




Hibernomas are extremely rare benign tumors that arise from vestigial remnants of brown adipose tissue. Their characteristic color is due to the presence of numerous pleomorphic mitochondria and significant vascular irrigation.1 In adults, hibernomas are more common in men, with a maximum incidence in the third and fourth decades of life. Their function is thermoregulatory, and they are found more frequently in the central parts of the body, where brown adipocytes accumulate2: mediastinal, retroperitoneal, cervical, axillary and interscapular.3 In most cases, hibernomas present as asymptomatic masses. However, they may present as incidental findings on imaging tests, rarely causing symptoms related to the compression of adjacent structures.4 Unlike adipose tissue, brown fat contains abundant phospholipids and glycogen, which are metabolized5 and supply energy, which is obtained in the form of heat. This capability depends on the presence of abundant mitochondria and the expression of UCP1 (uncoupling protein 1). In addition, it also differs from adipose fat by having significant innervation. Pheochromocytoma, a pathological condition characterized by high adrenergic activation, has been associated with hibernomas,6 and most cases are discovered incidentally on contrast imaging tests, which indicates that the expression of UCP1 can be induced in certain tumors7 and metabolic alterations.8
We describe a case of bilateral perirenal hibernoma discovered during the SPECT-CT 123I-MIBG study of a patient diagnosed with pheochromocytoma.
A 44-year-old patient was evaluated in the outpatient clinic: he reported abdominal pain for the last 5 months, associated with vomiting and sporadic sweating. Antihypertensive treatment was initiated, which provided a partial response. CT scan with contrast showed a right adrenal mass measuring 35mm that was poorly delimited, with heterogeneous contrast uptake and diffuse increased retroperitoneal fat attenuation, involving both perirenal compartments, suggestive of angiomyolipoma. MRI showed massive and symmetric infiltration of both adrenal areas, with a hyperintense signal in T1 and a right adrenal tumor, which confirmed the radiological diagnosis of angiomyolipoma.
