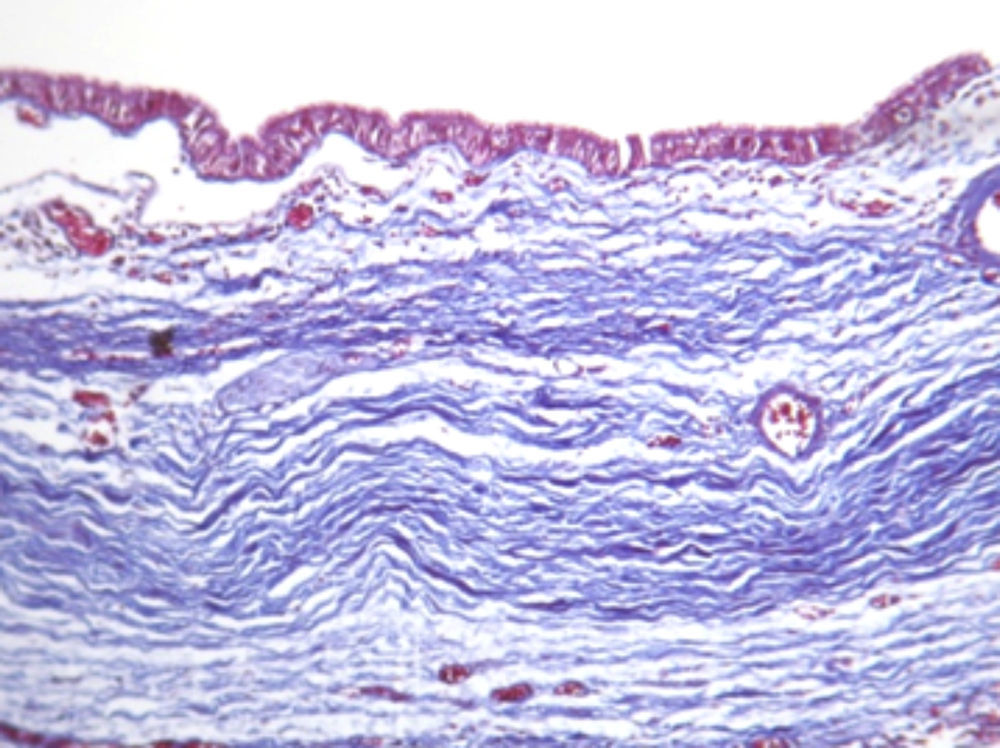
The bronchogenic cyst is a rare congenital malformation, the result of an abnormal budding of the tracheobronchial tree when separating from the primitive intestine, around the seventh week of gestation. This originates cystic lesions of variable sizes (in general of 1–15cm of diameter) mainly located in the mediastinum and the pulmonary parenchyma. The bronchogenic cyst may be filled with air or may contain a fluid with a milky appearance and of mucinous characteristics. The histology of the cyst wall reveals respiratory epithelium with mucous glands, cilia and, on occasions, bronchial cartilage. This characteristic histological pattern may disappear in the presence of an infectious process.1,2 Most of the patients are asymptomatic and the diagnosis is made by means of incidental findings when performing radiological routine tests.3 The bronchogenic cyst can appear as a cavitary formation of thin walls, occasionally accompanied by pleural effusion; it can also appear as a mediastinal mass that may be confused with a tumour.
In some cases the bronchogenic cysts become symptomatic when their content is infected, which produces purulent sputum that forces the patient to seek medical attention.
The objective of this research is to determine the clinical characteristics of the patients with the diagnosis of bronchogenic cyst, its location, the outcomes of the surgical treatment and to determine, in the infectious cases, which microorganisms were involved. The study was conducted in the Department of Pneumology of the General Hospital of Mexico O.D. (Decentralized Organism), a hospital concentrating on tertiary care.
Materials and methodsThe archives of the Pathology and Pneumology units of the Hospital General de México were reviewed from 1st January 2005 to 1st January 2013. The cases of resection of the confirmed bronchogenic cyst by histopathological study were selected. In all the cases, gender, age, diagnosis at admission, location, size, clinical condition, imaging studies and the results of the bacteriological cultures of the lesion content were evaluated. The value of the pulse oximetry was considered as information about the preoperative, intraoperative and postoperative functional state.
