



Gallstone ileus is caused by the exit of a gallstone from the gallbladder or bile duct into the small intestine, resulting in bowel obstruction if this stone becomes lodged in a small bowel loop.
Clinical caseThe case is presented of a 78 year-old woman with an episode of intestinal obstruction. After studying the main cause of the obstruction, it was decided to perform a laparotomy where a gallstone located in the terminal ileum was causing the obstruction. No fistula was observed between the gallbladder and the bile duct and the intestinal tract. It is important to note the history of an endoscopic retrograde cholangiopancreatography performed a few months earlier, as it would probably be the cause of the passage of the gallstone to the small bowel.
ConclusionFew reports of gallstone ileus have been described in the literature after performing an endoscopic retrograde cholangiopancreatography. In these cases, the intestinal obstruction usually occurs several months after the endoscopic retrograde cholangiopancreatography, so the diagnosis is often delayed. Surgery is usually the definitive treatment and it consists of the removal the stone by enterotomy and performing a cholecystectomy. Biliary enteric fistula repair is not necessary since this does not form.
El íleo biliar está causado por la salida de un cálculo de la vesícula biliar o de la vía biliar al intestino delgado, produciendo un cuadro de obstrucción intestinal al quedar dicho cálculo enclavado, generalmente, en un asa de intestino delgado.
Caso clínicoMujer de 78 años de edad, que acude a urgencias por un cuadro de obstrucción intestinal. Tras el estudio de la posible causa, se decide realizar una laparotomía exploradora en la que se observó un cálculo biliar enclavado en el íleon terminal, que es el causante de la obstrucción; sin observarse fístula entre la vesícula o la vía biliar y el intestino. Como antecedentes tiene que unos meses previos al cuadro clínico se le realizó una colangiopancreatografía retrógrada endoscópica, y este se consideró como el origen del paso del cálculo al intestino delgado a través de la esfinterotomía realizada.
ConclusiónSon pocos los casos descritos cuya causa de un íleo biliar sea el antecedente de una colangiopancreatografía retrógrada endoscópica. En estos casos la obstrucción intestinal suele ocurrir meses después de la colangiopancreatografía, con lo que el diagnóstico suele retrasarse. El tratamiento definitivo suele ser la cirugía, que consiste en la extracción del cálculo mediante enterotomía, colecistectomía, y no se requiere la reparación de la fístula biliar, puesto que no se forma.
Gallstone ileus is caused by a stone exiting the gallbladder or the bile duct towards the small intestine, producing symptoms of intestinal obstruction when the stone becomes lodged, generally in a loop of the small bowel. According to Sivagnanam et al.1, it was first described by Erasmus Bartholin in 1654, but it was Leo Rigler in 1941 who described the triad of aerobilia, intestinal obstruction and gallstone impaction in the intestine. In order for a gallstone ileus to occur, there needs to be a fistula or communication between the gall bladder or the bile duct and a section of the small bowel. Obviously, aerobilia is not pathognomonic of gallstone ileus, since it most frequently occurs after endoscopic retrograde cholangiopancreatography and sphincterotomy. Gallstone ileus is most common in patients aged over 60–65 years of age, and generally occurs after cholecystitis or cholangitis, which causes a fistula between either of these 2 structures and the duodenum or small intestine. A stone passes through this fistula and causes intestinal obstruction.
There are few described cases of gallstone ileus where it has been observed that the gallstone passes through an endoscopic sphincterotomy, since this sphincterotomy is usually millimetres in diameter, as is the gallstone passing to the small bowel which is therefore generally expelled with no complications at all.
The aim is to report the clinical case of a woman who presented with gallstone ileus associated with a background of choledocolithiasis, resolved by endoscopic retrograde cholangiopancreatography months earlier. The patient had not undergone cholecystectomy.
Clinical caseA 78-year-old woman who attended the Emergency Department with a 24-hour history of abdominal pain, reporting nausea without vomiting and no alteration in intestinal transit. She had a relevant clinical history of surgical intervention 25 years earlier for a peptic ulcer for which she underwent subtotal gastrectomy, and 6 months earlier she had suffered an episode of cholecystitis and choledocolithiasis which was resolved by endoscopic retrograde cholangiopancreatography with the removal of several stones and endoscopic sphincterotomy. The patient subsequently refused cholecystectomy.
On initial assessment in the department, the patient was haemodynamically stable and afebrile, with a soft, palpable, diffusely tender abdomen, although more intensely tender in the right hypochondrium, with no signs of peritoneal irritation. She had attended the emergency department with symptoms of non-specific abdominal pain in the past 2 months, which were resolved with intravenous analgesia. There were no significant findings from the tests undertaken.
The laboratory results showed mild leukocytosis of 12,300mil/mm,3 with normal transaminase and amylase levels, and no other findings of note. Abdominal X-ray revealed a dilated small bowel loop, but with no air-fluid levels. It was decided that the patient should be admitted for observation, since her pain did not subside with prescribed analgesia.
An abdominal ultrasound was performed, described as: gallbladder with thin walls, with no content and a small band of perivesicular free fluid. The bile duct was at the upper limit of normal at 8mm in diameter.
The patient's clinical condition worsened and she started to vomit profusely, therefore it was decided to place a nasogastric tube which drained abundant bile content.
