



The standard of care for advanced-stage laryngeal cancer is combined treatment (chemo-radiotherapy). However, the complications with this treatment are not few, mainly in swallowing. Conservative laryngeal surgery remains an effective alternative for cancer control without the complications of chemo-radiotherapy.
Material and methodsRetrospective study was conducted on patients with laryngeal cancer cT3, cN0 with paraglottic infiltration, fixation of the vocal cord, minimal invasion of the hyo-thyroepiglottic space, but with normal arytenoid mobility and no sub-glottic extension, were treated with subtotal supracricoid laryngectomy. Complications, sequels of treatment, and local recurrence were evaluated. Bronchial aspiration was studied with radioactive swallow.
ResultsThere were 25 patients, 22 with negative surgical margins, one had tumour contact with the surgical margins, and 2 were positive. Two patients received postoperative radiotherapy. The mean decannulation was 15 days and removal of nasogastric tube 25 days. During the mean follow-up of 26 months, none of the patients had tumour recurrence or required conversion to total laryngectomy. In all patients swallowing has been normal and none required permanent or temporary tracheotomy or definitive gastrostomy. The voice is considered intelligible in all patients. Radioactive swallow showed aspiration in 15/25 patients, with none being clinically relevant. There were postoperative complications in 5 patients, and 4 patients required re-intervention but no conversion to total laryngectomy.
ConclusionConservative surgery is an effective surgical-alternative to chemo-radiotherapy in patients with locally advanced laryngeal cancer, providing oncological control, acceptable complications and minimal sequels. Although most patients have aspiration, this does not affect functional status.
El tratamiento estándar tipo conservador no quirúrgico del cáncer de laringe en etapa avanzada es combinado (quimio-radioterapia); sin embargo, las complicaciones que se presentan con este tratamiento no son pocas, principalmente para la deglución. La cirugía conservadora de laringe continúa siendo una alternativa eficaz para control oncológico sin las complicaciones que tiene la quimio-radioterapia.
Material y métodosEstudio retrospectivo, transversal, que incluyó a pacientes con cáncer laríngeo cT3, cN0 con infiltración paraglótica, fijación cordal pero movilidad aritenoidea normal, sin infiltración subglótica, fueron tratados con laringectomía subtotal supracricoidea. Se evaluaron complicaciones, secuelas del tratamiento y recurrencia. La aspiración bronquial fue estudiada con trago radiactivo.
ResultadosFueron 25 pacientes, en 22 los márgenes de sección fueron negativos; en uno los márgenes tuvieron contacto con tumor y en 2 fueron positivos. Dos pacientes recibieron radioterapia postoperatoria. La media de decanulación fue de 15 días y el retiro de sonda nasogástrica de 25 días. La media de seguimiento fue de 26 meses; ninguno ha presentado recurrencia tumoral ni conversión a laringectomía total. Todos con deglución normal y ninguno con traqueotomía permanente; la voz es considerada inteligible en todos. El trago radiactivo mostró aspiración en 15/25 pacientes, ninguno con repercusión clínica. Cinco pacientes tuvieron complicaciones postoperatorias, 4 requirieron reintervención pero ninguno conversión a laringectomía total.
ConclusiónLa cirugía conservadora es una alternativa eficaz con la asociación quimio-radioterapia, ofrece control oncológico, complicaciones aceptables y mínimas secuelas. Aunque la mayoría de los pacientes tienen aspiración, esta no repercute en el estado funcional.
Standard treatment aimed at non-surgical organ preservation of patients with locally and specially advanced stage epidermoid laryngeal cancer, who maintain laryngeal function, is combined chemo-radiotherapy1; cancer may be controlled with this treatment in over 50% of patients and preservation of laryngeal function is present in up to 93%2; however, toxicity is not insignificant, nor laryngeal oedema, laryngeal setting and pharyngo-laryngeal stenosis can make swallowing impossible, cause tracheo-bronchial aspiration or preservation of a non-functioning organ with the result that the patient requires artificial feeding (gastrostomy) and tracheostomy to prevent aspiration and subsequent pneumonia.