ResultsTwelve cases of patients with diagnosis of bronchogenic cyst surgically resected by means of thoracotomy were found. All of them were documented with imaging studies (chest X-rays, chest computed axial tomography) that showed the presence of a cystic cavity of thin walls and, on occasions, hydro-aerial levels. The average size of the lesions was 5.3cm. In all the cases a histopathological study of the bronchial cyst wall was performed, which showed a pseudo-stratified and cubic ciliated epithelium, with a discreet oedema of the submucosa (120X PAS staining) (Fig. 1).
Six male patients and six female patients were found with an average age of 49, ranging from 22 to 77. Six cases with pulmonary location (Table 1) and six located in the mediastinum (Figs. 1 and 2). One of the mediastinal cysts was para-oesophageal cyst. In 91% of the cases, the diagnosis of bronchogenic cyst was not considered at admission. In this series, 33% (4 cases) presented asymptomatic evolution, 66% (8 cases) of the patients presented cough (80%), dyspnoea (80%), purulent sputum (60%), fever (40%), asthenia and adynamia (30%), sensation of retrosternal pressure (20%), one patient presented haemoptysis (quantified in 200ml in 24h) that stopped spontaneously (Figs. 2 and 3a,bFig. 3).
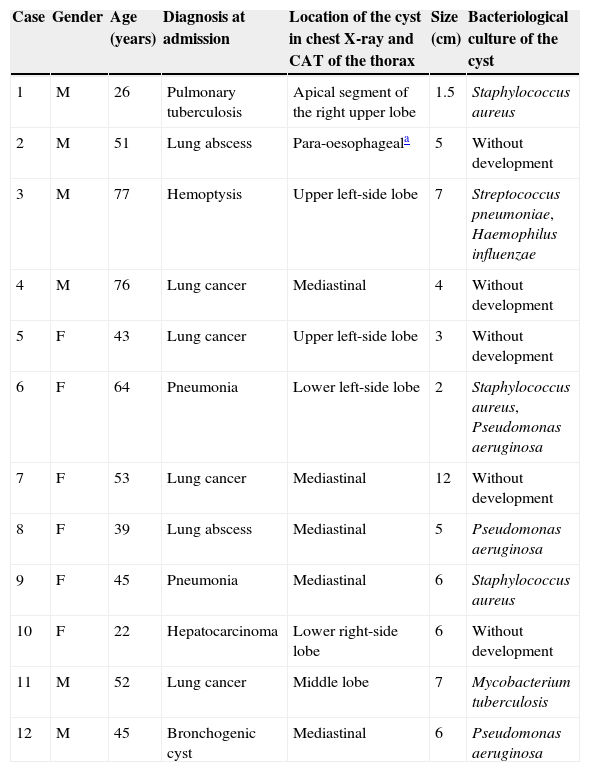
Bronchogenic cysts. Major findings.
| Case | Gender | Age (years) | Diagnosis at admission | Location of the cyst in chest X-ray and CAT of the thorax | Size (cm) | Bacteriological culture of the cyst |
|---|---|---|---|---|---|---|
| 1 | M | 26 | Pulmonary tuberculosis | Apical segment of the right upper lobe | 1.5 | Staphylococcus aureus |
| 2 | M | 51 | Lung abscess | Para-oesophageala | 5 | Without development |
| 3 | M | 77 | Hemoptysis | Upper left-side lobe | 7 | Streptococcus pneumoniae, Haemophilus influenzae |
| 4 | M | 76 | Lung cancer | Mediastinal | 4 | Without development |
| 5 | F | 43 | Lung cancer | Upper left-side lobe | 3 | Without development |
| 6 | F | 64 | Pneumonia | Lower left-side lobe | 2 | Staphylococcus aureus, Pseudomonas aeruginosa |
| 7 | F | 53 | Lung cancer | Mediastinal | 12 | Without development |
| 8 | F | 39 | Lung abscess | Mediastinal | 5 | Pseudomonas aeruginosa |
| 9 | F | 45 | Pneumonia | Mediastinal | 6 | Staphylococcus aureus |
| 10 | F | 22 | Hepatocarcinoma | Lower right-side lobe | 6 | Without development |
| 11 | M | 52 | Lung cancer | Middle lobe | 7 | Mycobacterium tuberculosis |
| 12 | M | 45 | Bronchogenic cyst | Mediastinal | 6 | Pseudomonas aeruginosa |
CAT scan, computed axial tomography scan.

.")