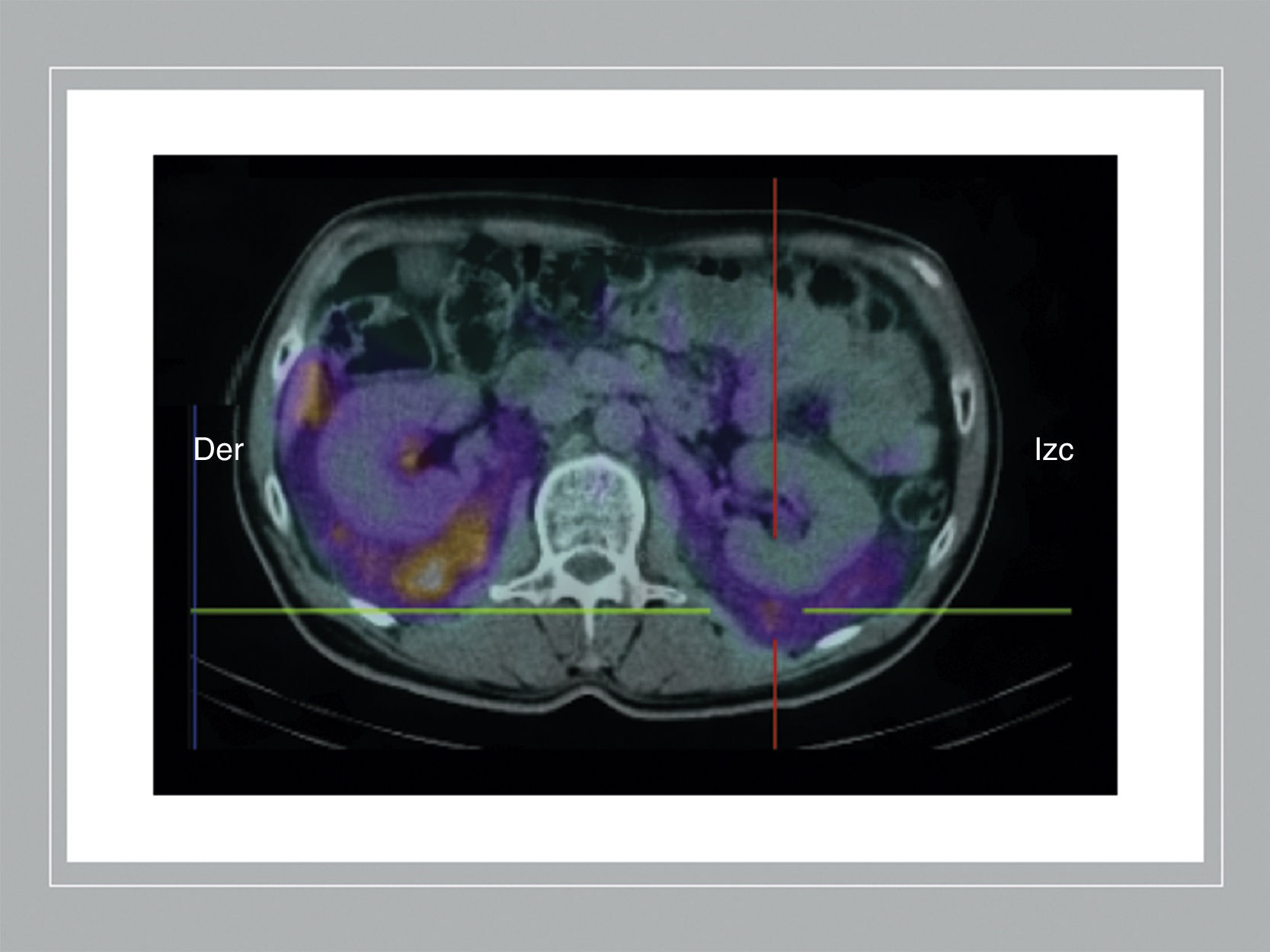
However, blood work-up showed plasma metanephrine levels at 442pg/mL, while urine normetanephrine was 1839μg/24h. Adrenaline, noradrenaline and dopamine levels in urine were normal. SPECT-CT 123I-MIBG study showed moderately intense, diffuse, symmetric, bilateral uptake of radiopaque contrast medium in the perirenal spaces, with a higher density of perirenal fat on each side of the midline, which extended to both iliac crests. Both lesions showed significant drainage in the renal veins. A 4-cm tumor was also detected in the right adrenal gland, suggestive of pheochromocytoma (Fig. 1). Laparoscopic right adrenalectomy and partial removal of brown fat surrounding the adrenal gland were completed successfully.

SPECT/CT 123I-MIBG study: there is evidence of diffuse, bilateral and symmetric uptake of the radiocontrast agent in both perirenal spaces, extending toward the iliac crests. In the right adrenal gland, a nodular image measuring approximately 3.5cm is observed, which does not present pathological uptake of the radiotracer, probably related with the myelolipoma.
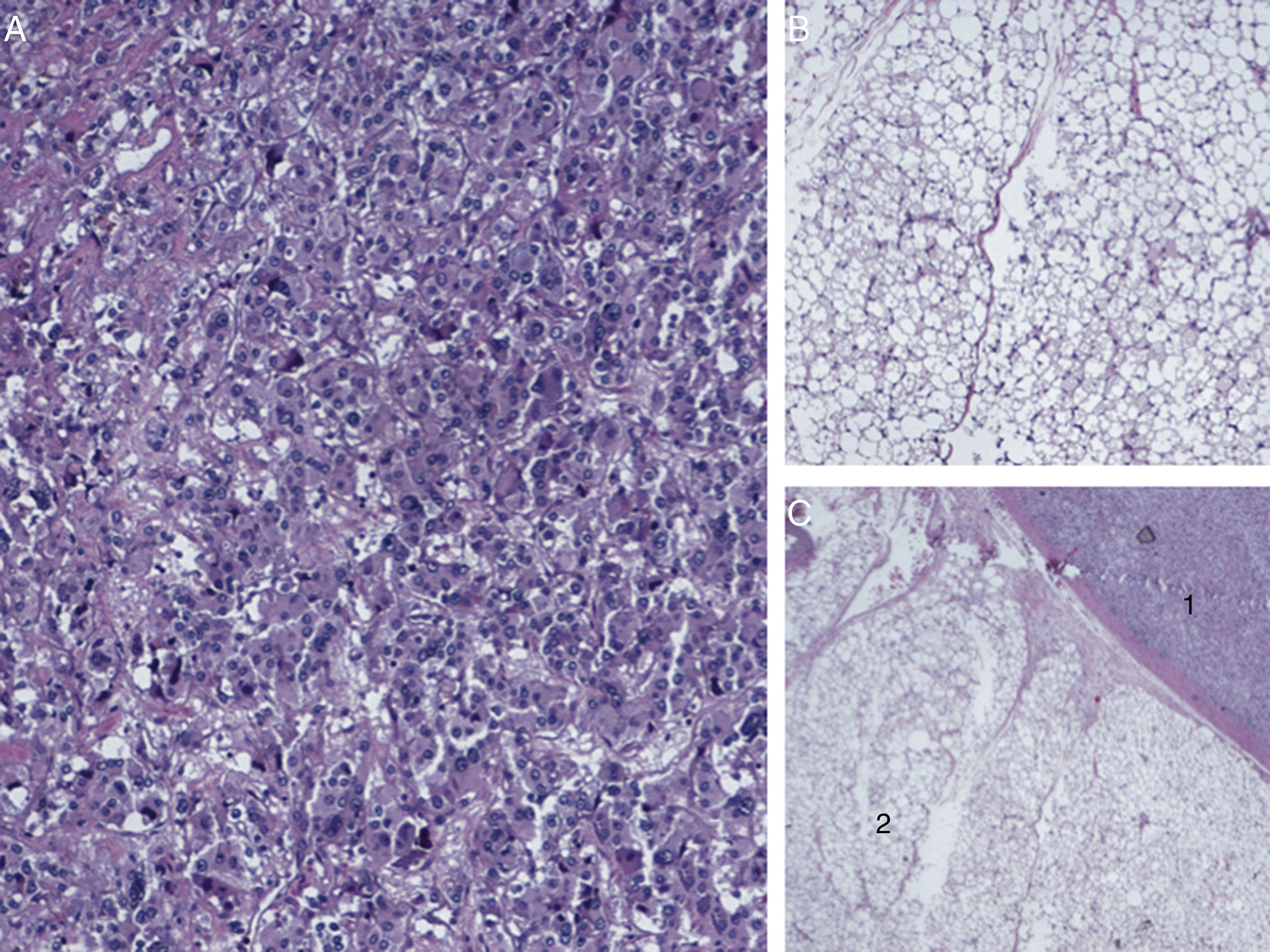
The postoperative period was uneventful, and the patient was discharged on the second postoperative day. The pathology study reported an adrenal pheochromocytoma measuring 3×2×1.5cm. Around the adrenal gland, brown fat was observed with mature adipose tissue, which included large cells with multivacuolated cytoplasm and small central nuclei, compatible with typical hibernoma (Fig. 2). Imaging tests one month later (MRI) showed postoperative changes in the right adrenal fossa and none in the perirenal spaces, with complete disappearance of contrast uptake. At follow-up one year after surgery, the patient remains with controlled blood pressure and normal urine catecholamine levels.