The aim of laryngeal preservation is to obtain cancer control with a satisfactory functional outcome, i.e. that the patient can breathe and swallow normally. Unfortunately, this goal is not always achieved in patients who are subjected to concomitant treatment.2,3 It has been shown that in patients who have been well selected, subtotal laryngectomy enables basic functions of the larynx to be preserved and the obtainment of a satisfactory cancer control, without the need to expose them to the possible risks of combined treatment. It is therefore essential to decide, prior to treatment, which of these patients may be indicated for combined treatment and which may benefit from conservative laryngeal surgery.4
Laryngeal preservation options are not limited to treatment with induction chemotherapy followed by radiotherapy or chemo-radiotherapy or initial combined treatment. Laryngeal preservation may also be surgical, with natural swallowing and breathing functions. To perform subtotal laryngectomy it is important to evaluate the determining factors to decide which is the best therapeutic alternative and whether the patient would be indicated for this procedure, depending on the patient's condition, tumour size (tumour volume, spread of tumour), the laryngeal function and the tumour sub-site.5
Conservative surgery has often been recommended as rescue treatment after radiotherapy used on the treatment of initial stage tumours has failed. At this time there may also be the possibility of complications and lack of success is greater. It does, however, play a major role in initial therapy of patients with locally advanced tumours and those where a high rate of complications is predicted on combining chemo with radiotherapy.5,6 Although there is not yet a sufficient level of evidence for us to decide which patient should be a candidate for surgery and which not, the function of the larynx at the time of diagnosis remains the best method of taking the decision on treatment.
The aim of this study was to discover the ontological and functional outcomes of subtotal laryngectomy with cricohyoidoepiglottopexy in patients with epidermoid laryngeal cancer who maintained a satisfactory laryngeal function (bilateral arytenoid movement and who were considered suitable for combined concomitant chemoradiotherapy treatment).
Material and methodsA retrospective, transversal study where outcomes obtained from patients who underwent subtotal supracricoid laryngectomy with cricohyoidoepiglottopexy reconstruction were analysed at the department of head and neck tumours of the Hospital de Oncología, in the Centro Médico Nacional Siglo XXI, of the Instituto Mexicano del Seguro Social. This took place between 1st January 2010 and 31st December 2011.
Patients diagnosed with stage cT3 epidermoid cancer of the larynx which had been confirmed by endoscopy and who were being treated consecutively were included in the study.
Classification testsDiagnosis was made using clinical, endoscopic and tomographic assessment completed in accordance with the histological classification with haematoxylin/eosin staining of biopsy specimens taken during direct laryngoscopy. Included in the study were those patients diagnosed with stage cT3 (AJCC 2010)7 epidermoid cancer of the larynx who had tomographic evidence of paraglottic infiltration, fixation of the vocal cord, absence of tumour mass in the pre-epiglottic space, absence of sub-glottic tumour infiltration and with normal bilateral arytenoid movement, which implies that although there has been major tumour spread, laryngeal function, characterised by arytenoid movement is still present, and the organ is thus functional.
They were clinically assessed prior to surgery with: fibre optic endoscopy, computed tomography of the larynx, respiratory and cardiovascular function tests. All patients were subjected to: functional respiratory tests, assessment of functional condition and nutritional assessment. Clinical data and surgical complications were also recorded. Mean follow-up was 26 months.
Confirmatory testsAll patients underwent subtotal supracricoid laryngectomy reconstructed with Piquet type cricohyoidoepiglottopexy8; when there was supraglottic infiltration (ventricle of Morgagni and/or ventricular band), modified radical division was performed on the neck of the side affected at levels II–IV. The procedure consisted of dividing the strap muscles at the hyoid bone insertion, at the foot of the epiglottis and clearing the thyroid cartilage, which includes both paraglottic spaces and both vocal cords up to their insertion with the arytenoid cartilages. The formation of the neo-larynx was performed by fixing the cricoids cartilage to the epiglottis, the hyoid bone and the base of the tongue with 3 separate stitches of Vicryl 1.