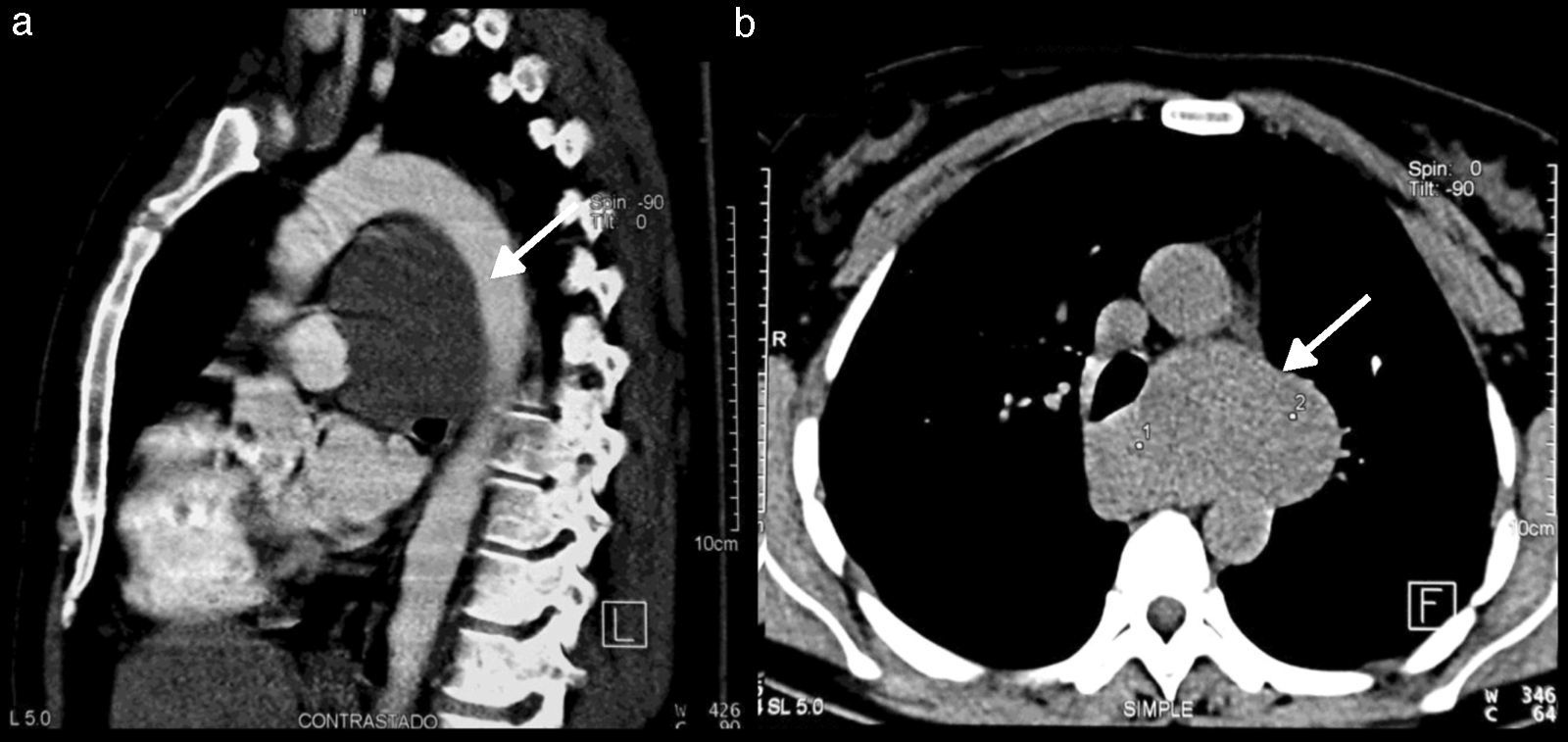
 Sagittal computed tomography; there is a well-defined mass of homogeneous opacity in front of the aortic arch and the ascending aorta (arrow). (b) Computed axial tomography. The mediastinal mass is projected towards the left, in front of the spinal column, between the ascending and the descending aorta (arrow).")
Case 7. (a) Sagittal computed tomography; there is a well-defined mass of homogeneous opacity in front of the aortic arch and the ascending aorta (arrow). (b) Computed axial tomography. The mediastinal mass is projected towards the left, in front of the spinal column, between the ascending and the descending aorta (arrow).
Overall, 58% of the cases had an additional infection developing in the cultures (Pseudomonas aeruginosa, Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae) and in one patient, with diabetes mellitus type 2, the culture in Löwestein–Jensen medium was positive for Mycobacterium tuberculosis (Fig. 4a,b). All the patients received specific antimicrobial treatment with a favourable response (Table 1).