 histology sections (20×) with hematoxylin–eosin (HE), compatible with pheochromocytoma; (B) sections (20×) with HE showing multivacuolated brown fat cells with abundant granular cytoplasm and small central nucleus: these findings were consistent with the diagnosis of hibernoma (typical variant); (C) histology sections (10×) with HE showing the contiguity of brown fat tissue (1) and pheochromocytoma (2).")
Pathology report: (A) histology sections (20×) with hematoxylin–eosin (HE), compatible with pheochromocytoma; (B) sections (20×) with HE showing multivacuolated brown fat cells with abundant granular cytoplasm and small central nucleus: these findings were consistent with the diagnosis of hibernoma (typical variant); (C) histology sections (10×) with HE showing the contiguity of brown fat tissue (1) and pheochromocytoma (2).
The difference between brown fat and normal adipose tissue is not simply based on morphology or distribution. The brown fat of hibernomas is more vascularized and presents certain important biochemical differences, such as a higher content of phospholipids9 and a higher saturated fatty acid composition.10 The first study of the relationship between a pheochromocytoma and a hibernoma was in 1957, when pericapsular adrenal brown fat was found in 2 samples of the 18 cases of pheochromocytoma.
In our study, we have observed that the appearance of hibernoma is not limited to the proximity of the adrenal gland, but may be present in other places, or even appear bilaterally. It is accepted that sympathomimetic hormones play an important role in the metabolism of fatty tissue. A marked increase in hormone-dependent metabolism could be captured by imaging tests with contrast media, such as 123I-MIBG, as in our patient. In conclusion, this is the first case that describes the disappearance of a hibernoma after the resection of a concomitant pheochromocytoma and the return of serum catecholamine levels to the normal range.
Please cite this article as: Lévano-Linares DC, Ruiz-Tovar J, García Muñoz-Najar A, Familiar V, Durán Poveda M. Un caso raro de hibernoma retroperitoneal bilateral identificado por 123I-MIBG SPECT/TC en un paciente con feocromocitoma unilateral. Cir Esp. 2018;96:595–597.