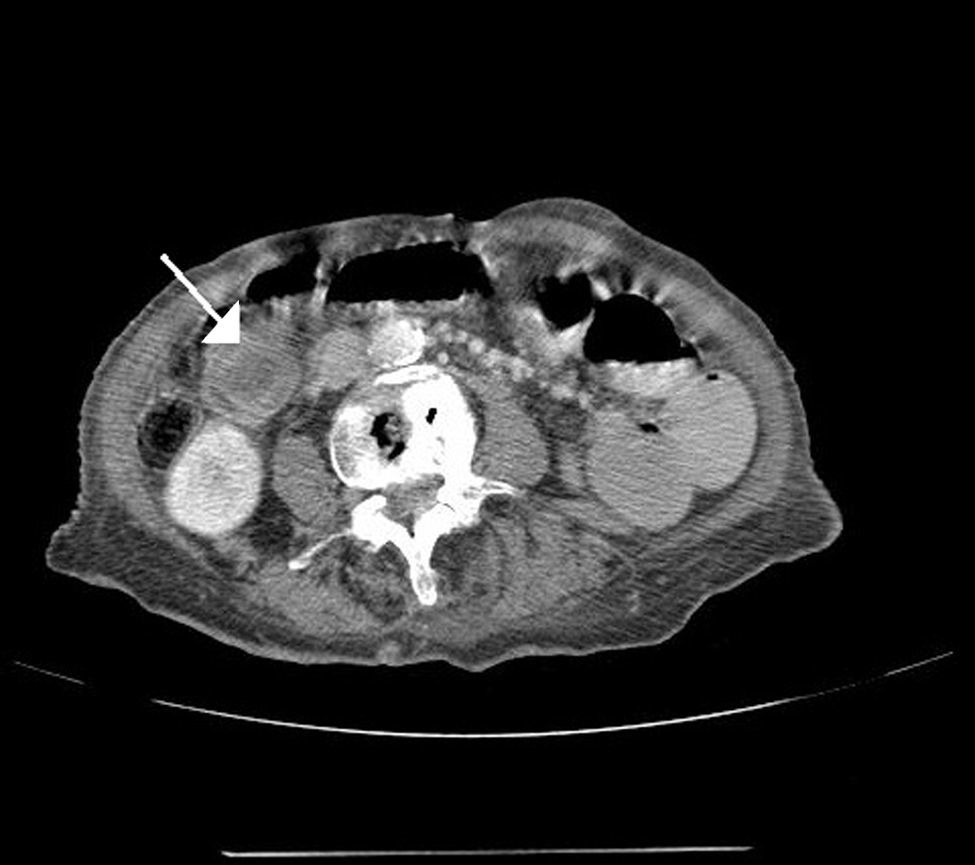
An abdominal CAT scan was ordered, which described aerobilia in the bile duct and the left intrahepatic duct, showing dilation of the small bowel loops up to a point in the right flank with doughnut morphology (approximately 3.5cm in diameter), with standard calibre of the distal loops (Fig. 1). Therefore, it was decided to perform emergency surgery, which revealed an intestinal obstruction caused by a stone of approximately 4cm (Fig. 2), with no cholecystojejunal fistula or choledocoduodenal fistula at any level. A simple cholecystectomy, enterotomy and removal of stone with primary closure of the small bowel was performed. The patient made good progress and was discharged from hospital 7 days after surgery.
 in the ileum with change of right intestine at that level.")

According to Goyal and Srivastava,2 the first person to draw attention to gallstone ileus was Erasmus Bartholin in 1654. The clinical picture is intestinal obstruction caused by impaction of a stone from the gallbladder or bile duct. It is the cause of between 1% and 3% of small bowel obstructions, but this increases to 25% in people aged over 65 years.2 The most common place for impaction of the stone is the distal ileum, followed by the jejunum and the stomach.
Gallstone ileus typically presents as intestinal obstruction. On this occasion, because the symptoms presented 6 months after a sphincterotomy, the suspected diagnosis was delayed and adherences or tumours were initially considered the most likely cause. The definitive diagnosis was only confirmed in the operating theatre.
In terms of imaging tests, occasionally plain abdominal X-ray, showing signs suggestive of an obstruction, along with the clinical symptoms is sufficient to indicate surgery in patients with no surgical history or palpable hernias. Diagnosis is confirmed by computed tomography of the abdomen and pelvis, which sometimes shows the impacted stone and sometimes, as in this patient, reveals an abrupt change in calibre at the level of the ileum, without showing the cause.
Definitive treatment is removal of the stone by enterotomy, with cholecystectomy and treatment of the fistula if there is one.
The most common complications of endoscopic retrograde cholangiopancreatography are: pancreatitis, cholangitis, haemorrhage or duodenal perforation. However, other less common complications have been described, as varied as: cardiovascular, pneumothorax, pneumomediastinum or gallstone ileus.
Gallstone ileus caused by a stone passing through an endoscopic sphincterotomy is extremely rare, less than 1% of complications, and some cases have been described in the literature.3,4 These are generally stones that measure on average 25mm, and that pass to the duodenum via a sphincterotomy, and probably remain in the small intestine without causing complete obstruction, but continue to increase in size until their diameter obstructs the intestinal lumen causing symptoms months later, which can delay definitive diagnosis.5–7
ConclusionsGallstone ileus had to be suspected with clinical signs suggestive of small bowel obstruction in a 60-year-old woman with a history of cholecystitis or cholangitis and endoscopic retrograde cholangiopancreatography and sphincterotomy, irrespective of the fact that this patient had undergone endoscopic retrograde cholangiopancreatography months before the onset of her symptoms.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
FundingThe authors have received no funding of any type to undertake this study.
Conflict of interestsThe authors have no conflicts of interest to declare.
Please cite this article as: Aláez-Chillarón AB, Moreno-Manso I, Martín-Vieira FJ, Mojtar MF, Pérez-Merino E. Íleo biliar posterior a colangiopancreatografía retrógrada endoscópica. Cir Cir. 2017;85:154–157.