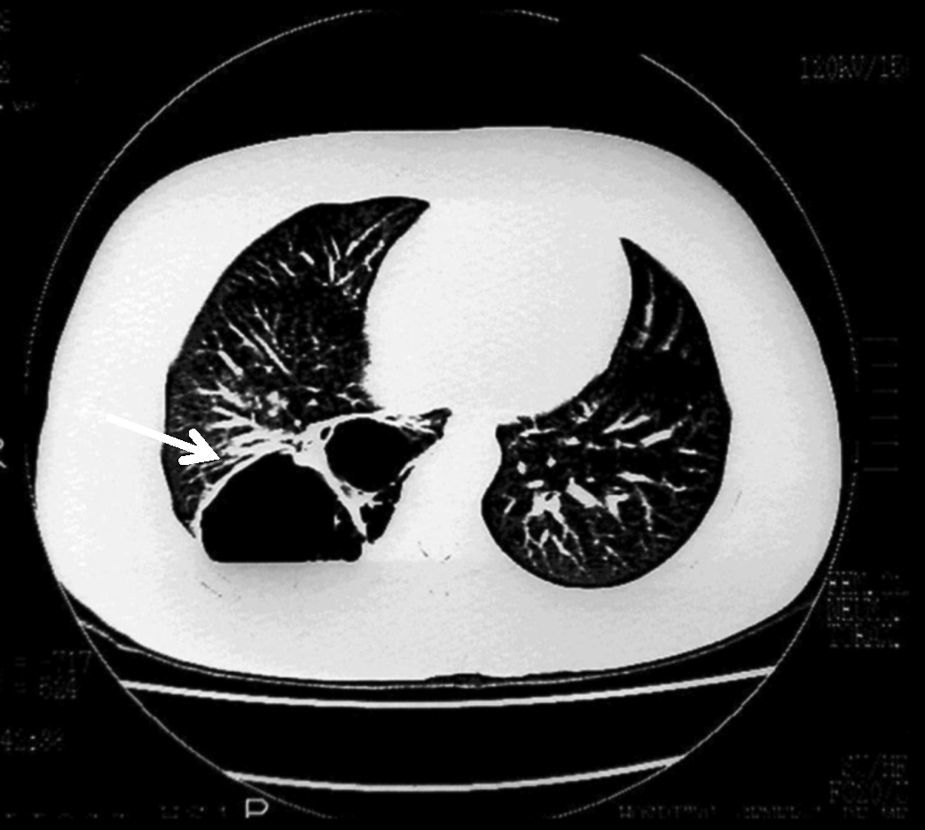
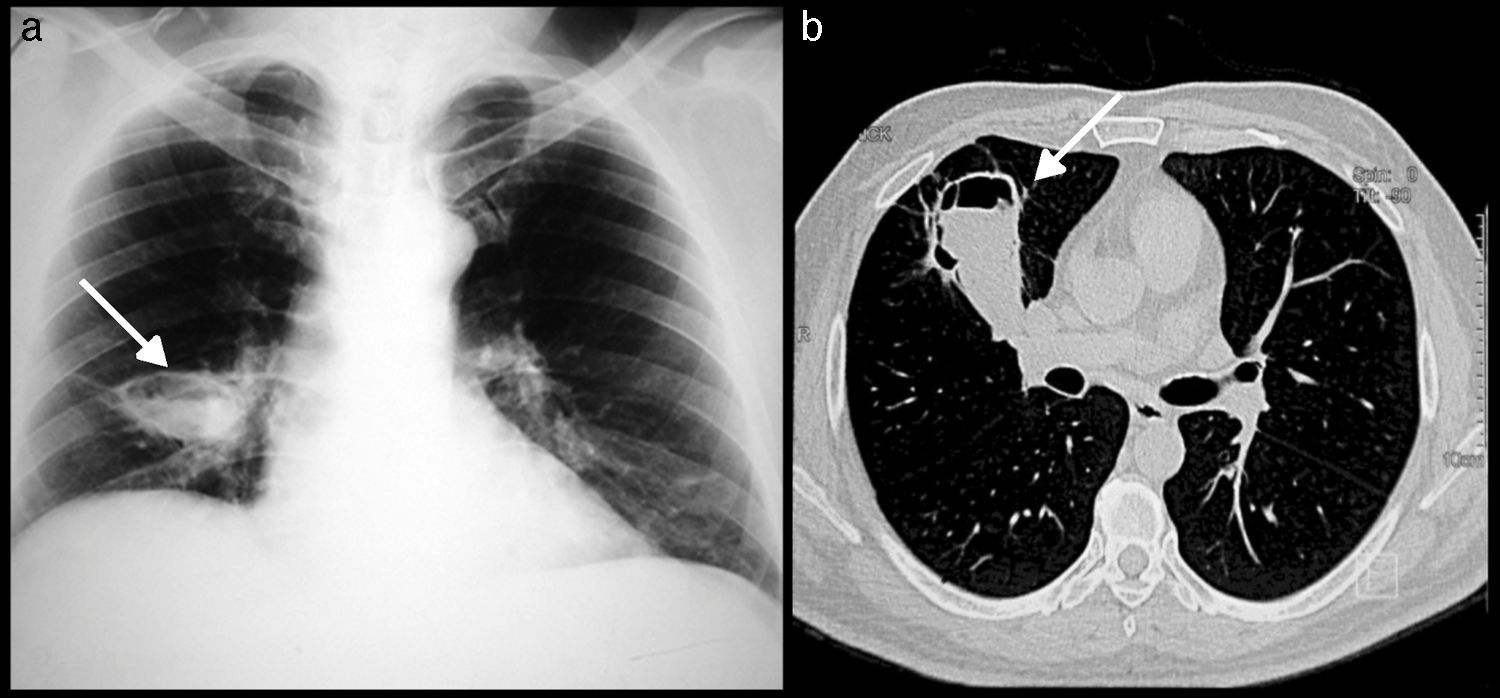
 Chest X-ray shows a cavity of thin walls with hydroaerial level (arrow). (b) Computed axial tomography shows an irregular cyst image with hydroaerial level in the middle lobe retracted to the front (arrow); Mycobacterium tuberculosis was isolated.")
After an average follow up of 16 months no cases presented recurrence after surgical intervention and all patients remained asymptomatic.
DiscussionGram-negative and gram-positive bacterial infection of the bronchogenic cysts is relatively frequent, provoking purulent sputum in the majority of cases. In the medical bibliography consulted, isolated cases affected by mycobacteria were found. In this series, a cyst infected with Mycobacterium tuberculosis was found in a patient with diabetes mellitus type 2, poorly controlled and with a long evolution.4–6 Cases like this may be diagnosed by the presence of granulomas with the characteristic histological image of the tuberculous microbacterias,7 also found in the non-tuberculous microbacterias (atypical).8 When cultures are not developed and a diagnosis of tuberculosis is suspected, the use of molecular biology techniques, such as the polymerase chain reaction in real time, are indicated.9 It is also important to rule out the presence of recurrent pulmonary abscesses that may be confused with infected bronchogenic cysts,10,11 particularly when there are doubts about the imaging test results.12 The computed axial tomography is generally a study with high sensitivity; nevertheless, the histopathology is essential to confirm the diagnosis. Bronchogenic cysts have bronchial epithelium, mucous glands and cartilage in their walls. This pattern may occasionally be lost if there is a chronic infection.13–15