Surgical margins were considered positive when the tumour infiltrated the margin limit, in contact when it reached the section without infiltration and close when it was 1mm or less from the surgical margin.
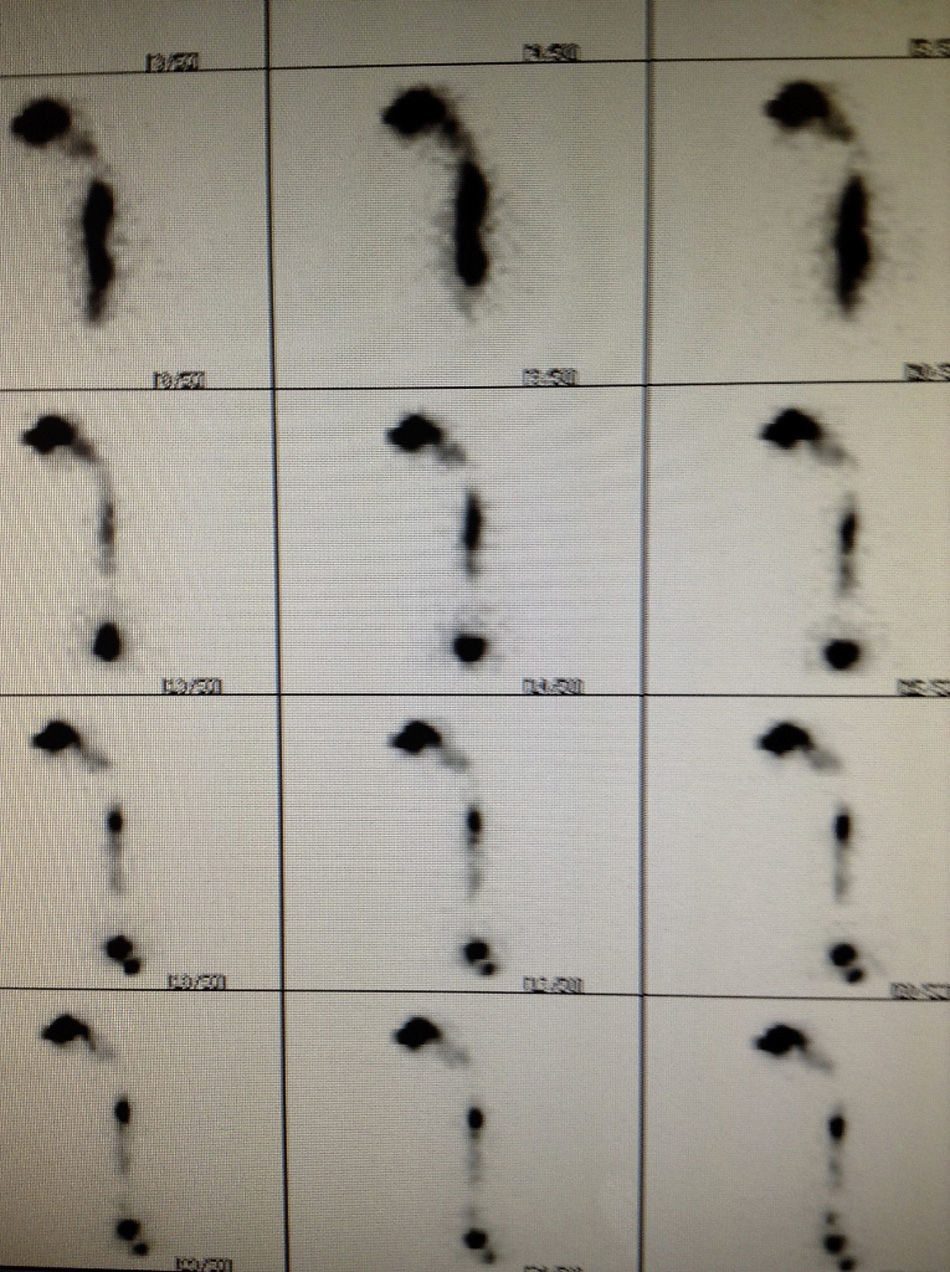
After decannulation and removal of nasogastiric line, all patients were assessed with Technetium 99 isotope and a gammagraphy was performed to discover the presence and possible magnitude of bronchial aspiration during swallowing (Fig. 1).
