


We read with great interest the article signed by Herrera-Fernández et al.1 published in your prestigious journal, and since we have had the opportunity to treat 2 patients with pancreatic pseudoaneurysm with diametrically opposing forms of presentation and resolution,2 we write to you to record our experience and put forward a series of considerations.
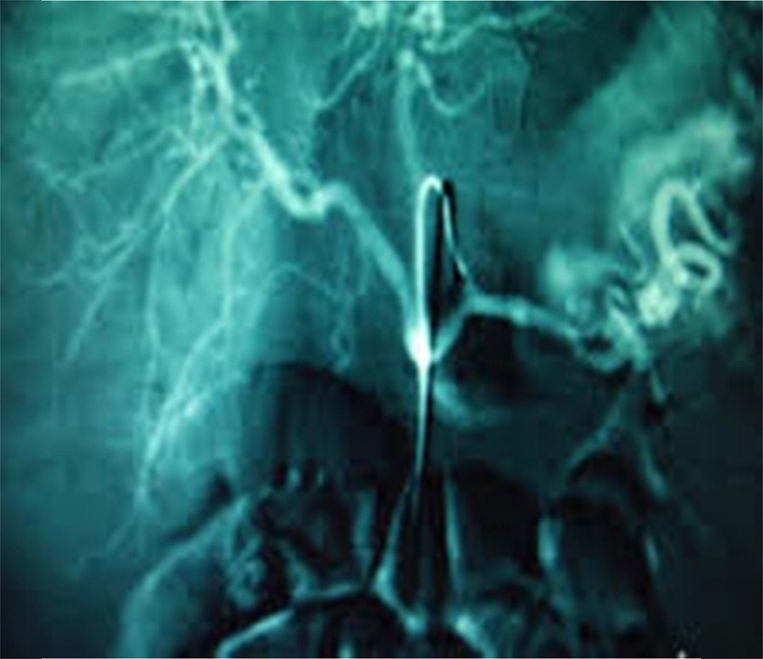
Our series covered the 2 most frequent forms of onset: the first being hypovolaemic shock due to vascular rupture (splenic artery), which can be diagnosed by mesenteric arteriography (Fig. 1), and the second being intense, recurring, and occasionally, shooting abdominal pain, discovered by means of computed axial angio-tomography scan (angio CAT).
, which can be diagnosed by mesenteric arteriography.")
We agree with the authors that this condition can be suspected if a patient presents with a history of alcoholic pancreatitis and severe, recurrent abdominal pain, and that the angio-CAT scan is the diagnostic tool of choice.
Although it used to be considered that the usual treatment was surgery, nowadays whenever possible, the therapy of choice is endovascular embolisation of the aneurysm via angiographic access, as our colleagues rightly note. This is effective in up to 80% of occasions, and surgery is reserved for when this technique cannot be undertaken due to the patient's haemodynamic instability or if the technique fails.3
Lastly, we wish to note that direct puncture and embolisation of the aneurysm via laparotomy have been described,4 as well as percutaneous puncture and intra-aneurysmal thrombin injection.5
Please cite this article as: Vázquez-Ruiz J, López-Flor V, Aguado-Pérez M, Fernández-Moreno J, Pérez-Folqués JE, Mansilla-Molina D. Seudoaneurismas pancreáticos: formas de presentación y opciones terapéuticas. Cir Cirí. 2015;83:454–455.