





Aneurysms of the iliac vessels are relatively uncommon, representing 0.4%–7%1 of abdominal aneurysms. The symptoms caused by this entity are related to vascular symptoms, such as pain or hemodynamic alterations. The clinical symptoms of constipation and intestinal obstruction secondary to extrinsic compression of the colon or rectum by a vascular mass are extremely rare.
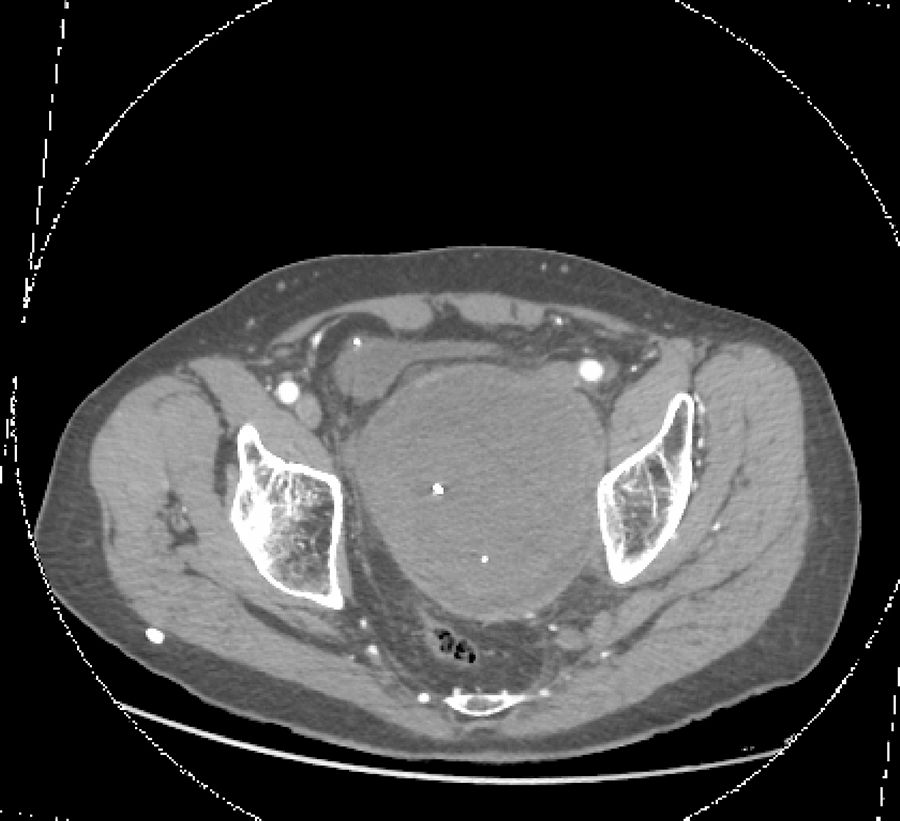
We present the case of a 71-year-old male patient who had been diagnosed 2 years earlier with abdominal aortic aneurysm and thrombosed left hypogastric artery aneurysm, treated with aortic–aortic bypass and ligation and exclusion of the latter. One year later, due to pain in the left iliac fossa, an endoleak of the hypogastric aneurysm was discovered; the sac was closed and embolized using interventional radiology (coils and biological glue), a procedure that needed to be repeated 8 months later for the same reason. Three months later, the patient consulted in the emergency department, this time for symptoms of constipation (but no difficulties for eliminating gas from the anus) and oliguria in the previous 3 weeks, with no other symptoms. A pelvic mass was palpated by rectal examination, which was compressing the rectal ampulla on the anterior and left sides; it was not pulsatile, suggestive of extrinsic compression, with no pathological products. Abdominal radiography showed mild dilatation of a few small intestine loops and the colon up to the descending colon. Ultrasound and angio-CT were performed, which demonstrated a pelvic mass compatible with a large thrombosed aneurysm of the left hypogastric artery filled with coils, which was compressing the rectum and bladder, and mild left hydronephrosis (Fig. 1). The patient was scheduled for surgery. Through an abdominal incision, the peritoneum was retracted until the retroperitoneum was reached. An incision was made in the aneurysmal sac and the contents were extracted and cleaned, and a bleeding point in the sac was sutured as well (Fig. 2). On the first postoperative day, the patient was re-operated due to bleeding in the psoas muscle, and hemostasis was achieved. Pulmonary thromboembolism was also diagnosed, requiring the placement of a temporary filter in the vena cava and anticoagulation with low-molecular-weight heparins. Afterwards, the patient progressed favorably and was discharged.
.")
.")
Aneurysms of the iliac system usually occur more frequently in the common iliac vessels and usually as multiple aneurysms.1 Isolated aneurysms of the internal iliac artery are rare (2%–7% of abdominal aneurysms1–3). Many are due to arteriosclerosis, although it has been suggested that the replacement of an aortic aneurysm with a graft predisposes patients for hypogastric artery aneurysms.3 These are more frequent in older men. Urinary symptoms may appear as a result of the extrinsic compression on the bladder or ureters, or due to perianeurysmal fibrosis.4
Intestinal symptoms derived from this disease are uncommon, and may be due to intestinal adhesions or stenosis after the surgery of the aneurysm, postoperative intestinal ischemia, or bowel obstruction due to extrinsic compression.5 This last mechanism is extremely rare, and only 4 cases2,3,6–10 have been reported in the consulted literature. It should be suspected in patients with constipation and a pulsatile mass during digital rectal examination, although this sign is only found in 55% of internal iliac artery aneurysms.1 This was not the case in our patient since the aneurysm was already thrombosed and treated endovascularly.
Endovascular treatment or surgery is recommended (resection, ligation of arterial branches and vascular reconstruction), since its natural course is progressive expansion and rupture.2 In fact, when the latter occurs, there is high mortality, since they are usually located deep within the pelvis and difficult to resolve during bleeding. In our patient with bowel obstruction due to mass effect, repeating the endovascular treatment did not make sense, so we opted for surgery. This disease must be considered in the differential diagnosis of intestinal obstruction. They should be considered abdominal emergencies, and elective surgery should be performed in those that are 3.5cm in diameter.3
Please cite this article as: Gil Vázquez PJ, Gutierrez García F, Olivares Ripoll V, Ferreras Martinez D, Cánovas López SJ. Obstrucción intestinal secundaria a aneurisma de arteria hipogástrica. Cir Esp. 2018;96:593–595.