 with Tc99 which shows the absence of bronchial tree aspiration. The radiocolloid passes satisfactorily through the digestive tract with no presence of dye showing up in the bronchial tree.")
The surgical and non-surgical procedures and alternatives were explained in detail to all patients, and they signed informed consent documents. The project was reviewed and approved by the Ethics Committee.
Statistical analysisLocal control rates, tumour recurrence and laryngeal preservation function were calculated.
Descriptive statistics were used in statistical analysis in which the category variables are expressed in percentages.
ResultsDuring the study period 25 patients classified as cT3, cN0 glottics were treated, 23 men and 2 women, aged between 47 and 82 and a mean age of 62.9; they all presented with bilateral arytenoids mobility assessed with fibre optic at diagnosis. For all patients treated conservatively, functional condition was ECOG 0 and mean patient follow-up in this series was 26 months.
In 22 patients the surgery margins tested negative in the anatomopathological study, in 2 the margins tested positive and in one the margins were in contact with the tumour. There was no cartilaginous or extralaryngeal tumour spread in any patient, thus confirming stage pT3 in all of them. Six patients had supraglottic tumours (ventricular band) and underwent lateral neck dissection (levels II–IV); of these, only 2 (33%) had lymph node metastasis, both classified as pN1 without adverse prognostic factors (single metastasis without capsular invasion to soft tissues), both metastases were located at level III (middle jugular); the mean lymph nodes dissected were 25.
Two patients received post-operative radiotherapy, both with positive surgical margins.
Five patients (20%) had post-operative complications, the most frequent of which was bleeding; 2 of these patients had haematoma; 4 required further surgery for haemostasis and/or haematoma evacuation; 3 patients who had bleeding presented with infection of the surgical wound after surgery and received systemic antibiotic treatment; one patient presented with subcutaneous emphysema in the neck and in the upper third of the chest. This was resolved with conservative treatment. None of the patients’ complications necessitated cricohyoidoepiglottopexy reversal or conversion to total laryngectomy. Table 1 lists the complications.
Post-operative complications.
| Complication | Patients, n (%) | Surgical re-intervention (%) |
|---|---|---|
| Bleeding | 4 (16) | 4 (16) |
| Haematoma | 2 (8) | 2 (8) |
| Subcutaneous emphysema | 1 (4%) | – |
| Surgical wound infection | 3 (12) | – |
Post-operative complications in patients undergoing Piquet type cricohyoidepiglottopexy. Five patients presented with this the most frequent was post-operative bleeding (4); of them 2 had haematoma, 4 had to be re-operated on. Four patients with 2 or more complications.
The surgical wound infection and the subcutaneous emphysema were resolved conservatively. No patient needed conversion to total laryngectomy.
The mean decannulation was 15 days and the removal of the nasogastric tube 25 days. The patients’ voice was clinically assessed and patients were asked how they considered their voice to be, and the success they felt they gained when another person listened to them and/or during a telephone call. Assessment was made one month after decannulation.
The gammagraphy with radioactive swallow showed bronchial aspiration in 15 of the 25 patients (60%); none of them had clinical repercussions nor presented with areas of pneumonia on the chest CT scan.
None of the patients required conversion to total laryngectomy and all of them could swallow and breathe normally; none of them required final tracheotomy. Voice was considered intelligible in all patients, based on the previously described clinical assessment.
None of the patients presented with local or regional tumour recurrence.
Diet was similar to that patients had prior to treatment and none required reinsertion of nasogastric tube or temporary or definitive gastrostomy.