Cysts may coincide with heart conditions such as pericardial defect and atrial fibrilation16,17; others have major adherences to the oesophagus, pericardium and pleura, which prevents the complete resection of them. The marsupialisation of the oesophagus may be a solution, as shown in one of the presented cases. The identification of the infectious microorganisms is important to establish the adequate antimicrobial treatment together with the cyst drainage, which will facilitate the cyst resection.18 The selective drainage of the infected cysts may occasionally determine the cure by means of ultrasound-guided aspirations.19 Cyst resection at open thoracotomy is still a safe procedure; thoracoscopy20 and video-assisted surgery are also very useful procedures in these cases.21
ConclusionThe bronchogenic cysts are rare congenital benign lesions that are generally not considered at diagnosis probably because the frequency of the incidence is very low. Cysts must be resected because their content may get infected. The histopathological study and the bacteriological test are decisive to confirm the final diagnosis. In this series, seven cases with five different bacteria and one with M. tuberculosis were found.
Conflict of interestThe authors declare that there are no conflicts of interest.
The authors thank the academic technician Marco E. Gudiño-Zayas, from Universidad Nacional Autónoma de México, for his help in the reproduction of the figures.
Please cite this article as: Hernández-Solís A, Cruz-Ortiz H, Gutiérrez-Díaz Ceballos ME, Cicero-Sabido R. Quistes broncogénicos. Importancia de la infección en adultos. Estudio de 12 casos. Cir Cir. 2015; 83: 112–116.