DiscussionLaryngeal preservation is, without a doubt, an advance in the treatment of epidermoid laryngeal cancer. Around 50% of patients who are indicated for total laryngectomy may preserve the organ with a non-surgical treatment which includes chemo and radiotherapy combined, or induction chemotherapy followed by only radiotherapy or chemo-radiotherapy. The ideal treatment pattern has yet to be defined.9
Notwithstanding, combined treatment is not without complications and sequelae which may condition the deterioration in quality of life. Several patients preserve the larynx but require gastrostomy or tracheotomy for feeding. This implies a non functional organ and approximately 33% of patients have serious bronchial aspiration and 26% require gastrostomy at some time of treatment, whilst 5% of them require it permanently.10 Several factors affect the clinical evolution of these patients and the most major are: tumour spread, the patient's general conditions and laryngeal function at diagnosis.9–11
Conservative treatment of the larynx has been suggested as an alternative in patients with locally advanced tumours, in which combined treatment is not considered ideal and where a better quality of life is the aim.12
In this series we presented 25 patients with locally advanced stages of cancer but who had maintained laryngeal function treated with conservative laryngectomy, with the technique described by Piquet.8 All of these patients were indicated for non surgical treatment with combined therapy and selection criteria was based on normal mobility of both arytenoid cartilages, where there was no mass paraglottic infiltration.
The mean removal of nasogastric tube and decannulation was 25 and 15 days respectively. Radioactive swallowing showed bronchial aspiration to several degrees in 60% of patients, but none of them had clinical consequences nor required conversion to total laryngectomy.
Laryngeal function was satisfactory in 25 patients and none required alternative methods of nutrition or final tracheotomy. Voice was considered normal in all of them and none required conversion. Although follow-up time was short, no patient presented with tumour recurrence.
Organ preservation in patients with advanced epidermoid cancer of the larynx may not be surgically associated with chemo or radiotherapy, but in selected patients for whom a poor response to this treatment is expected or there is potential danger of high toxicity, surgical preservation with subtotal laryngectomy is a suitable alternative, since a balance may be maintained between cancer control and a satisfactory quality of life.12,13
The parameters predicting treatment toxicity require further studies for analysis.10
The characteristics the Piquet type cricohyoidoepiglottopexy8 patients need to have in addition to the necessary indications of the technique,14,15 are appropriate arytenoid mobility, appropriate ECOG and permissible ventilation function results.
Conservative supracricoid subtotal type laryngectomy reconstructed by cricohyoidoepiglottopexy is an alternative to chemo-radiotherapy in patients with locally advanced epidermoid cancer, which offers appropriate control and allows for satisfactory laryngeal function, without exposing the patient to the risk and mobility which non surgical treatment involves; moreover, it enables both surgical and radiation rescue treatment with local recurrence, although in this series this did not occur (short follow-up period); probably its greatest disadvantage would be the need for temporary tracheotomy although in the present series, none of the patients needed a total laryngectomy, which would justify temporary loss of voice.
ConclusionsSupracricoid subtotal laryngectomy and the reconstruction of a “neo-larynx” with cricohyoidoepiglottopexy is a suitable alternative for the preservation of organs in locally advanced epidermoid cancers of the larynx, leading to satisfactory cancer control and a functional organ. The latter is defined as the absence of tracheotomy, normal swallowing without aspiration which in turn could lead to ventilation complications, and intelligible speech. It is therefore a valid therapeutic option in patients who for some reason are not suited to combined chemo-radiotherapy.
Conflict of interestsThe authors declare they have no conflict of interests.
Please cite this article as: Gallegos-Hernández JF, Cruz-Esquivel I, Ortiz-Maldonado AL, Minauro-Muñoz GG, Arias-Ceballos H, Pichardo-Romero P. Cirugía conservadora de laringe en pacientes candidatos a tratamiento combinado con quimio-radiación por cáncer laríngeo. Cir Cir. 2016;84:94–99.